
Abstract
Study design:
A retrospective study of consecutive surgically managed cases of cervical spinal fractures and diffuse idiopathic skeletal hyperostosis (DISH) at our hospital from October 2006 to April 2016.
Summary of background data:
Prognostic factors have not been determined for cervical fractures in DISH.
Objectives:
To assess demographics, surgical techniques, and complications in cervical spinal cord injury with DISH and to evaluate factors affecting neurological prognosis.
Methods:
Patients’ medical records and radiographs were reviewed and analyzed for demographics, injury characteristics, surgical outcomes, perioperative complications, additional surgeries, and neurological prognosis. Neurological status was assessed by the American Spinal Injury Association (ASIA) grade at admission and discharge.
Results:
Of 38 patients (mean age 71.9 ± 8.8), 20 had type 1 fractures (through the disc space), 8 had type 2 (through the vertebral body), and 10 had type 3 (through disc and vertebral body). ASIA grades at admission included 14 ASIA-A, 4 ASIA-B, 7 ASIA-C, 8 ASIA-D, and 5 ASIA-E. All patients underwent posterior fusion with an average of 4.5 ± 2.5 instrumented vertebrae (range, 2–7) and six patients required secondary halo-vest fixation. Of 14 ASIA-A patients, 12 developed serious postsurgical pulmonary complications and 4 of these died within 6 months of surgery. Of the 38 patients, 13 improved more than one grade after treatment, 24 did not improve, and 1 deteriorated. In the 18 ASIA-A/B cases (complete motor paralysis), neither fracture type nor injury mechanism (e.g. a ground-level fall or high-energy trauma) correlated with neurological prognosis, but a time of 8 h or less from injury to surgery correlated significantly with an improvement from ASIA A/B to C/D (p < 0.01, Pearson’s χ 2 test).
Conclusion:
Patients with complete motor paralysis after a cervical fracture with DISH may recover to partial paralysis if surgically treated within 8 h of injury.
Introduction
Diffuse idiopathic skeletal hyperostosis (DISH) is a non-inflammatory disease in which the spinal longitudinal ligaments and enthesis become ossified over time, decreasing mobility in the affected segment. 1 DISH can be diagnosed by the presence of flowing ossification of the anterior longitudinal ligament over at least four consecutive vertebrae in lateral-view spine radiographs. 2 DISH is more common in people over 50 years of age, and its overall prevalence is greater than 10% in subjects that are 70 years and older. 3,4 In DISH, multilevel bony vertebral fusions produce long lever arms, creating an environment in which even low-energy trauma can cause fractures with an increased risk of neurological injury. 5 Delayed detection of fractures in the ankylosing spine is sometimes an issue with DISH, either because of misdiagnosis or the patient’s failure to seek medical attention promptly. In general, surgery is recommended for three-column injuries in the ankylosed spine because conservative treatments have not proven effective. 6 –10 This study presents a series of patients with cervical-spine ankylosis due to DISH who presented at our center with a spinal fracture. All patients were treated surgically by posterior decompression and fixation. We present the results with special attention to surgical outcomes and complications. Our goals were to assess and define the presentation and demographics in a series of patients with DISH and unstable cervical-spine fractures and to assess the factors affecting prognosis.
Materials and methods
A retrospective review at Hokkaido Spinal Cord Injury Center was conducted to identify patients who presented with DISH and fractures of the cervical spine and who were treated surgically between October 2006 and April 2016. These patients were identified by searching spinal X-rays and computed tomography images, and details were obtained from medical records and surgery notes. When DISH was identified, we examined the corresponding imaging studies and medical records for the presence of a cervical spinal fracture.
Evaluation of patient and injury characteristics
The following patient variables were assessed: (i) patient age; (ii) injury variables such as the mechanism of injury and the fracture type, as described previously; 11 (iii) preoperative neurological status using the American Spinal Injury Association (ASIA) grade; (iv) treatment variables such as time to treatment, surgical technique, and delay of diagnosis; and (v) posttreatment variables such as morbidity, mortality, additional surgery, and ASIA grade at final follow-up.
Cervical fractures caused by a distraction force were classified into three types 11 based on whether the fracture through the anterior spinal column involved the intervertebral disc, the vertebral body, or both the body and the disc.
Evaluation of neurological function
Patients were assessed for neurological function by the ASIA spinal injury grade at the time of their initial assessment in our center’s emergency room and at their last follow-up.
Complications
Patients’ medical records were evaluated for perioperative complications related to the injury. We also looked for delayed diagnosis, which we defined as a lack of documentation of a fracture within 24 h of the patient’s initial assessment, 5 for any decline in neurological function and death. Decline in neurological function was defined as an obvious worsening of the patient’s motor score from the time of the initial examination to the most recent follow-up.
Statistics and level of significance
Means, standard deviations, and correlations were computed for descriptive analysis. Cross-tabulation tables were applied along with Fisher’s two-tailed exact tests and Pearson’s χ 2 test. Data were analyzed with unifactorial analyses of variance and two-sided, unpaired Student’s t tests as post hoc tests. For all analyses, Mac statistical analysis add-in software for Microsoft Excel (ESUMI, Japan) was used. A p value less than 0.05 indicated a statistically significant relationship between variables or a significant difference between means.
Results
Patient and fracture characteristics
Our review of medical records and radiographs identified 38 patients (35 males and 3 females) with DISH and unstable cervical fractures. The mean age was 71.8 ± 8.8 years (mean ± SD; range, 53–92 years). The fracture location was C3–4 in 2 cases, C4–5 in 10, C5–6 in 12, C6–7 in 11, and C7–Th1 in 3. The most common fracture type, a fracture through the disc space (type 1), occurred in 20 patients (52.6%); fractures through the vertebral body (type 2) occurred in 8 patients (21.1%), and fractures through both the disc and vertebral body (type 3) occurred in 10 patients (26.3%; Table 1).
Relationship of injury classification to neurological examination.
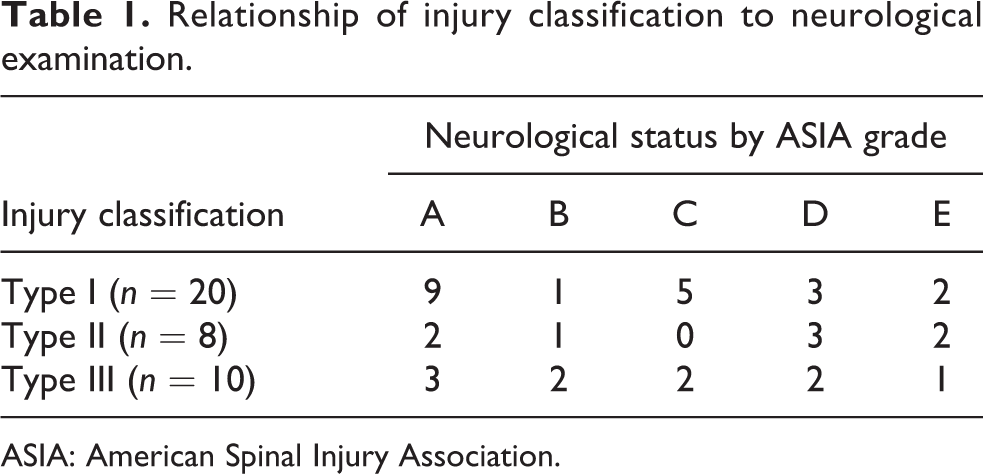
ASIA: American Spinal Injury Association.
Mechanism of injury and time to diagnosis
The most common mechanism of injury was a fall at ground level in 20 patients (52.6%), followed by motor vehicle collision in 8 (21.1%), a fall from a height in 6 (15.8%), and falling on stairs in 4 (10.5%). The average time from injury to diagnosis of the spinal fracture was 3.1 ± 7.8 days (range, 0–45); this included nine cases (23.7%) of delayed diagnosis.
Neurological status
ASIA grades were documented for all patients at the time of admission. There were 33 patients (86.8%) with a spinal cord injury (18 with complete and 15 with partial paralysis). The patients’ ASIA grades upon admission were as follows: 14 ASIA-A (36.8%), 4 ASIA-B (10.5%), 7 ASIA-C (18.4%), 8 ASIA-D (21.1%), and 5 ASIA-E (13.2%; Table 1). Statistical analysis showed no significant difference between the type of fracture and the ASIA grade. The ASIA grade at admission was used as the baseline in all patients. At the last recorded examination, 13 patients (34.2%) had improved at least one ASIA grade, 24 patients (63.2%) had no change, and 1 patient (2.6% (Figure 1)) had neurological deterioration due to disuse atrophy syndrome (Table 2).

A representative case of treated early than 8-h case. 65 years old male with C6–7 three column fracture (Bransford type 2). Double door laminoplasty, at C3–5 level underwent at other hospital 12 years ago. His preoperative modified Frankel grade was C1. We performed C5–T1 decompression and fusion surgery (C5–6 lateral mass screws and Th1 pedicle screws). His final modified Frankel grade was D2 at 1 years after surgery. (a) Preoperative CT with yellow arrows indicating fracture sites; (b) postoperative X-rays.
Neurological outcome by ASIA spinal injury grade at admission versus final follow-up.
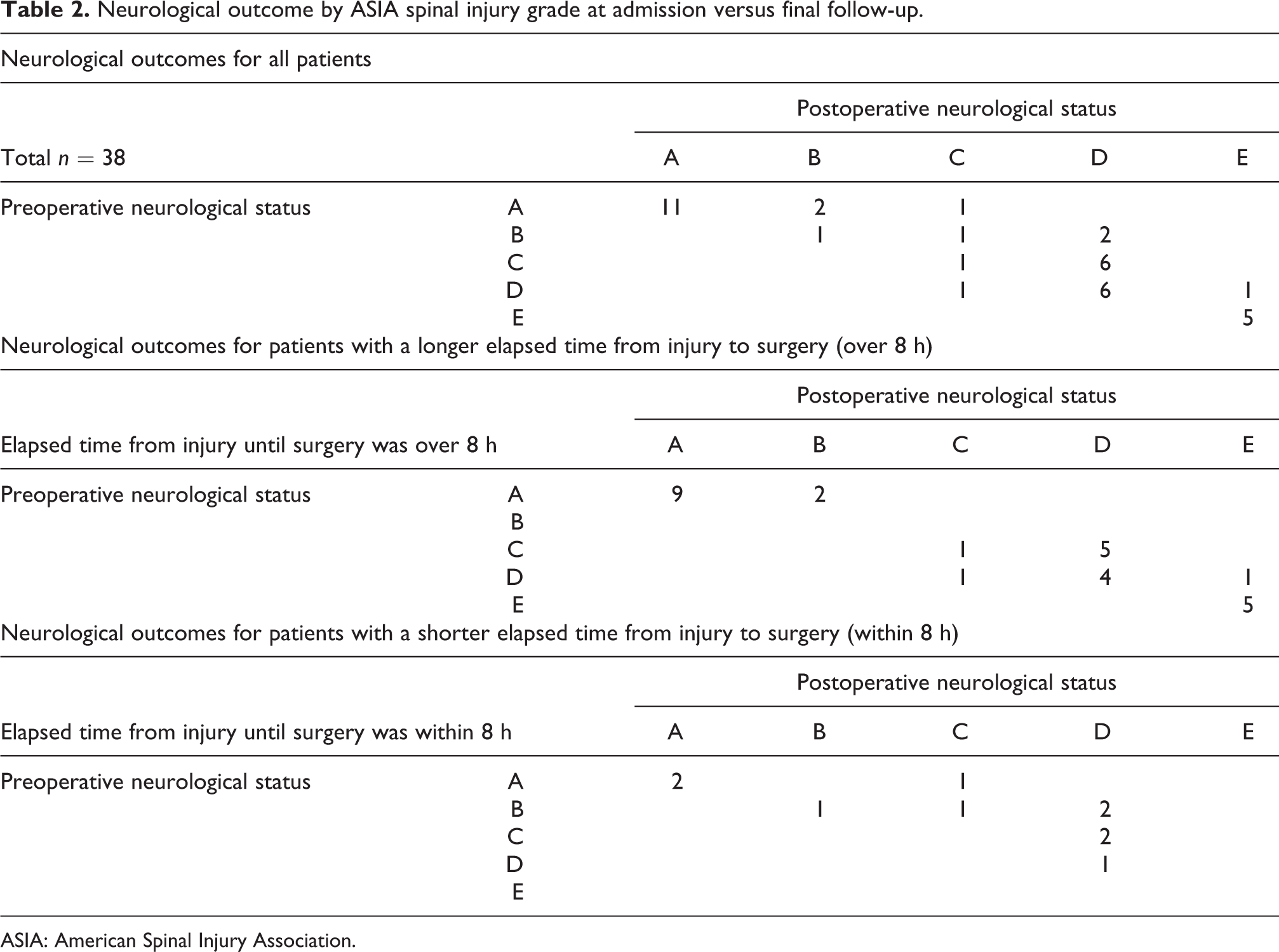
ASIA: American Spinal Injury Association.
Treatment data and complications
All patients were treated by posterior decompression and instrumented fusion; none of the patients was treated by anterior approach. The average number of instrumented vertebrae was 4.5 ± 2.5 (range, 2–7). Within 2 months after surgery, six patients (15.8%) required additional halo-vest fixation because instrumentation screws had loosened.
Table 3 lists perioperative medical complications, including eight patients (21.1%) with severe pulmonary postoperative complications requiring ventilator support and four patients (10.5%) who died within a mean of 3 months post-injury (range, 0.5–6 months). The average age at the time of death was 72.5 ± 11.0 years (range, 63–86 years), which was not much older than the total study population. All of the patients who died or had severe pulmonary disorders were ASIA-A on admission.
Perioperative medical complications associated with cervical fractures with DISH.

DISH: diffuse idiopathic skeletal hyperostosis.
Factors affecting neurological prognosis
Among 18 patients with complete motor paralysis (ASIA-A/B), neither the type of fracture nor the mechanism of injury was significantly correlated with neurological prognosis (Table 4). However, the elapsed time from injury until surgery was significantly correlated with neurological improvement (Table 2). Of 11 cases that were assessed as ASIA-A/B at admission and had an elapsed time from injury to surgery greater than 8 h (range, 8.5 h to 9 days), there was no neurological recovery (complete motor paralysis was unchanged, ASIA-A/B) at the final follow-up (Table 2). On the other hand, in seven ASIA-A/B cases with an elapsed time from injury to surgery of 8 h or less (average 5.4 ± 2.3 h, range 1–7.8), four patients (57.1%) recovered from complete to partial motor paralysis (from ASIA-A/B to ASIA-C or -D; Table 2). Statistical analysis revealed that the elapsed time from injury to surgery was significantly correlated with the neurological prognosis (p < 0.01, Pearson’s χ 2 test).
Neurological prognosis in relation to mechanism of injury or type of fracture.

ASIA: American Spinal Injury Association.
Of the remaining 20 patients with partial motor paralysis on admission (ASIA-C/D), only one patient had functional neurological deterioration at final follow-up, and this deterioration was due to disuse syndrome (Table 2). For these patients, there was no statistical correlation between neurological prognosis and the elapsed time between injury and surgery.
Discussion
Although several studies have assessed fractures occurring with ankylosing spinal disorders, most have not distinguished between ankylosing spondylitis and DISH. Until now, the largest single series to study cervical fractures with DISH was conducted by Branford et al., with 33 cases that were all treated surgically. 11 The present study included 38 patients with DISH cervical fractures, all of whom underwent posterior instrumentation surgery. This is a first study showing that surgical treatment within 8 h after injury significantly improved the neurological status in the patients with cervical DISH fractures. The injury was due to low-energy trauma in more than half of the patients (52.6%); this proportion was lower than that reported in other series. 11,12 Our center is a core hospital in the Hokkaido region (the northern area of Japan) and is specialized for spinal cord injury, and this probably accounts for the proportion of cervical DISH fractures caused by high-energy trauma being relatively high compared to that in other studies.
In our study, four patients (10.5%) died within 6 months of the injury. Other studies have reported mortality rates of 11% to 79%. 6,5,12 –14 All of the deaths in the present series were due to severe pulmonary disorders related to complete cervical spinal cord injury. All of the patients with severe pulmonary complications, including those who died, were ASIA-A on admission. This finding underscores the necessity for careful pulmonary monitoring in this frail population, as noted by Bransford et al. 11
Of the 33 cases of cervical DISH fracture reported by Bransford et al., 16 patients were treated with an anterior-only procedure, 12 patients with posterior-only instrumentation surgery, and 5 with a one-stage anterior-and-posterior procedure; patients treated with a posterior-only procedure had an average of 6.5 ± 1.4 (range, 4–8) instrumented vertebrae. 11 The patients in our series had an average of 4.5 ± 2.5 instrumented vertebrae (range, 2–7). This improvement in the number of instrumented levels in our study is likely to reflect advances in cervical posterior instrumentation that have occurred since previous studies. All of the patients in our series were treated with posterior-only instrumentation and decompression. Halo vests were required in six cases because of screw loosening after the surgery. Bone union was achieved in all cases at final follow-up. We chose the posterior-only procedure with instrumentation because of recent improvements in posterior cervical devices and the possibility of tracheotomy in cases with a neurological injury above the C5 level.
Although the bone mineral density (BMD) of both the lumbar spine and femur neck is increased in patients with cervical or thoracic DISH, 15,16 the bone quality of elderly patients with DISH remains to be elucidated. Since the ossified anterior longitudinal ligament influences the results of BMD measurement, routine dual-energy X-ray absorption scanning may overestimate the true vertebral body BMD in DISH patients. 15 We hope that new validation tools, perhaps using methods such as quantitative CT, will become available in the near future for evaluating bone microstructures and other factors related to bone quality. 17 Fractures in the ankylosed spine resemble those in long bones, and the consequent stress concentration at the fracture site makes these fractures unstable. Unlike ankylosing spondylitis, DISH presents with a diverse morphology and range of ankylosed vertebrae. For example, the number of mobile segments in the cervical spine was different in each case in our series, with some patients having segments with a fused, long-bone-like appearance, and others having a wide range of motion at the levels involving DISH. Furthermore, in some cases of cervical DISH fracture, the fractured vertebrae at the ankylosed site appeared osteosclerotic in preoperative CT images and difficulties faced by the surgeons in determining the lateral mass adequately by feel or in fixing the pedicle screws resulted in more levels being included in the fusion. This divergence between CT findings and what the surgeon can determine by feel during the surgery might arise from cancellous bone regression caused by ankylosis extending into the vertebra. To determine the appropriate therapeutic strategies for cervical DISH fracture, it is mandatory to assess factors such as stress concentration, instability of the ankylosed spine, and bone fragility. 17
In our series, the elapsed time from injury to surgery was correlated with the neurological prognosis in patients that presented as ASIA-A/B upon admission, suggesting that there is an 8-h golden window for avoiding complete motor paralysis after spinal injury. Although our study is the largest case series of cervical fractures in DISH to date, it is still limited by a relatively small sample size. Among patients that presented with partial motor paralysis (ASIA-C/D), the elapsed time from injury to surgery had no correlation with prognosis. However, Einsiedel et al. reported that because of unstable fracture configurations in the ankylosing spine, initially intact patients may sustain secondary neurologic deterioration after unprotected transfers or manipulation. 18 Even in patients that initially present as ASIA-C/D, motor function can deteriorate if the cervical spine is not positioned appropriately in a neck collar during emergency transport; thus, meticulous management is essential in all cases of partial motor paralysis. ASIA-A cases present a serious clinical challenge because of the high frequency of severe pulmonary complications and mortality. Our data show that surgical intervention within 8 h of the injury can improve postoperative outcomes, emphasizing the importance of early diagnosis and surgery for spinal cord injuries with complete motor paralysis.
Key points
Of 38 surgically managed patients with cervical DISH fractures, 8 (21%) had severe pulmonary disorders during the postoperative period and 4 (10.5%) died within 6 months of surgery. All of these cases were ASIA-A grade at admission. All patients were treated by posterior fusion with an average of 4.5 ± 2.5 instrumented vertebrae (range, 2–7), and six patients (15.8%) required secondary halo-vest fixation because of loosening screws. Even in patients with complete motor paralysis at admission (ASIA-A/B), surgical treatment within 8 h after injury can improve the neurological status from complete to partial motor paralysis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.