
Abstract
Background
The incidence of femoral neck fracture is increasing as society ages. Different types of cannulated screws can be used for internal fixation of femoral neck fractures, but no screw selection protocol has been determined to reduce the risk of operation failure. This retrospective study aimed to elucidate differences in outcomes between using cannulated compression screws and headless compression screws for fixation in nondisplaced femoral neck fractures.
Methods
Adults aged 18 years and older with non-displaced femoral neck fracture, admitted between February 2016 and January 2022, and received fixation using three screws in an inverted triangle configuration were selected for this retrospective study. After exclusions, patients were separated into four groups based on using different combinations of headed cannulated compression screws and headless compression screws. Postoperative computerized tomography or magnetic resonance imaging was used to evaluate operation failure, defined as nonunion or avascular necrosis of the femoral head.
Results
After exclusions, 153 patients (median age 75.0, range 65.0-85.0) with majority of females (69.9%) were included. While the combination of one cannulated compression screw (CCS) and two headless compression screws (HCS) did not achieve statistical significance compared to other screw configurations (P = 0.073), it still demonstrated the lowest rate of operative failure (0.0%). Age was identified as the only significant factor associated with operative failure (adjusted OR: 1.10; 95% CI: 1.03-1.17; P = 0.004).
Conclusions
No significant differences are found in outcomes between different combinations of cannulated headed compression screws and headless compression screws in an inverted triangle configuration for fixation of non-displaced femoral neck fractures.
Keywords
Introduction
The femur, one of the strongest bones in the body, typically fractures due to high-energy trauma, such as motor vehicle accidents, or low-energy trauma in older adults with osteoporosis.1-3 In the United States, over 250 000 hip fractures occur annually, evenly split between femoral neck and intertrochanteric fractures. 4 A femoral neck fracture not only impairs mobility but may also disrupt blood supply to the femoral head, increasing the risk of avascular necrosis and eventual bone collapse. This significantly impacts patients’ health and quality of life.5,6
Femoral neck fractures are classified into four types based on fracture severity and bone displacement 7 : Garden type I fracture refers to non-displaced and incomplete fracture; Garden type II fracture refers to non-displaced and complete fracture; and Garden III and IV are complete and displaced fractures. Types I and II, though non-displaced, are prone to re-displacement, with a healing rate of 44.3% and a postoperative re-displacement rate of 33-44%.8,9 Treatment options include femoral head arthroplasty, total hip arthroplasty, or internal fixation.10,11 Internal fixation utilizes various screws and plates to stabilize the bone and promote healing.12,13
Cannulated screws, which are hollow and inserted over a guide wire for precise placement, are widely used for femoral neck fractures.14,15 They are classified into two types: cannulated compression screws (CCSs), which are headed, and headless compression screws (HCSs). CCSs are commonly used due to their advantages, including minimal soft tissue damage, reduced blood loss, and ease of use during surgery. 16 However, CCSs may hinder the sliding effect essential for optimal fracture healing, potentially causing a gap at the fracture site 2-3 weeks postoperatively due to bone resorption or malreduction.17,18 Additionally, an increased Pauwels angle can result in higher fixation failure rates with CCSs, leading to complications such as femoral neck shortening, loose fixation, varus deformity, and fracture displacement. 19
The HCS have emerged as a reliable option for internal fixation, especially in articular regions, due to minimal soft tissue irritation and reduced interference. 20 HCS features two sets of threads (distal and proximal) separated by a smooth shaft. The screw’s conical shape, with a larger diameter at the tail and a smaller pitch near the tip, enhances bone contact, holding force, pull-out strength, and shear strength. This design increases joint compression, providing immediate stability to support early mobilization. However, complications such as screw migration and superior cutout can still occur, potentially leading to varus collapse through a distinct mechanism. 20
While both CCSs and HCSs offer varying stability for femoral neck fractures, no standard protocol exists to determine their preferred use. This retrospective study aimed to compare the outcomes of HCS and CCS fixation in nondisplaced femoral neck fractures.
Methods
Study Design and Sample
This retrospective study, conducted in accordance with the STROBE guidelines (Supplemental Material 1), enrolled patients with non-displaced or valgus-impacted fractures in the femoral neck at our hospital between February 2016 and January 2022. Inclusion criteria were: (1) age >18 years; (2) diagnosed with Garden type I or II non-displaced femoral neck fracture; (3) underwent internal fixation using cannulated headed or headless screws in an inverted triangle configuration. Exclusion criteria were: (1) patients with pathological fracture, multiple fractures or stress fractures in the femoral neck; (2) patients with fractures in the ipsilateral femur shaft, femur head, pelvic, and acetabular; (3) patients with previous proximal femur fractures; (4) follow-up less than 6 months; (5) missing data in medical records. The flowchart of sample selection is shown in Figure 1. Flowchart of Patient Selection.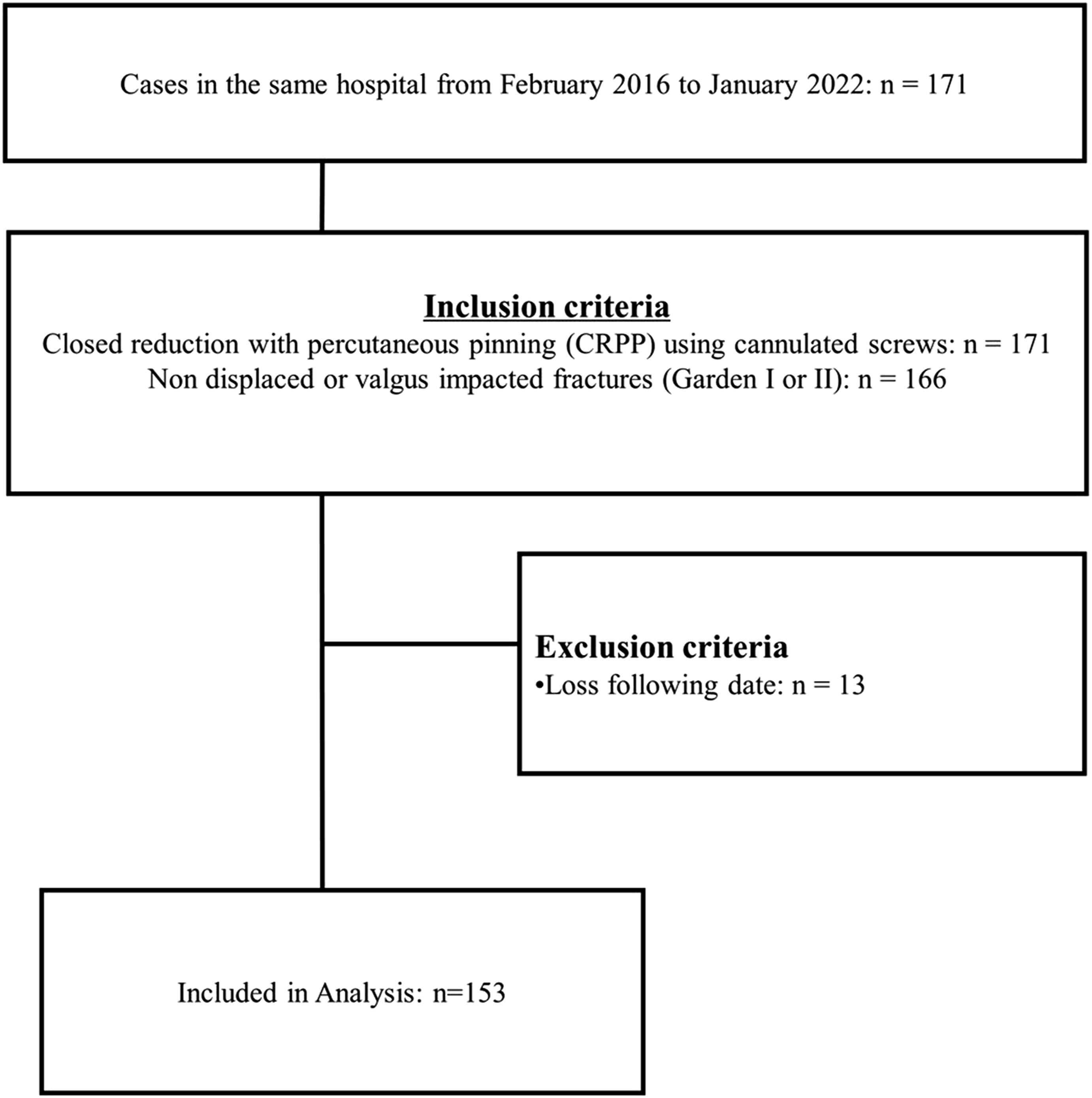
Further, patients were classified into 4 groups by implantation type, as 3 CCS, 2 HCS + 1 CCS, 1 HCS + 2 CCS, and 3 HCS groups for subsequent analysis. The 3 CCS group was assigned as the reference group.
Ethical Considerations
The study protocol was reviewed and approved by the Joint Institutional Review Board of our hospital with registered number N202210074. Because the study design was retrospective, and all patient medical records data were deidentified to protect patients’ anonymity, informed consent was waived by the IRB.
Surgery and Postoperative Management
When admitted to the Emergency Department, all patients underwent a standard radiological protocol of X-rays, including anteroposterior (AP) view of the pelvis and lateral view of the injured hip, as well as computed tomography (CT) scans and image reconstruction. Preliminary management included skin traction or bony skeletal traction to reduce and maintain limb alignment. On admission, demographics and mechanism of injury were recorded.
All surgeries were performed by the same team of surgeons. Screws and combination used for fixation were based on surgeon’s judgement (Figures 2A–D). Two types of screws used were 4.5 mm in thread diameter, partial thread length, and made from 316 L stainless steel (DePuy Synthes, USA). A standard postoperative rehabilitation protocol was followed regardless of the implantation type. All patients were non-weight bearing for at least 8 weeks after surgery. When radiographic and clinical healing appeared to be progressing toward union, weight bearing was advanced slowly from toe touch to partial weight bearing as tolerated over the subsequent 6 weeks, and at the discretion of the treating surgeon. A: X-Ray Image of Screw Implantations (3 HCS). B: X-Ray Image of Screw Implantations (2 HCS+1 CCS). C: X-Ray Image of Screw Implantations (1 HCS+2 CCS). D: X-Ray Image of Screw Implantations (3 CCS).
All patients received routine follow-up. Standard radiographs were obtained at each follow-up visit. Postoperative CT or magnetic resonance imaging (MRI) was utilized at the discretion of the treating surgeon to evaluate for nonunion or avascular necrosis of the femoral head (AVNFH). Complications observed during follow-up were recorded.
Primary and Secondary Outcomes
The primary outcome was operation failure, defined as malunion or nonunion requiring a necessary shift to hemiarthroplasty, total hip arthroplasty (THA) or revision of internal fixation. Secondary outcomes were the occurrence of implant cut out or backout, avascular necrosis of the femoral head, non-union, varus deformity, or periprosthetic fractures during follow-up.
Covariates
Imperative covariates were included to study interest of association, such as age, sex, garden type, and bone mineral density (BMD).
Statistical Analysis
Descriptive statistics of the patients are presented as number (n) and percentage (%) or median and 25th percentile-75th percentile. Comparison of categorical and continuous data between groups were performed. Cox proportional hazard model was performed to identify associations between operation failure time and variables. All P values were two-sided and P < .05 was considered statistically significant. All statistical analyses were performed using the statistical software package SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Demographic & Clinical Characteristics of 4 Groups.
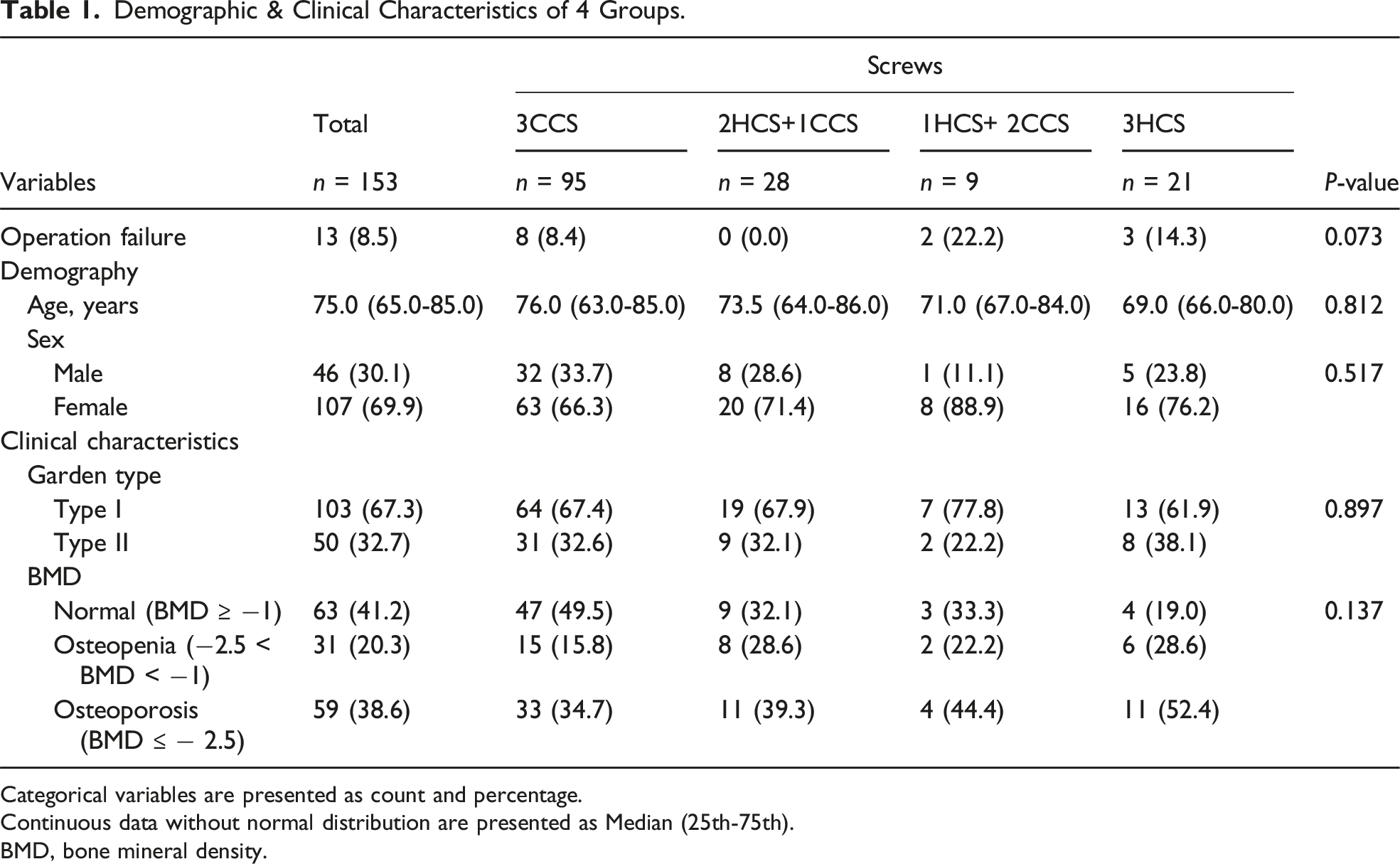
Categorical variables are presented as count and percentage.
Continuous data without normal distribution are presented as Median (25th-75th).
BMD, bone mineral density.
Risk Analysis of Operation Failure.

aHR, adjusted hazard ratio; BMD, bone mineral density.
P-value < 0.05 are shown in bold.
Discussion
The present study showed that risk of operation failure in the fixation of non-displaced femoral neck fracture was the least when using two HCSs and one CCS in an inverted triangle configuration, although no significant differences were shown between different combinations of HCS and CCS in that configuration. Age was shown to be the only factor directly associated with operation failure.
When treating femoral neck fractures with cannulated screw systems, the stability of the fixation construct has been shown to be affected by several factors, including screw type, screw number, screw thickness, along with position, direction and the configuration of screws. 21 Besides, age is identified as a critical factor in femoral neck fracture outcomes; patients ≥ 80 years have a 69% complication rate with cannulated screw fixation, suggesting endoprosthetic procedures should be preferred in this group. 22 A total of 61% of patients experience worsened mobility postoperatively, emphasizing the need for improved surgical selection and postoperative management. 22 A meta-analysis also echoed that internal fixation, the cannulated screw, carries a high failure and reoperation rate, making it appropriate only for young patients with good bone quality. 23 Surgical decisions should be individualized based on age, mobility, and comorbidities, with a multidisciplinary approach to optimize outcomes. 23 Besides, most biomechanical studies agree with the idea that using three screws with diameters larger than 6 mm is ideal.24,25 In the present study, three cannulated screws were used in an inverted triangle configuration to achieve the required stability.
The combination configuration of HCS and CCS is commonly used for complex fractures (e.g., vertical femoral neck fractures, subtalar arthrodesis) which integrates the advantages of HCS’s biomechanical stability and CCS’s dynamic compression.26,27 While combination configuration associated with higher costs and increasing surgical complexity, especially during removal or in revisions, the combination configuration achieves superior outcomes with better fixation and fewer complications such as femoral neck shortening, nail withdrawal, and fixation failures. 27
Maheshwari et al. 28 studied the management of Hoffa fracture fixation using headed and non-headed cannulated screws, and reported no significant differences between the screws in terms of functional outcomes such as range of motion. However, in that study, HCS implantation did reduce the rate of complications and implant failure more than the headed cannulated screws. Meanwhile, Zhang et al. 27 studied the configuration of fixation screws in the treatment of vertical femoral neck fractures, reporting that using one CCS and two HCSs improved the outcomes more than using CCSs alone. Results of that study agree with those of the present study. Together, these studies have shown that HCS provides specific benefits in fracture fixation.
Previous studies have also reported that increased age is associated with increases in revisions, complications, nonunion and poor functional outcomes in non-displaced femoral neck fractures fixation.29-31 Age was also identified in the present study as the only factor that was significantly and independently associated with operation failure of femoral neck fracture fixation. Two studies have reported that older age and being female were the main factors associated with increased risk of healing complications after an osteoporosis-induced femoral neck fracture.32,33 Osteoporosis, or lower bone mineral density (BMD), is known to be a risk factor for femoral neck fracture.34,35 Bruyère et al. 36 reported that in the post-hoc analysis of women undergoing three years of strontium ranelate treatment, an increase in femoral neck BMD was associated with a decrease in hip fracture incidence. Bartels et al. 37 also reported that patients aged 55-70 years with a displaced femoral neck fracture had lower bone density and higher comorbidity compared with a sex- and age-matched population without femoral neck fractures. However, no significant associations were found between low hip BMD and fixation failure in patients with femoral neck fracture treated with internal fixation. 38 Results of the present study also showed that different degrees of BMD representing osteopenia and osteoporosis were also not associated with risk of operation failure. Thus, using the current fixation methodology, BMD has little impact on the outcomes of femoral neck fracture treatment.
Limitations
The present study has several limitations. First, this was a retrospective study with a relatively small sample, which does not allow generalization of results to other populations and selection bias cannot be ruled out. Besides, the unequal distribution of patients across groups—one nearing 100, two around 20, and one with fewer than 10—may impact statistical power and further limit generalizability. Third criteria for implant selection were not clearly defined by the surgeons and the absence of such details may introduce variability in treatment decisions. Additionally, functional outcomes, such as patient mobility and quality of life, were not assessed, limiting our ability to correlate radiographic findings with clinical recovery. Future studies with larger, more balanced cohorts are needed for validation.
Conclusion
In the fixation of non-displaced femoral neck fracture, while the combination of one CCS and two HCSs did not reach statistical significance compared to other screw configurations, it exhibited the lowest rate of operative failure, suggesting its potential as a favorable option for an inverted triangle configuration for fixation of non-displaced femoral neck fractures, with age as a risk factor for failure.
ORCID iD
Meng-Huang Wu https://orcid.org/0000-0003-1606-2444
Supplemental Material
Supplemental Material - Outcomes of Headed and Headless Cannulated Screws Fixation in Nondisplaced Femoral Neck Fracture
Supplemental Material for Outcomes of Headed and Headless Cannulated Screws Fixation in Nondisplaced Femoral Neck Fracture by Ko-Ta Chen, Hsien-Tsung Lu, Chian-Her Lee, and Meng-Huang Wu in Geriatric Orthopaedic Surgery & Rehabilitation
Statements and Declarations
Ethical Approval
The study protocol was reviewed and approved by the Taipei Medical University – Joint Institutional Review Board 1 . Because the study design was retrospective, and all patient medical records data were deidentified to protect patients’ anonymity, informed consent was waived by the IRB of Taipei Medical University. All methods were carried out in accordance with relevant guidelines and regulations in the declaration.
Footnotes
Author Contributions
Ko-Ta Chen: guarantor of integrity of the entire study; study design; experimental studies; data acquisition; data analysis; statistical analysis; manuscript preparation; manuscript review.
Hsien-Tsung Lu: literature research; clinical studies; definition of intellectual content.
Chian-Her Lee: study concepts; manuscript editing; data analysis; statistical analysis.
Meng-Huang Wu: data acquisition; data analysis; statistical analysis; manuscript preparation; manuscript review.
All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.