
Abstract
Purpose:
Ankle Charcot neuroarthropathy presents a great challenge for treatment. While conservative treatments yield poor results, arthrodesis is considered the treatment of choice for unstable Charcot ankles. There are two methods used for ankle fusion: retrograde intramedullary nail (IMN) and external fixator (EF). Literature reports inconclusive results on which method is better for arthrodesis.
Methods:
The aim of this meta-analysis is to look for significant difference between the two techniques in terms of fusion rate and complications. Four comparative studies including 117 patients (117 interventions) were located and analyzed.
Results:
IMN was found to yield double fusion rate than EF (p = 0.2) with 5 weeks less time to heal (p = 0.4). While no significance was noted for revision surgery and amputation rates, EF yielded higher rates of hardware infection (p = 0.01) and wound infection (p = 0.01). The IMN method seems to offer quicker and better fusion rate when compared to EF with significantly lower postoperative infection rates.
Conclusion:
In the clinical context of high-risk patients such as the diabetic population, IMN technique could be a better option in the case of ulcer-free ankles/feet or in the presence of medial/lateral ulcers. In case of presence of plantar ulcers, EF might be a better choice to avoid the plantar approach for nail insertion. Future research with bigger sample sized and randomized studies are warranted for validation.
Introduction
Charcot neuropathic osteoarthropathy or neuroarthropathy (CNO) of the foot and ankle constitutes a great clinical challenge for a poorly understood destructive process. 1 Neuropathic arthropathy could have many etiologies, but the leading cause is diabetic neuropathy. 2 The CNO is due to sensory and motor neuropathies which lead to a chronic and progressive destruction of the foot architecture involving bones, joints, and soft tissues. 3
Secondary fractures and dislocations predispose to deformity and ulceration with a great decrease of the gait-related quality of life and an increasing potential for major amputation. 2,4 The goal of treatment is to achieve a plantigrade foot with osseous stability. 5 Offloading devices such as total contact casting, Charcot restraint orthotic walker devices, and bracing are usually used in the initial treatment of CNO. 6 Contrary to the foot Charcot neuroarthropathy, involvement of the ankle is most likely to lead to progressive deformity poorly responding to nonoperative management. 7 In fact and unlike the good results reported for Charcot arthropathy of the midfoot, those of the ankle are found to be far inferior. 7,8
Fusion is usually the surgical treatment which is indicated in severe, progressive, unstable deformity of the hindfoot. 9 The aims of the arthrodesis reconstructive procedure are realignment and stabilization of the severely deformed ankle in order to avoid ulcers and amputation. Retrograde intramedullary nails (IMN) and ring external fixators (EFs) are two of the most common fixation techniques used for arthrodesis in CNO. Proponents of EF argue that this method limits soft tissue trauma in a population with vascular compromise and poor wound healing potential. 10 Additionally, since no cast is usually required following ring fixator, swelling and ulcer recurrence could be monitored. 7 On the other hand, advocates of retrograde nails cite the high incidence of pin tract infections, risk of tibia fracture, and the need for a second surgery for EF removal as reasons to choose a nail over external fixation. 11,12 No evidence synthesis on the comparative efficacy of both methods is yet reported in the literature. Therefore, the aim of this systematic review is to collate evidence from comparative studies to look for significant differences in terms of fusion rate, salvage rate, and complications following EF and IMN techniques for tibiotalocalcaneal arthrodesis.
Methods
Search strategy
The electronic search strategy included the following databases: PubMed, Embase, Cochrane Library, and Google Scholar, and that from inception to June 2018. Specific Boolean terms were used: (Charcot OR neuroarthropathy) AND (fusion OR arthrodesis) AND (foot OR ankle). No language or date limitations were imposed.
Criteria for study selection
Papers reporting the primary outcome were selected for inclusion. Cohort studies, review articles, and case reports were excluded. Only studies with comparative design were included. Studies reporting outcomes on tibiocalcaneal arthrodesis were excluded.
Screening and selection of literature
One reviewer (KY) screened all retrieved studies. After deletion of duplicates, title checking was first initiated followed by independent abstract screening by two reviewers. Abstracts which were found to be likely relevant had their full manuscripts retrieved. Reference list of every included study was checked for any additional potentially relevant articles. Disagreement on eligibility was resolved by consensus.
Types of outcome measures
The primary outcome was set as the radiological fusion healing rate. Secondary outcomes were defined as time to heal, revision surgery, hardware infection, wound infection, and amputation rate. It is anticipated that not all cases of nonunion were revised; in the case of revision due to symptomatic nonunion, such outcome has been reported separately.
Data collection
In preparing this review, we adhered to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. 13
Data extraction
A data extraction sheet was used to record all relevant data of the included studies. Initially, one author (KY) extracted the data, which was later reviewed jointly to produce agreed accurate data. Disagreements were resolved by consensus. Predefined demographic data of the patients were extracted. Data on Charcot stage, preoperative ulcer or infection status, and follow-up duration were recorded.
Quality assessment
The quality of the studies was assessed to detect potential sources of bias from the study design using The Joanna Briggs Institute (JBI) critical appraisal checklist for case-control studies. 14
Data analysis
Proportion meta-analysis was used to look for weighted frequencies of outcomes in each study. The weighted risk difference (RD) was used to compare weighted outcome frequency difference. For continuous variables, the unpaired t-test was used to look for significance between the two groups. Heterogeneity was assessed by the inconsistency test (I 2). Since the number of included studies was small (less than 5), the fixed-effect estimate was reported. StatsDirect (Cambridge, UK) software was used to compute the statistical analysis.
The study of Ettinger et al. 15 was the only study where patients’ infection status dictated the use of one method over the other (all patients with infected and noninfected ulcers were treated with EF while all others with IMN). Therefore, a subgroup analysis excluding this study was conducted for the following outcomes: hardware infection, wound infection, and amputation rate. Additionally, patients treated for tibiocalcaneal arthrodesis in this study were excluded from analysis.
Results
Search results
The electronic search strategy yielded 257 record hits. After removing seven duplicates, title screening generated 52 potentially relevant abstracts. Full manuscripts of 12 studies were retrieved and only 3 were found eligible. Reasons for exclusion were as follows: one study compared total contact cast with ankle arthrodesis, two studies compared surgical correction versus amputation, one study compared the cost of limb salvage versus amputation in patients with CNO, two studies compared nail to nail + EF, and three studies were review articles. Reference checking of the three papers yielded another relevant paper (Figure 1). In total, four studies 7,9,15,16 met the inclusion criteria and were included in the quantitative analysis: one quasi-randomized clinical trial and three retrospective comparative studies.

Flowchart of the search strategy.
Sample and Charcot deformity characteristic results
The four studies comprised 117 patients (117 interventions) with 98 having a diabetic Charcot neuropathy. Seventy patients were included in the IMN group and 47 in the EF group, with no previous surgeries. The mean age of the pooled sample is 56.54 ±1.9 years. All deformities were described as severe or as stage II/III of Eichenholz’s classification. The mean follow-up period was 2.84 ± 0.55 years. Preoperative ulcer presence and infection status are given in Table 1.
Characteristics of included studies.

IMN: intramedullary nail; EF: external fixator; RCS: retrospective comparative study; TT: tibiotalar joint; Q-RCT: quasi-randomized clinical trial; OM: osteomyelitis; ST: subtalar joint; TC: talo-calcanealL.
Quality assessment results
Using the JBI checklist tool, the total of “no” answers was zero for three studies. For Shah and De study, 16 there was one “no” answer in relation to the statement of strategies dealing with confounding factors. Table 2 presents the detailed quality items of each study.
JBI critical appraisal checklist for case control studies.

JBI: Joanna Briggs Institute.
Outcome results
Fusion rate
The weighted pooled proportions were of 90.7% (95% CI = 0.830–0.963, I 2 = 83.9%) versus 74% (95% CI = 0.610–0.852, I 2 = 56.8%) for IMN and EF, respectively. The weighted RD was of 14.6% (95% CI = −0.115–0.407, I 2 = 67.7%, p = 0.2) and the weighted odds ratio was of 2 (95% CI = 0.441–9.050, I 2 = 42.9%, p = 0.3), in favor of IMN. When the study of Ettinger et al. was excluded from the analysis, the weighted RD was of 17.1% (95% CI = −0.270–0.612, I 2 = 78%) in favor of IMN, but it did not reach significance (p = 0.4).
Time to heal
The mean time values for fusion healing were 29.3 ± 19.7 and 34 ± 25.4 weeks for IMN and EF, respectively. Unpaired t-test showed no significant difference (t = 0.23, p = 0.4).
Revision surgery (excluding amputation)
Weighted rates were 32.8% (95% CI = 0.186–0.489, I 2 = 48.5%) and 26.2% (95% CI = 0.127–0.423, I 2 = 64.4%) for IMN and EF, respectively. The weighted RD was 6% (95% CI = −0.132–0.255, I 2 = 79.9%) in favor of having revision surgery following IMN compared to EF, but with no significance (p = 0.5).
Hardware infection
Weighted proportions were 6.7% (95% CI = 0.021–0.136, I 2 = 87.3%) and 33.6% (95% CI = 0.2121–0.473, I 2 = 70.3%) for IMN and EF, respectively. The weighted RD was 18.4% (95% CI = 0.323–0.044, I 2 = 86.6%, p = 0.01), in favor of having hardware infection following EF compared to IMN. Similar results were found when the study of Ettinger et al. 15 was excluded; RD = 20.7% (95% CI = 0.371–0.043, I 2 = 67.5%, p = 0.01).
Wound infection
Weighted proportions were 4.4% (95% CI = 0.009–0.103, I 2 = 47.6%) and 23% (95% CI = 0.124–0.357, I 2 = 77.3%) for IMN and EF, respectively. The weighted RD was 14.8% (95% CI = −0.261–0.035, I 2 = 58.6%, p = 0.01), in favor of having wound infection following EF compared to IMN. Similar results were found when the study of Ettinger et al. 15 was excluded; RD = 22.5% (95% CI = 0.425–0.024, I 2 = 90.4%, p = 0.02).
Amputation rate
Weighted proportions were 2.2% (95% CI = 0.001–0.069, I 2 = 0%) and 13.1% (95% CI = 0.052–0.239, I 2 = 36.9%). The weighted RD was 12.2% (95% CI = 0.240–0.003, I 2 = 19.5%, p = 0.04), in favor of having an amputation following EF compared to IMN. Significance was lost when the study of Ettinger et al. 15 was excluded; RR = 7.7% (95% CI = −0.219–0.065, I 2 = 0%, p = 0.2).
Postoperative weight bearing
Compared to EF, two studies reported fewer time of non-weight bearing following IMN method, and one reported the same period for both methods (Table 3).
Comparative outcomes.
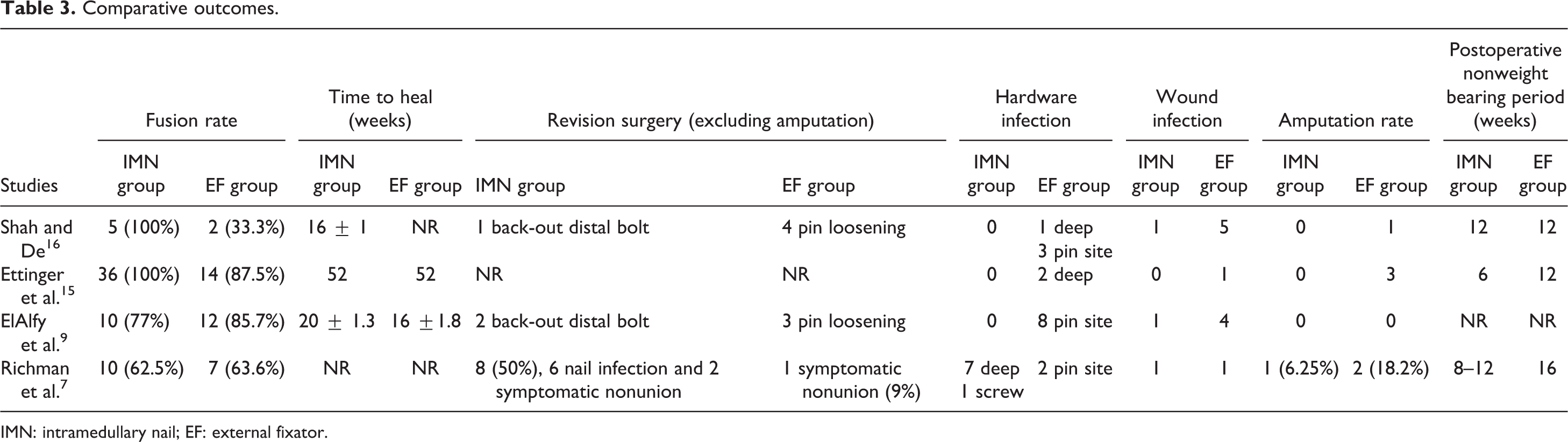
IMN: intramedullary nail; EF: external fixator.
Discussion
Although the difference did not reach significance, the mean fusion rate following IMN was found to be the double than that following EF. Further, in the quasi-randomized study of ElAlfy et al. 9 where no significant difference in fusion rate was reported, the authors stated that of the three patients showing a radiological nonunion following IMN, two had a pain-free stable ankle after a minimum follow-up of 26 months. Therefore, our results would suggest that IMN might be a better option than EF in terms of fusion rate for tibiotalocalcaneal arthrodesis. In addition, the mean time to heal after IMN was 5 weeks less than that needed after EF, but again significance was not attained.
Weighted RD related to revision surgery was found to be mildly higher with IMN technique but mostly due to nail infection from one study, that of Richman et al. 7 (Table 3). High revision rates following IMN have been reported in the literature, mainly caused by the need for nail removal. Pinzur and Noonan 17 and Caravaggi et al. 18 reported hardware removal in 14 and 21% of their IMN patients, respectively. Revision rate following EF displayed mixed results in the literature. El-Gafary et al. 19 and Fabrin et al. 20 reported 0% of revision surgery after EF, whereas Fragoman et al. 21 and Zarutsky et al. 22 reported 26.3 and 63.6% of revision surgery, respectively.
On the other hand, outcomes such as hardware infection and wound infection were found to have significant RDs in favor of IMN compared to EF in overall and subgroup analyses. Knowing the higher risk of infection associated with chronic diabetes, IMN method could be more appropriate in the diabetic population. The amputation RD value lost its significance toward IMN method once the study of Ettinger et al. 15 was excluded. In line with the literature, both methods yielded high limb salvage rate.
The major limitations of this review are the small pooled sample size and the study design of the included studies. Indeed, all were comparative studies but only one had a form of randomization (Table 1). Further and while all studies explicitly recorded their inclusion and exclusion criteria, not all comparative groups were explicitly reported as matched groups as is the case in Shah and De study. 16 While only one study showed 1 “No” answer of the 10 question items of the JBI appraisal tool, one study had 2 “unclear” responses and another 2 studies had one “unclear” answer. It is very likely that the included studies had similar but not very comparable quality.
The preoperative infection status could have impacted our healing results. For instance, Ettinger et al. 15 reported the use of EF in all cases where infection was present. However, that was not the case in the remaining three studies. Richman et al. 7 stated that neither the amount of deformity nor the quality of the soft tissue precludes either types of instrumentation. Shah and De 16 stated that the type of surgical procedure a patient underwent was senior author’s choice irrespective of the stage or condition of the bone. Additionally, no infected cases were included in both ElAlfy et al. 9 and Shah and De 16 studies. When sensitivity analyses were conducted by excluding Ettinger et al. 15 study, all results but the amputation rate were similarly in favor of IMN, but still not significant. In other terms, preexisting infection status did not alter our healing findings. To add, postoperative wound infection was significantly higher following EF, when analyses were conducted with and without Ettinger et al.’s study. 15
Although not significant, the difference found in the needed time for healing could have been compromised by the complete lack of such outcome reporting in one study 7 and the partial missing data in another one. 16 Another limitation is the lack of reported correlations with other relevant variables which might have impacted the outcomes. For instance, the peripheral vascular status was not been always accounted for as a potential confounding factor; only Richman et al. 7 reported this risk factor with similar number of patients having peripheral artery disease in both groups but no correlation with the fusion rate was conducted. Additionally, the impact of ulcer presence on fusion outcome was inconclusive. When used to treat patients having infected or noninfected ulcers, EF showed significantly lower fusion rate when compared to that reported in patients free of ulcers and treated with IMN. 16 However, ElAlfy et al. 9 showed no difference in fusion rate in relation to preoperative ulcer presence.
Based on this review, there is substantial evidence that IMN could yield better fusion rate with less complication than EF. However, the context in which the arthrodesis procedure is to be performed should be taken into consideration as well. With only 117 interventions to analyze where most patients were diabetic and having high risk of infection, indications to use one method over the other could be tailored to each individual depending on the ulcer/infection status. For patients free of ulcers, IMN method could be considered as a better choice than EF. In case of presence of medial or lateral ulcers at the ankle/foot area, IMN would also be preferable to avoid inserting fixator wires nearby potential infected areas. In case of presence of plantar ulcers, in particular those in the mid-foot or hindfoot, it could be better to avoid the plantar approach required for nail insertion; the EF in such cases would be a better option for arthrodesis. Figure 2 shows an algorithm to assist decision-making on arthrodesis technique in unstable ankle Charcot neuropathy.

Algorithm for decision-making for fusion method in unstable diabetic ankle Charcot.
Conclusion
There is evidence that IMN could yield better results than EF for tibiotalocalcaneal arthrodesis. Based on this review, IMN generated higher rate of fusion with lesser complications than EF. In the clinical context of ulcer presence on the plantar aspect of the foot, the EF might be a better solution, particularly in diabetic patients. Due to the small number of included studies summing a small pooled sample, further research via bid sampled randomized trials is warranted.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.