
Abstract
Purpose:
Displaced two-part fractures of the proximal humerus are generally treated with open plate (OP) fixation. Recently, minimally invasive plate osteosynthesis (MIPO) has been increasingly favored for fracture healing and functional recovery. We aimed to compare OP and MIPO for two-part fractures of the proximal humerus to identify outcome differences.
Methods:
All patients who underwent OP or MIPO for a displaced two-part fracture of the proximal humerus at a single level I trauma center between 2007 and 2013 were retrospectively evaluated. Of the patients, 17 were treated using the OP method through the delto-pectoral approach and 19 with MIPO through deltoid splitting. Radiographic results were evaluated to determine the union rate, time to union, and alignment. Functional outcomes were measured with Constant and UCLA scores. Radiation exposure and operative time were also evaluated.
Results:
All patients achieved bone union without complication. In the OP and MIPO groups, no significant difference was observed in the neck shaft angles, constant scores, or UCLA scores. The OP group required less radiation exposure time than the MIPO group (p < 0.001). However, the OP group showed more operation time than the MIPO group (p < 0.001).
Conclusions:
Both techniques showed satisfactory radiographic and functional outcomes in two-part fractures of the proximal humerus. Although MIPO technique offers advantages, including minimal soft tissue damage and short operation time, surgeons and patients should be warned of the invisible risk from the radiation hazard.
Keywords
Introduction
Two-part fractures are the most common injury among proximal fractures of the humerus. 1 The treatment options for these fractures include nonoperative treatment, percutaneous K-wire fixation, open reduction and internal fixation, intramedullary device fixation, and external fixation.
While minimally displaced two-part fractures can be successfully treated nonoperatively, 1,2 the treatment method is determined on the basis of the fracture pattern and patient factors, including age, functional status, and hand dominance. 3 Nonoperative treatment requires good patient compliance for a successful outcome. On the other hand, operative fixation using the plate is commonly used in two-part fractures, with either the open plate (OP) or the minimally invasive plate osteosynthesis (MIPO) technique.
The OP technique is a popular surgical fixation for proximal humerus fractures, typically through the delto-pectoral approach. 4 However, this approach may cause damage to soft tissue and blood supply, which may lead to potential problems, including injury to the deltoid muscle, increased blood loss, nonunion, avascular necrosis of the humeral head, and infection. 5
Recently, the MIPO technique has been used to fix proximal humerus fractures, using the deltoid splitting approach. As it preserves the soft tissue and periosteum around the fracture, this technique may have advantages to reduce complications of the traditional OP technique. 6 However, it confers a risk of injury of the axillary nerve, as compared to OP fixation. As MIPO is known to have the benefit of fracture healing, it is reported to be a useful method for treatment of three- or four-part fractures of the proximal humerus. 5
However, to the best of our knowledge, only a few reports have compared OP and MIPO for two-part fractures of the proximal humerus. The present study evaluated the differences in radiographic and functional outcomes between OP and MIPO for two-part fractures of the proximal humerus.
Materials and methods
After institutional review board approval (KNUH IRB (Kyung Pook National University Hospital Institutional Review Board); IRB No: KNUH 2016-05-030) was obtained, a retrospective study was performed in all the patients who underwent OP fixation or MIPO for a two-part fracture of the proximal humerus at a single level I trauma center between 2007 and 2013. Patients with pathological fractures, intra-articular fractures, open fractures, or fractures with primary neurovascular damage and those who were lost to follow-up were excluded from this study. After the exclusions, 36 patients were included in this study. Of these patients, 17 underwent OP fixation through the traditional delto-pectoral approach (the OP group) between April 2007 and September 2010, while 19 were treated with MIPO through anterolateral deltoid splitting (the MIPO group) between October 2010 and December 2013. All the operations were performed by a single surgeon experienced in orthopedic traumatology.
The outcome measurements included radiographic fracture healing and function. The radiographic outcomes included union rate, time to union, and alignment. Bony union was defined as the presence of bone-bridging callus in at least three cortices in two planes. Alignment was evaluated on the basis of a neck-shaft angle (NSA) of 135° (range 125°–145°) from the anteroposterior (AP) view (Figure 1) and anterior or posterior angulation from the lateral view. Malalignment was defined as an NSA of <125° or >145° at AP view or an angulation of >10° at lateral view. Functional outcomes were assessed, including scoring systems that reflected shoulder function (Constant and UCLA scores), at the 12-month follow-up.

The NSA was measured by drawing a line from the superior to the inferior border of the articular surface and then a perpendicular line through the center of the humeral head. The angle between this line and the line bisecting the humeral shaft was measured as the NSA. NSA: neck-shaft angle.
In addition, radiation exposure and operation time were compared as demographics of surgical procedures. Radiation exposure time was defined as the duration of fluoroscopy use, and operation time was defined as the time from skin incision to closure. Three orthopedic surgeons who did not perform the operation measured and evaluated the radiographic and functional outcomes.
Operating techniques
In both the OP and MIPO groups, patients were placed in a supine position, with the affected arm prepared to permit intraoperative mobilization. The fluoroscope was positioned to allow visualization of the proximal humerus in two axes. All the procedures were performed under general anesthesia.
Open plating
The delto-pectoral approach was used. An approximately 10- to 15-cm incision was made, starting at the tip of the coracoid process and running laterally in the direction of the insertion of the deltoid muscle. After the fracture was reduced, a Philos plate (Synthes®, Oberdorf, Switzerland) was placed 2–4 mm lateral to the bicipital groove and 5–7 mm distal to the tip of the greater tubercle. The plate was first fixed to the distal fragment, and then screws were inserted in the head according to the woodpecker technique. At the proximal part of locking plate, we fixed at least six locking screws and at least three bicortical screws at the distal part (Figure 2).
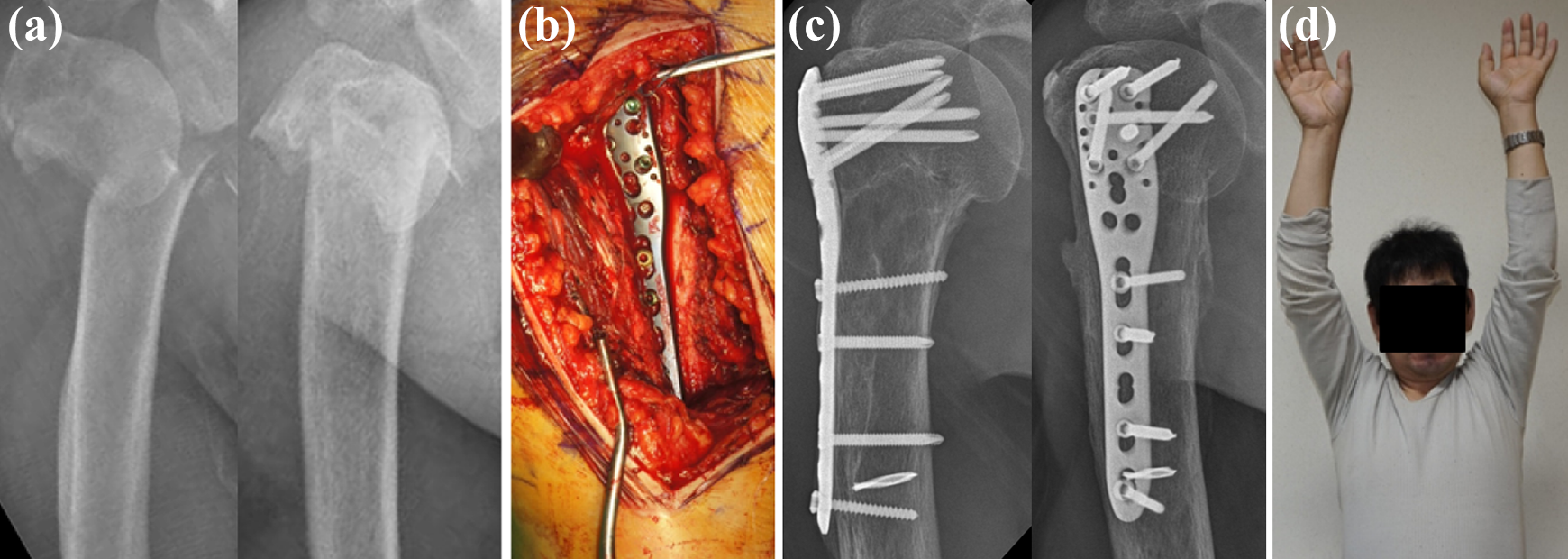
A 56-year-old man with a two-part fracture of the proximal humerus. Open plating group: (a) AP and lateral radiograph at accident; (b) intraoperative gross photo; (c) AP and lateral radiograph at 28 months after surgery; (d) gross photo of range of motion at 12 months after surgery. AP: anteroposterior.
Minimally invasive plate osteosynthesis
The deltoid splitting approach was used. Beginning at the anterolateral tip of the acromion, the proximal incision was extended approximately 5 cm distally, deep to the level of the deltoid muscle. A distal incision was made 2 cm distal to the first incision. The skip area between the two incisions contained the axillary nerve and was considered the unsafe zone. Reduction was achieved by applying axial traction on the humerus or by various techniques of indirect reduction, such as a joystick with pins or plate-induced reduction. The plate position and screw fixation was the same as that in the OP group (Figure 3). After the operation, the patient’s arm was supported with a neck sling for 2–4 days. As soon as pain subsided, shoulder and elbow motions were started.
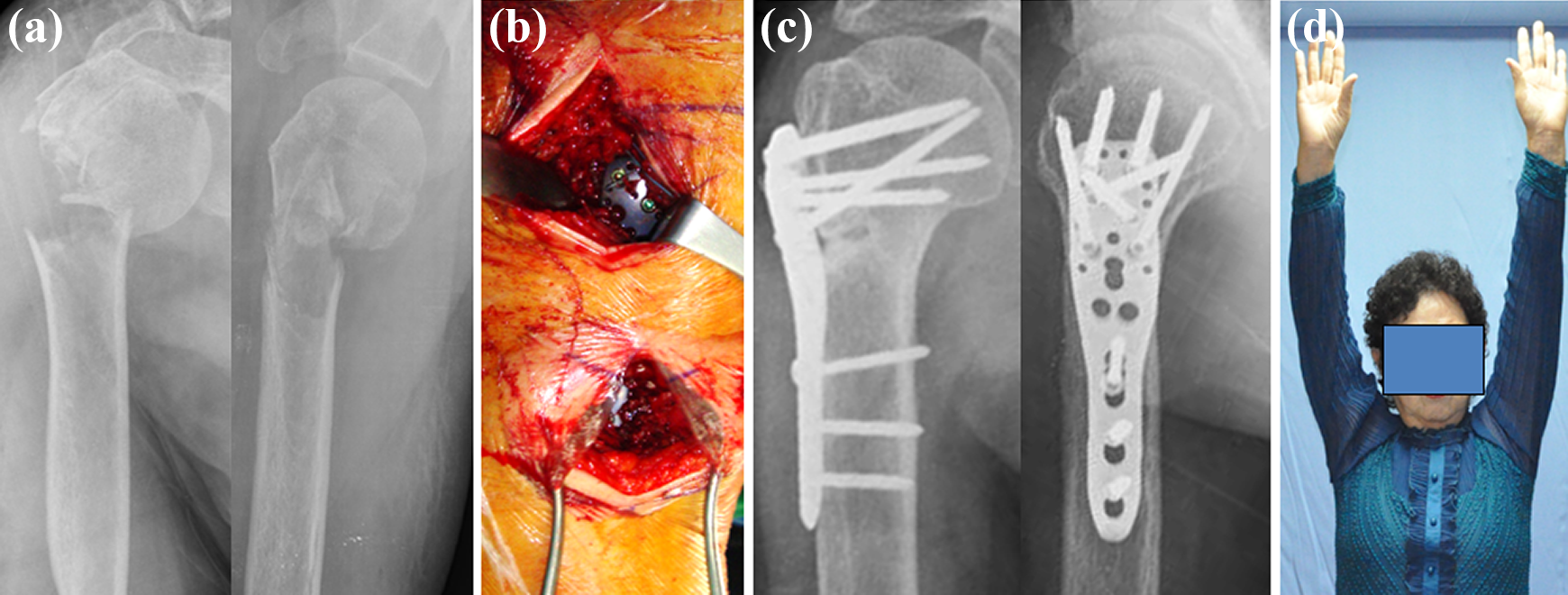
A 52-year-old woman with a two-part fracture of the proximal humerus. MIPO group: (a) AP and lateral radiograph at accident; (b) intraoperative gross photo; (c) AP and lateral radiograph at 12 months after surgery; (d) gross photo of range of motion at 12 months after surgery. MIPO: minimally invasive plate osteosynthesis; AP: anteroposterior.
Statistical analysis was performed using PASW Statistics version 18.0 for Windows. Mann–Whitney tests were used for data that were not normally distributed. The χ 2 tests were used for categorical data. The values of p < 0.05 were considered statistically significant.
Results
The mean age of the participants was 52.6 years (range 23–72 years) in the OP group and 58.7 years (range 20–80 years) in the MIPO group. In all the cases, the minimum follow-up period was 24 months. According to the AO/OTA classification system, the most frequent fracture was type A3 (n = 32; 88.9%), followed by type A2 (n = 4; 11.1%). No significant differences in patient demographics and injury characteristics were found between the two treatment groups.
In radiographic outcomes, all patients in both groups achieved bone union, without delayed union or nonunion. The mean times to union were 15.6 weeks (range 13–18 weeks) and 14.9 weeks (range 12–20 weeks) in the OP and MIPO groups, respectively (p = 0.465). The mean NSA was 137.8° (range 129°–149°) in the OP group and 133.8° (range 115–148°) in the MIPO group (p = 0.102). Except for three patients, all patients healed with less than 10° of angular deformity. Three patients showed malalignment of more than 10° of angular deformity at AP view, one in the OP group (valgus 149°) and two in the MIPO group (valgus 148°; varus 115°). The operative and intraoperative outcomes are summarized in Table 1.
The outcomes of patients with proximal humeral two-part fractures.
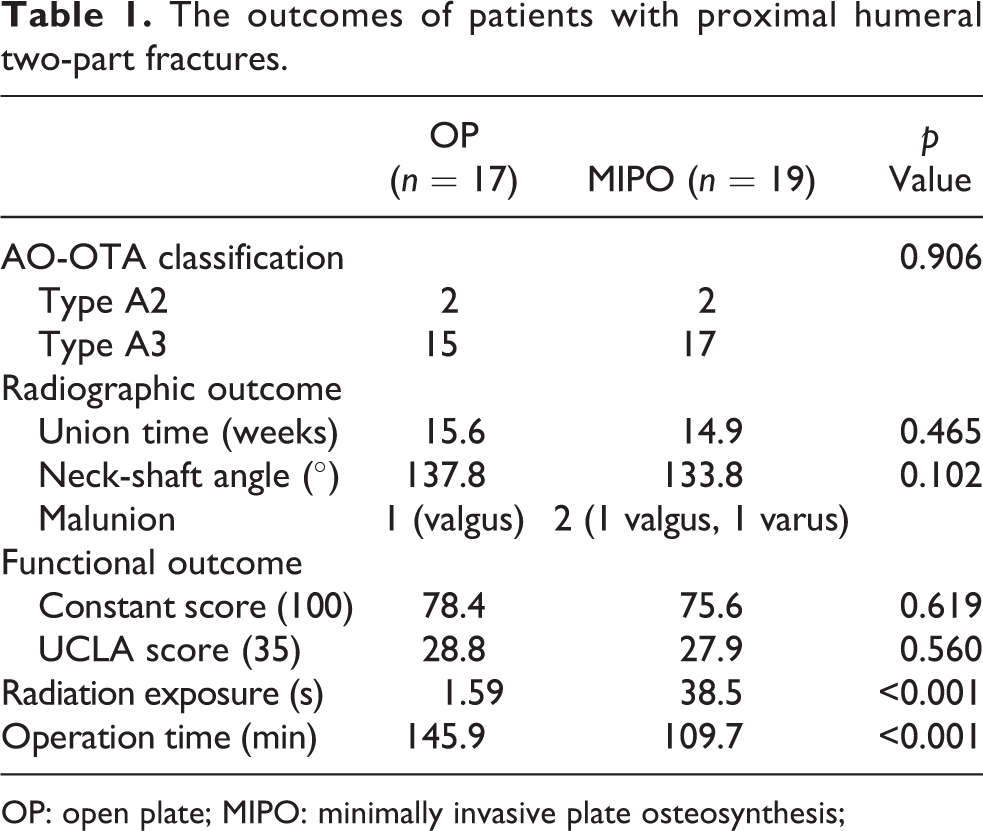
OP: open plate; MIPO: minimally invasive plate osteosynthesis;
In functional outcomes, the mean constant scores were 78.4 in the OP group and 75.6 in the MIPO group (p = 0.619). The mean UCLA score was 28.8 and 27.9, respectively (p = 0.560).
The mean radiation exposure time was 1.59 s (range 0.5–2.4 s) in the OP group and 38.5 s (range, 32.2–45.7 s) in the MIPO group (p < 0.001). The mean operation times were 145.9 min (range 136–154 min) and 109.7 min (range 98–120 min), respectively (p < 0.001). Statistically significant differences in radiation exposure and operation time were found between the groups. No major complications, including nonunion, deep infection, and neurological injuries, occurred in either group.
Discussion
We compared the result of MIPO with that of the traditional OP method. As indicated by our results, bony healing occurred at a high percentage, in both groups, and the functional outcomes were excellent on the basis the constant and UCLA scoring system. Therefore, we believe that MIPO is a safe and effective method for the treatment of two-part proximal humerus fractures.
Many studies have analyzed the surgical approach and their outcomes for proximal humerus fractures. MIPO is commonly believed to provide advantages of fracture healing, as it preserves the periosteum and soft tissue. 7,8,9 Lin et al. reported no significant difference between OP and MIPO in the union rate for all types of fractures of the proximal humerus. 5 Recently, MIPO for proximal humerus fractures was reported to have similar radiographic and functional outcomes compared to those of OP. 10 Nonunion is rarely a problem in two-part fractures of the proximal humerus, 11 managed by either the OP or the MIPO technique.
Generally, malalignment with resulting malunion or nonunion is a common complication of MIPO surgery, 12,13 as it mainly depends on indirect reduction of the fracture without exposing the fracture site. However, no significant difference in malrotation was found between the two groups in this study. We assume that in two-part fractures, unlike in three- or four-part fractures, reduction is relatively easy to attain. The rotational alignment of the union was evaluated through comparison with the radiographic measurements and range of motion of the healthy side. However, this may be one of limitations of this study, as accurate rotation should be evaluated by CT scanning.
As MIPO is less invasive than OP, it was thought to have a superior outcome in terms of shoulder function. In previous reports, 5,13,14,15 functional scores were excellent after operation using either technique, similarly to the findings of our study. As the soft tissue suffers a relatively small injury from the two-part fracture, we assume that non-injured muscle and soft tissue may successfully restore the function of the shoulder joint, regardless of the chosen surgical approach.
Paradoxically, repeated use of fluoroscopy may be needed to attain an acceptable closed reduction in MIPO. In the present study, the radiation exposure was 38.5 s in the MIPO group, which is higher than that in the OP group. Similarly, the mean radiation exposure time for a humerus shaft fracture was 68 s in the MIPO group 16 and 142 s in another study. 17 Repeated use of fluoroscopy would prevent malalignment, but this might increase the radiation exposure time. As the longer radiation exposure time is a major drawback of the MIPO technique as compared to the OP technique, surgeons should be cautious about the radiation hazard during the operation.
MIPO needed a significantly shorter operation time than OP, as reported in previous studies. 4,16 The difference in surgical approach is the most likely explanation for this finding. In contrast to the delto-pectoral approach, the deltoid-splitting approach can provide sufficient vision of the plate location, while requiring only minimal soft tissue dissection. The shorter operation time of MIPO is certainly an advantage over OP, as the fracture is often accompanied by other traumas that require surgery.
In the present study, the MIPO technique had advantages of small scar size and shorter operation time but had a disadvantage of high radiation exposure time. On the other hand, the OP technique had advantages of less radiation exposure and easy fracture reduction; however, it had disadvantages of large scar size and longer operation time. Orthopedic trauma surgeons may consider using this time-saving procedure for polytrauma patients with multiple fractures (Table 2).
Comparison of considering factors in determining the surgical method between the OP and the MIPO.
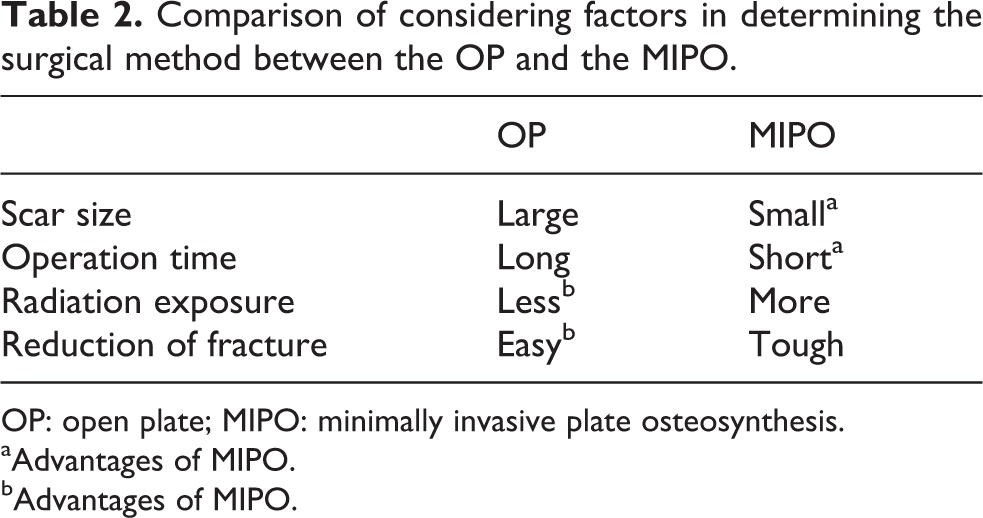
OP: open plate; MIPO: minimally invasive plate osteosynthesis.
aAdvantages of MIPO.
bAdvantages of MIPO.
Several limitations of our study must be addressed. First, this was not a prospective study and randomized controlled trial. Second, the number of cases included in the study was relatively small, and the follow-up period may be insufficient. Further prospective studies with a larger sample size may need to be performed. However, the baseline characteristics of the patients in the two study groups were similar with respect to age and fracture classification. Finally, because this study was performed by a single surgeon, there might be a bias including radiation exposure time and operation time. Although the surgeon was experienced, a potential for bias was present because the radiation exposure and operation times can be different depending on the operator. However, this study is valuable as all patients were treated by a single surgeon with a standardized surgical approach and postoperative rehabilitation.
Conclusion
On the basis of the results of this study, either the OP or the MIPO technique can be effectively used to fix two-part fractures of the proximal humerus, with satisfactory radiographic and functional outcomes. Although the radiation exposure in MIPO was much more increased than that in the OP technique, MIPO offers advantages, including minimal soft tissue damage and shorter operation time. In conclusion, we believe that MIPO is equivalent to the traditional OP as a safe and effective method for two-part proximal humeral fractures, with the advantage of shorter operation time.
Footnotes
Author contributions
Young-Gun Kim and Kyeong-Hyeon Park contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by AOTrauma Asia Pacific of AO Foundation (no. AOTAP 16-17).