
Abstract
Background:
The management of nondisplaced femoral neck fractures (FNFs) has evolved, with emphasis in radiographic features such as posterior displacement. However, the role of advanced imaging in this scenario is still not well defined. Therefore, our objective is to assess the impact of a computed tomography scan (CT) on interobserver agreement (IA) of fracture classification, posterior tilt measurement, and treatment decisions in nondisplaced FNF in elderly patients.
Methods:
Eleven patients with a nondisplaced (Garden 1–2) FNF were assessed by six hip surgeons. On a first stage, fracture classification, posterior tilt, and treatment plan (fixation/arthroplasty) were determined only with clinical information and X-rays. On a second stage, a CT was added. The kappa coefficient (κ) and intraclass correlation coefficient (ICC) were used to determine IA.
Results:
IA for Garden classification was only slight in X-rays and with the addition of a CT, with a κ = 0.13 (0–0.28) and 0.18 (0.03–0.33), respectively. Conversely, posterior tilt measurement agreement was excellent in both schemes, with an ICC = 0.92 (0.83–0.98) and 0.92 (0.82–0.98). The IA for the proposed treatment was slight with X-rays (κ = 0.44; 0.29–0.6), but moderate with the addition of a CT scan (κ = 0.67; 0.52–0.82). Changes in surgical decision where made in 14 of 66 evaluations with an OR = 1.4 (0.62–3.2) for choosing an arthroplasty if a CT was used.
Conclusion:
IA for fracture classification and posterior tilt evaluation in nondisplaced FNF was not altered by the usage of a CT. There is improvement in treatment agreement when a CT scan is added to conventional imaging, with changes in treatment in 21% of cases.
Introduction
Femoral neck fractures (FNFs) in the elderly patient are a frequent and complex scenario worldwide. 1 They can lead to severe morbidity, 2 carry an enormous economic burden, 3 and are associated with a high risk of mortality. 4 Thus, the adequate surgical management of these patients and a safe rehabilitation free of complications have become a significant topic of interest for both orthopedic surgeons and geriatric/internal medicine-related specialists. 5
Generally, FNFs in the elderly patient are classified according to the Garden Classification 6 and are divided upon displacement in nondisplaced (Garden 1–2) or displaced (Garden 3–4), depending on the anteroposterior (AP) X-ray of the pelvis. According to this, treatment for nondisplaced FNF frequently consists in fixation with the use of cannulated screws or a dynamic hip screw, whereas a total or partial hip arthroplasty is generally performed in displaced fractures. 6 –8 Recently, several authors have proposed that a posterior tilt measured on the lateral X-ray of the hip significantly enhances the risk for complications, and therefore a hip arthroplasty should be considered in a selected group of patients in order to improve the clinical outcomes such as satisfaction, pain relief, and reoperations. 9 –11
The use of a computed tomography scan (CT) has shown to improve agreement in fracture classification as well as increased intraobserver reliability for treatment decisions in several types of fractures, including tibial plateau and distal radius fractures. 12,13 This is especially relevant in scenarios where plain X-rays are considered to be difficult to assess, allowing a better understanding of the fracture pattern, an improved preoperative evaluation and, therefore, a better surgical and clinical outcome. Thus, being able to accurately establish which patients with a nondisplaced FNF will benefit from an alternative surgical plan by improving fracture pattern understanding and posterior tilt identification would be of enormous clinical impact.
So far, there are no studies that assess the performance of CT in the preoperative evaluation of nondisplaced FNF and its properties, such as interobserver agreement (IA) for the evaluation of posterior tilt. On the other hand, there is no data on whether its use could alter treatment decisions in these patients considering some of the new recommendations and algorithms mentioned. 14
Consequently, we performed this study to determine IA on fracture classification, posterior tilt measurements, and treatment decisions in nondisplaced FNF in elderly patients, comparing a standard diagnostic approach with only AP and lateral X-rays to this same approach with the addition of a CT. Our initial hypothesis is that the addition of CT scan would result in a better agreement on fracture understanding and could change evaluation and management of nondisplaced FNF in the elderly patient.
Patients and methods
This study was approved by the institutional ethics review board of our institution. We collected and analyzed the data of 11 patients with an acute low energy FNF, classified as Garden 1 or 2 who had a complete imaging set from an extensive database of elderly patients with hip fractures between 2010 and 2015. We excluded patients younger than 65 years old, bilateral, or pathological fractures and high-energy trauma patients.
One of the authors, who did not act as an evaluator, gathered all the data that were necessary to perform the assessment and corroborated inclusion criteria and diagnosis of patients with the aid of an independent panel of assessors. The data included clinical information (age, gender, mechanism of fracture, comorbidities, actual and previous general status, and physical examination findings), radiographs (including an AP and cross-table view of the hip), and a CT scan including axial oblique reconstructions.
The information from each of the 11 patients was sent to six expert hip surgeons who are regularly engaged in the management of FNF, all of them blind to patient’s identity, diagnosis, and definitive treatment.
On an initial stage, each evaluator received a digital versatile disc (DVD) containing a clinical vignette including all information gathered and the patients’ X-rays. For assessment purpose, all patients were stable and fit to be subjected to any proposed treatment. The six evaluators were asked to classify the fracture according to the Garden classification and to measure the posterior tilt on the lateral X-ray view (Figure 1). Finally, the evaluators were asked to choose one of the following treatment plans for each patient based on the available clinical and radiologic information: to perform a fixation or an arthroplasty. IA was determined by comparing the responses of the six evaluators.

A 72-year-old female with a right femoral neck fracture. (a) APX-ray of the hip; (b) lateral X-ray of the hip with PTA measurement. PTA: posterior tilt angle; AP: anteroposterior.
After 12 weeks, each evaluator was asked to perform the same assessment with the cases in a random sequence to avoid recall bias as reported in other studies. On this stage, a CT of the affected hip was added to the elements provided and posterior tilt was now measured in axial oblique reconstructions (Figure 2). Again, evaluators were asked to choose one of the mentioned treatments considering all the elements in hand. IA was now determined between responses of the six evaluators with the availability of a CT.

A 80-year-old male with a right femoral neck fracture. The (a) AP X-ray of the hip; (b) lateral X-ray of the hip. (c) Axial oblique reconstruction of a computed tomography scan. AP: anteroposterior.
To determine sample size, we considered preliminary intraclass correlation coefficient (ICC) values reported for the posterior tilt angle measured on X-rays by Palm et al. 9 and through the method reported by Walter et al. 15 as follows: assuming six evaluators, defining r0 (minimally acceptable level of reliability) = 0.7 and r1 (expected ICC value) = 0.9, resulted in a minimal sample size of 10 subjects for α = 0.05 and β = 0.2. Therefore, we considered 11 cases for the final patient sample.
Statistical analysis was conducted using the SPSS version 21 (SPSS, Chicago, Illinois, USA). χ 2 or Fisher test was used to compare categorical data and paired t-test for numerical data, after normality verification. ICC was performed for IA of posterior tilt angle measurements because multiple observations of a continuous variable were done as recommended by the GRRAS guidelines. 16 Fleiss’ kappa coefficient (κ) was used to determine the IA for the Garden classification and the proposed treatment strategies as it was designed for the assessment of agreement between multiple raters and a categorical rating. Levels of agreement for ICC were determined as proposed by Fleiss 17 : ICC values <0.40, 0.40–0.75, and >0.75 indicated poor, fair to good, and excellent agreement, respectively. Levels of agreement for κ were determined as proposed by Landis and Koch, 18 with κ values 0.00–0.20 considered slight agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement; and 0.81–1.00, almost perfect agreement. The ICC and κ values are presented with 95% confidence intervals (CIs).
Results
Eleven patients were included with a median age of 77 years (65–89). Four patients were male (36%) and seven female (64%). Regarding classification, 56% of cases (74/132 evaluations) where assessed as Garden 1 and 44% (58/132 evaluations) as Garden 2.
The mean posterior tilt angle was 14° ± 9.6°. When measured in X-rays, the value was 14° ± 8.5° and 15° ± 10.7° when measured in a CT (p = 0.38).
IA for the Garden classification was slight when assessed both in X-rays and CT, with a κ = 0.13 (95% CI: 0–0.28) and κ = 0.18 (95% CI: 0.03–0.33), respectively. Full IA on the Garden classification was achieved in only one case (9%) when X-rays were used and in two cases (18%) when a CT was added to the diagnosis algorithm. On the other hand, IA was excellent for the posterior tilt angle measurements in X-rays and CT, with a CCI of 0.926 (95% CI: 0.83–0.98) and 0.921 (95% CI: 0.82–0.98), respectively (Table 1).
IA for garden classification and posterior tilt angle.

IA: interobserver agreement; CT: computed tomography.
The interobserver analysis for the proposed treatment strategies showed a full agreement in 55% (6/11) of cases assessed with plain films alone, with κ = 0.44 (95% CI: 0.29–0.6), indicating moderate agreement. When a CT was added to the assessment tools, full agreement was observed in 73% (8/11) of cases, with κ = 0.67 (95% CI: 0.52–0.82), indicating substantial agreement.
Regarding the type of treatment selected, fixation was chosen as the proposed treatment in 77% (102/132) of all evaluations and a prosthetic replacement in 23% (30/132). Cases where an arthroplasty was selected had a more significant posterior tilt angle compared to cases were fixation was selected (26 ± 7° vs. 10 ± 6°, respectively; p < 0.001). In cases where the evaluation was performed only with X-rays, internal fixation was chosen as the treatment of choice in 80% of cases (53/66), while in 20% (13/66) of evaluations, an arthroplasty was selected. When a CT was added to the evaluation algorithm, internal fixation was chosen in 74% of cases (49/66), and an arthroplasty in 26% (17/66) (p = 0.4) (Table 2).
Type of treatment selected with the standard evaluation versus the addition of a CT.
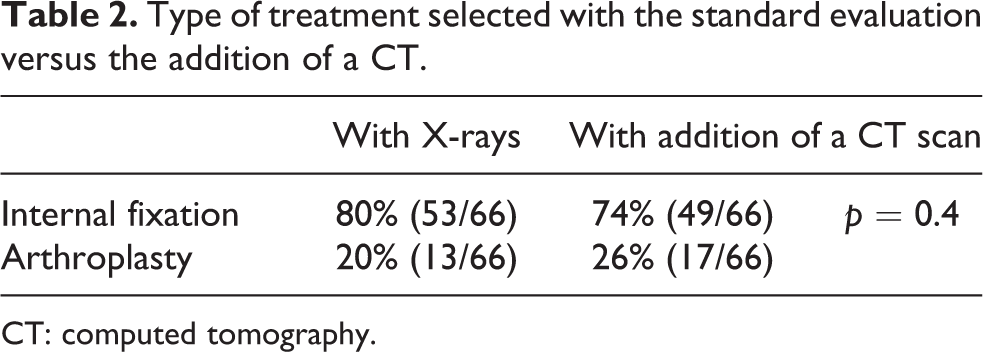
CT: computed tomography.
Changes were made on proposed surgical treatment with the addition of a CT scan in 21% of evaluations (14/66), most of them, being from internal fixation to an arthroplasty (64% of cases). In the same way, risk analysis showed an OR of 1.4 (95% CI: 0.62–3.2) for choosing an arthroplasty as the treatment of choice when a CT was added to the study algorithm.
Discussion
Adequate surgical management for FNF in the elderly patient remains a controversial topic. Although, traditionally, nondisplaced FNFs in the elderly have been treated with an internal fixation, the high rate of reoperations found in a group of patients with this condition has led to more attention being paid to different factors (such as the posterior tilt angle) that could affect a patient’s functional results, satisfaction, and complications. 11,19 An adequate study algorithm should allow the proper evaluation of these factors, to propose the best possible treatment and to improve clinical outcomes. Thus, to detect how accurately clinicians can identify these factors and how it changes treatment strategies is an essential step in improving overall results.
Our results show an excellent interobserver agreement for the posterior tilt angle measured on X-rays as well as in a CT. However, when this last imaging modality was added to the classical study algorithm with plain X-rays alone, we observed an improved inter-observer agreement for the proposed surgical plan among expert hip surgeons, changing from moderate to substantial agreement. Even more, adding a CT scan changed the proposed treatment in 21% of the cases.
The use of a CT scan has been evaluated in several other studies for various fractures. 12,13,20 –22 On tibial plateau fractures, Chan et al. 12 showed that adding a CT scan to the standard evaluation protocol improved the clinical interpretation of comminution and articular displacement, resulting in a better IA for proposed treatment plan even when fracture classification agreement did not improve. In the same way, results from the study by Katz et al. 13 on distal radius fractures showed improved capacity to detect comminution, quantification of articular gapping, and overall involvement with changes in interobserver reproducibility from moderate to substantial agreement for different treatment strategies.
On FNF, Melvin et al. 23 assessed the use of the CT scan on the IA for the classification and treatment plan for displaced and nondisplaced fractures. Their results showed that the addition of a CT to plain X-rays improved Garden classification agreement, revealing an improved understanding of fracture displacement on those considered to be Garden 3 or 4 FNF. However, treatment agreement was not impacted by the addition of a CT scan for expert hip surgeons or general orthopedic surgeons. On trochanteric fractures, van Embden et al. 21 showed no difference on the AO classification IA nor implant selection with the addition of a CT to standard X-rays assessment. Nevertheless, they value the role of this imaging modality in more challenging fractures in which treatment might need further planning to reduce complication rates.
Our study shows only slight IA for the Garden classification in both X-rays evaluation and with the addition of a CT, similar to what has been reported in the other studies. 23 These results reflect the difficulties that specialists have when trying to differentiate between incomplete or complete but nondisplaced FNF, even with the addition of more advanced imaging modalities. As reported by different authors, 24,25 agreement in Garden classification can be significantly improved when stages 1 and 2 are combined as nondisplaced and compared with stages 3 and 4 as displaced. On the other hand, IA for the posterior tilt angle measurement is excellent both in X-rays and CT scan (ICC = 0.92). These findings agree with previous data reported by Palm et al. 9 on X-ray measurements. These results are extremely relevant, as they reveal valuable information about this measurement validity, especially when it is being considered as an essential element in the decision process and the risk of future complications in case of internal fixation. Nevertheless, it is important to consider that CT evaluation was done with all data available, including axial oblique slices, and not only with selected views. This thorough evaluation improves external validity as it represents what clinicians are faced on a real case scenario, but it could affect IA results. (Figure 2)
IA for the proposed treatment plan for X-rays alone evaluation showed a moderate agreement with a κ of 0.44 and only a 55% of cases with full agreement between all observers. These findings represent an interesting scenario as it reveals that even among expert hip surgeons, there are different opinions on how to treat the same patient with a nondisplaced FNF. With the addition of the CT scan, IA improves to a substantial agreement with a κ of 0.67 and 73% of cases with full agreement between all observers. This improvement in IA can be explained by multiple factors and not only by the measurement of the posterior tilt angle. Among them, a better understanding of fracture displacement, assessment of posterior comminution or gaps in the fracture site could play a role. In the same way, this improvement in agreement of fracture management determined changes on the treatment decision in 21% of cases, mainly with changes from fixation to an arthroplasty once a CT assessment was added to the algorithm. Thus, it is our opinion that a CT assessment should be considered as a complementary tool in this type of cases, especially if there is any doubt that an arthroplasty would be the best treatment for that specific patient.
The optimal treatment for nondisplaced FNF is still a matter of debate. Even when it is generally accepted that nondisplaced FNF are best treated with internal fixation to allow early mobilization and prevent secondary displacement, a higher reoperation rate (up to 10–31%) and long-term daily discomfort has been observed in geriatric population. 19,26 –28 On the other hand, patients with a nondisplaced FNF treated with internal fixation have shown lower satisfaction and functional results than patients with displaced FNF treated with an arthroplasty, probably associated with their higher risk of complications. 19,26 Thus, tools that help us determine individual risk of failure, such as the posterior tilt angle in some series, are increasingly relevant, 9 –11,29 even when some have failed to probe the same results. 30
This study has several limitations. First, we only assessed patients with FNF that were considered to be nondisplaced (Garden type 1 or 2); thus, our results cannot be extrapolated to other patients or fracture patterns. Furthermore, we only assessed IA regarding the proposed surgical treatment and the changes that the addition of a CT produced on these decisions, but we did not assess the reasons for choosing a specific treatment. Therefore, the role that certain factors (like comminution, gap, and even posterior tilt) have on a patient’s treatment decision process is still something that needs further evaluation.
To conclude, IA for fracture classification and posterior tilt evaluation in nondisplaced FNF in elderly patients was not altered by the usage of a CT, with only slight results for classification and excellent for posterior tilt measurements. There is an improvement in treatment agreement when a CT is added to conventional imaging algorithm, with changes in the type of surgical treatment proposed in up to 21% of cases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.