
Abstract
Background:
Three-dimensional (3D)-guided navigation percutaneous screw fixation of pelvi-acetabular fractures has been reported in patients with high-energy trauma. Its use in fragility fractures of the pelvis is expanding and its results are promising.
Methods:
We report a series of 17 consecutive patients with fragility fractures of the pelvis treated with 3D-guided navigation percutaneous screw fixation from 2016 to 2017. Percutaneous screw trajectories were planned preoperatively for the majority of patients. Closed reduction was performed prior to fixation in grossly displaced fractures.
Results:
The mean time to surgery was 8.6 ± 2.4 days, and the mean intraoperative blood loss was 94.1 ± 26.6 mL. One early surgical complication occurred involving an infected pelvic external fixator iliac pin track site, and there were no cases of neurological deficits after fixation. In total, 7 of the 14 patients had screw backout, and the mean backout distance was 8.3 ± 4.4 mm. Cortical perforation was seen in one patient involving an anterior column screw by 5.7 mm; 14 patients were followed up for a mean of 18.7 ± 2.8 months; 13 patients achieved complete fracture union, and 1 patient had a fracture non-union. Premorbid ambulatory function was restored in 8 of the 14 patients. The mean visual analogue scale for pain severity at follow-up was 0.36 ± 0.50. There were no cases of 30-day and 1-year mortality.
Conclusion:
3D-guided navigation percutaneous screw fixation is a safe, precise, and effective surgical technique for managing fragility fractures of the pelvis.
Keywords
Introduction
Fragility fractures of the pelvis (FFP) result from a fall from a standing height or from physiological loads and are seen in 7% of all osteoporotic fractures. 1 FFP is associated with osteoporosis, hypocalcaemia, vitamin D deficiency, and secondary hyperparathyroidism. 2 This subset of fragility fractures has garnered awareness worldwide with its climbing incidence and daunting projected medical and socio-economic impact. 1 Based on data from the US population, annual osteoporotic fractures and their costs are estimated to rise by nearly 50% from 2005 to 2025. 1 The incidence and costs of osteoporotic pelvic fractures are predicted to rise by 56% and 60%, respectively. 1 This trend is also being widely recognized internationally. 3 –7
Fundamentally different from high-energy pelvic fractures in younger adults, the low energy of injuries that cause FFP rarely result in major soft tissue disruption and fracture displacement is minimal due to stabilization by intact ligamentous constraints. 8,9 Similarly, haemodynamic instability is uncommon. 9 Therefore, the primary aims in managing patients with FFP are to achieve adequate pain relief and early mobilization.
Conservatively managed, FFP leads to impaired ambulation, increased infection rates from hospitalization and greater carer needs on discharge. 2,10 –13 Breuil et al. reported adverse events in over half their patients with FFP, with urinary tract infection accounting for half of all adverse events, followed by pressure sores, mood and cognitive alterations, and thromboembolic events. 2 Similar observations in this group of patients treated conservatively have also been reported. 10 –13 Mortality is high in this group of patients, with rates reported at 14.3% and 23% at 1 year. 11,13 Early surgical fixation of FFP is shown to significantly reduce pain and promote early mobilization. 13 –15 At 1-year follow-up, patients with screw fixation for posterior ring injuries demonstrated lower fracture displacement rates as well as improved functional outcomes. 15
Classical open approaches to the pelvis are extensive and lead to increased bleeding, wound complications, scar formation and heterotopic bone formation. 16,17 There is increasing interest in minimally invasive techniques due to reduced soft tissue disruption and reduced blood loss. 18 Computer-assisted fluoroscopy-navigated percutaneous screw fixation (minimally invasive) techniques, in particular, have been advocated for its accuracy and versatility in traumatic pelvic fractures. 16,17,19 –21 In a meta-analysis, computed tomography (CT)-guided navigation was associated with the lowest rate of screw malposition. 20 Three-dimensional (3D) fluoroscopy-based navigation had lower cortical perforation rates and better adherence to planned screw trajectories compared to two-dimensional fluoroscopy-based navigation in model and cadaveric acetabular fractures. 16 Sacroiliac screws similarly navigated in both cadaveric and in vivo pelvises had reported accuracies within a 2-mm range and procedure-related complications. 19,21 Long-term outcomes for fracture displacement, implant failure, and fracture union at a mean follow-up period of 30 months were favourable. 17
Based on our experience, 3D-guided navigation minimally invasive surgery (MISs) reduced blood loss, radiation exposure to operative staff and improved screw placement accuracy within reasonable operative time in most non-displaced or displaced pelvi-acetabular fractures. 19 The application of this technique in FFP is less reported in the literature, but we believe that the established advantages of this fixation technique in traumatic pelvic fractures can similarly benefit patients with FFP. In this series, we apply 3D-guided navigation MIS for pelvi-acetabular fractures to the management of 17 consecutive patients with FFP during the period between 2016 and 2017. We provide management strategies in optimizing patients with FFP during the perioperative period, present our methodology and the feasibility of navigation surgery in treating FFP and discuss the perioperative and 1-year outcomes.
Patients and methods
Patients with FFP were initially managed by conservative means involving adequate analgesia, medical optimization and physiotherapy for early mobilization and walking exercises. Those having unremitting pain impaired ambulation or high clinical or radiological suspicion of more unstable fractures, received a CT scan of the pelvis. Uncommonly, patients presented with haemodynamic instability and required immediate pelvic external fixator, retroperitoneal pelvic packing and angiography with or without embolization for pelvic haemostasis, followed by a CT scan of the pelvis for preoperative navigation planning. 22 Digital Imaging and Communications in Medicine (DICOM) data were analysed on the navigation computer and screw trajectories were planned with the 3D-reconstructed images.
Standardized screw fixation was performed for specific fracture patterns. Retrograde and antegrade anterior column screws were used to fix low-to-mid and mid-to-high anterior column fractures, respectively. Antegrade posterior column screws were used to tackle posterior column fractures. Supra-acetabular screws were used in fractures of the iliac wing, sizeable crescent fractures, high anterior column fractures and fractures involving both the anterior and the posterior columns of the acetabulum. Where necessary, supplemental fixation with subcristal screws were used in iliac wing fractures. Sacroiliac screws were used to fixed sacral fractures or sacroiliac joint diastasis. Screws were planned taking into account the optimal screw entry sites, trajectories across different fractures, and the surgical feasibility and margins of safety. The preoperative planning of multiple percutaneous screws is described and illustrated in Figure 1.

Preoperative planning images and post-operative radiographs of a multiple fractured pelvis of a polytraumatized 22-year-old man illustrates the different screw strategies used to tackle different fractures of the pelvis and acetabulum. The preoperative CT scan of the pelvis is analysed using the 3D navigation computer software. The ideal entry sites and spatial orientations of the screws, as well as their respective diameters and lengths, can be individually adjusted using the 3D software to achieve maximal bone purchase and fracture stability with adequate safety margins within narrow bony corridors of the pelvis and acetabulum. Any screw overlap or extra-osseous trajectories can be detected and avoided during the preoperative planning. In this example, bilateral sacroiliac and anterior column screws, left posterior column screw and left dome screws are planned and shown in the pelvic inlet (a), left iliac oblique inlet (b) and anteroposterior (c) image reconstructions. Each set of screws is colour coded to distinguish between them during preoperative planning and intraoperative execution on the navigation computer. For this patient, two left anterior column screws were planned, one antegrade and one retrograde, to allow for flexibility in execution should technical difficulties in either approach arise. The post-operative anteroposterior radiograph of the pelvis closely follows the preoperative plan (d).
All patients were optimized medically for surgery and gave consent for navigation surgery and open reduction and internal fixation should the need arise. Definitive fixation was performed under general anaesthesia with the patient positioned supine on an OSI radiolucent table. The Stryker NAV3i navigation computer system (Stryker Navigation, Kalamazoo, Michigan, USA) was set up at the caudal end of the radiolucent table and connected to the Arcadis Orbic 3D C-arm (Siemens Healthcare GmbH, Erlangen, Germany). Closed reduction of the fracture, where indicated, was by a combination of joystick manipulation via Apex pins (Stryker, Selzach, Switzerland) inserted into the iliac crest and traction and/or rotation of the ipsilateral leg under fluoroscopic guidance. The reduction was then maintained with an anterior pelvic external fixator which could be connected to femoral pins to hold the ipsilateral lower limb in a fixed degree of traction and rotation.
After installation of patient trackers, 3D fluoroscopy of the pelvis was performed, and the DICOM data thus acquired were simultaneously transferred to the computer navigation system for pelvic geometry registration. The 3D scan images, excluding mobile structures such as the femoral head, were merged with that of the preoperative CT scan. If a complete match is ascertained, the surgery will proceed according to the preoperative plan. Any inconsistencies suggesting fracture displacement necessitated replanning with or without closed reduction.
A 3.2-mm drill-tip guide pin was inserted with a calibrated rigid drill sleeve under real-time 3D-guided navigation. After insertion and positional verification of all guide pins, Asnis III 6.5 mm partially threaded, cannulated, titanium screws with washers (Stryker) were inserted over each guide pin and tightened sequentially. Detailed intraoperative set-up and logistics have been documented in a previous publication. 19
Post-operatively, all patients were immediately started on protected weight-bearing walking exercises with the physiotherapist. In patients with stable fixation and good bone purchase, full weight bearing was allowed. Chest physiotherapy, limb maintenance exercises and out-of-bed transfers were continued. Patients were closely monitored for occurrences of medical complications during the post-operative period. Calcium and vitamin D supplement and bone health medications were prescribed if not contraindicated.
The Student’s t-test was used in evaluating the statistical significance of differences in means. The unpaired t-test was used in the comparison of mean surgery times of the preoperatively and intraoperatively planned surgeries, while the paired t-test was used for comparison of means of the preoperative and post-operative visual analogue scale (VAS) for pain severity. Informed consent from patients was obtained for the use of their demographics, inpatient medical records and data and images for use in this publication with no personal identifying information.
Results
A review of 17 consecutive patients with FFP managed with 3D-guided navigation percutaneous screw fixation was conducted. The patient demographics and fractures sustained are shown in Table 1. The mean age was 80.1 ± 8.2, and 16 of the 17 patients were female. The mean Charlson comorbidity index was 4.9 ± 0.6. The majority sustained a fall on level ground from standing height, while one fell from a 1-m high bed, and one who did not sustain frank injury but complained of insidious and progressive sacral and groin pain for a month. Prior to their injuries, nine patients walked unaided, seven patients ambulated with an ambulatory aid, such as a cane or frame walker and one patient was wheelchair-dependent for ambulation.
Patient demographics.a

–: nil.
aClassification indicates tiles classification was used in pelvic ring fractures. Judet-Letournel classification was used for acetabular fractures. Arbeitsgemeinschaft für Osteosynthesefragen/Orthopoaedic Trauma Institute (AO/OTA) classification was used for both pelvic and acetabular fractures.
Of the 17 patients, 2 patients had a history of fractures preceding their pelvic injuries; one was an osteoporotic T12 and L1 vertebral collapse and the other was a fractured neck of femur for which hemiarthroplasty was performed. Aside from the pelvi-acetabular fractures, 4 of the 17 patients sustained a concomitant fracture. One patient had a fractured distal radius that was casted after closed reduction. Two patients had a fractured neck of femur; one was fixed with screws emergently, while the other was managed with a cemented hemiarthroplasty. The final patient sustained a fractured proximal humerus that was fixed with an intramedullary nail at the time of definitive pelvic fixation.
The mean time from admission to fixation of the pelvic fracture was 8.6 ± 2.4 days. As presented in Table 2, navigation surgery was executed according to preoperative plan for 13 of the 17 patients. This scenario is exemplified by patient 15 who sustained a Tiles B3, nondisplaced fracture of the right sacral ala, widening of the left sacroiliac joint and a fracture of the left superior ramus (Figure 2). Changes in fracture position were identified at the time of surgery in 2 of the 13 patients; as a result, the navigation plan could only be executed for the nondisplaced fractures, while the remaining screws had to be replanned intraoperatively using intraoperative 3D fluoroscopic images. The remaining 4 of the 17 patients had fracture reduction followed by intraoperative navigation planning and execution within the same operation. An example of this is in patient 12, whose case is presented in Figure 3.
Fracture classification and mode of surgical treatment with the corresponding operative time and blood loss.

–: nil; Pre-op: before definitive fixation; intra-op: at definitive fixation; post-op: after definitive fixation; U: unavailable; UTI: urinary tract infection; VAS: visual analogue scale for pain severity.

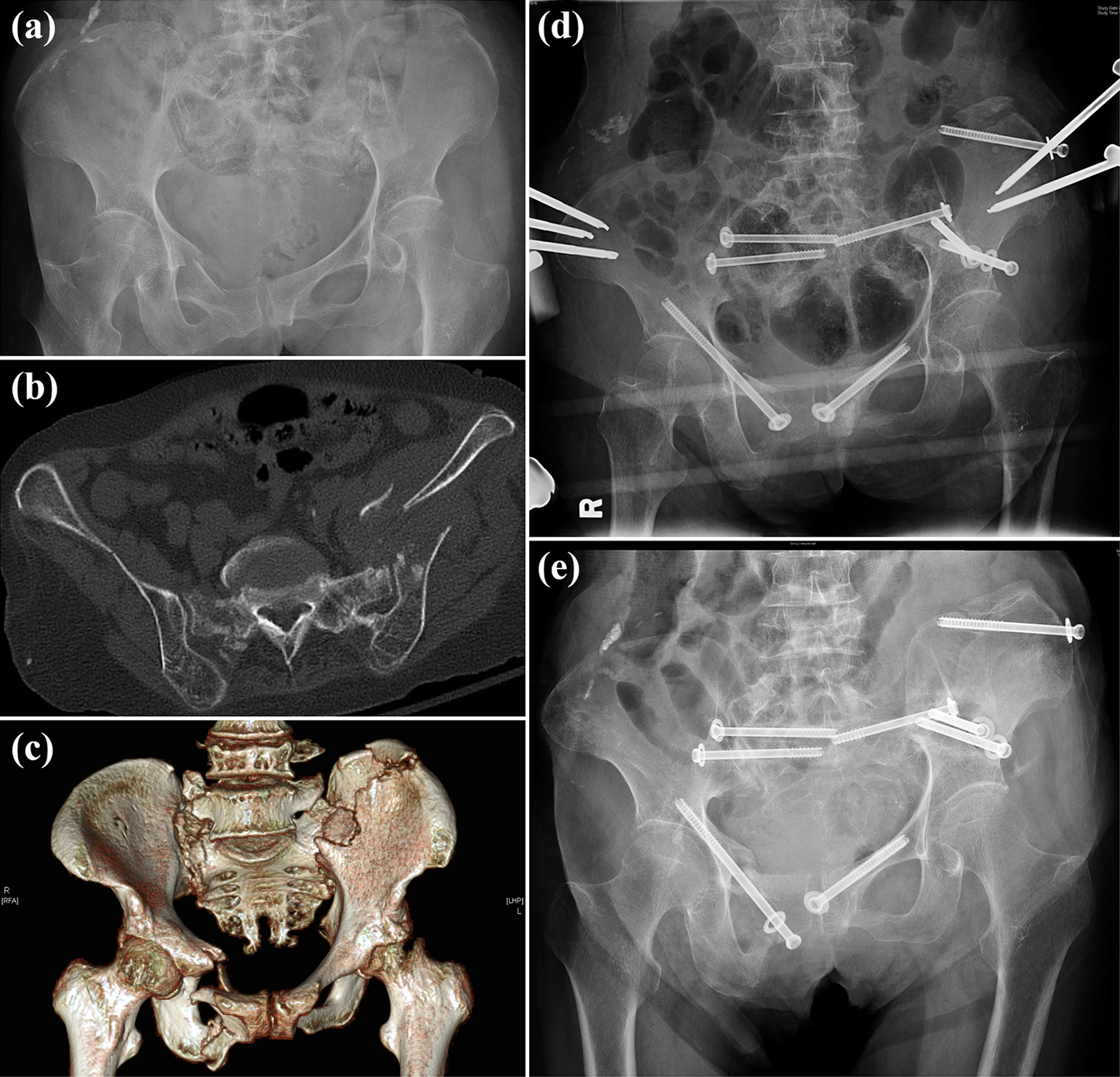
An 80-year-old male (patient 15) who fell from a standing height presented with sacral and left groin pain. The initial anteroposterior radiograph of the pelvis shows a left superior and an inferior pubic rami fracture (a). CT scan of the pelvis confirms these findings and reveals a nondisplaced Tiles B3 fracture of the right sacral ala and widening of the left sacroiliac joint (b). The 3D reconstruction of the pelvis is shown (c). The navigation plan showing the planned and the corresponding actual screw inserted superimposed one over the other (d). The upper left and right axial and coronal reconstructions (with relation to the screws) depict the trajectory for the superior right sacroiliac screw; the lower left image is the sagittal reconstruction depicting the trajectory for the superior left sacroiliac screw, and the lower right image depicts the computer-rendered radiograph with superimposed trajectories of the planned screws and the actual screws inserted. 3D-guided navigation screw fixation following the preoperative plan allowed for the precise insertion of two sacroiliac screws bilaterally through the S1 vertebral corridor and a retrograde left superior pubic ramus screw. The CT scan of the pelvis with axial (e) and coronal (f) reconstructions taken at 6 months after fixation showed satisfactory fracture union. The 3D-reconstructed anterior and posterior views of the pelvis at 6 months after fixation (g). Slight back out of the superior two sacroiliac screws was observed, which were present and remained static at 6 weeks after fixation.

An 81-year-old lady (patient 12) fell from a standing height with left buttock and groin pain. The plain anteroposterior radiograph showed a vague discontinuity over the left ilium (a) confirmed by the CT scan to be a significantly displaced Tiles B2, left ilium fracture (b). A concomitant nondisplaced left anterior column acetabular fracture is not shown. The ilium fracture was reduced intraoperatively with iliac crest pins and held with an anterior pelvic external fixator. Intraoperative planning was performed on the pelvis stably held in reduction with an external fixator. Two supra-acetabular guide pins were inserted through the restored bony corridor connecting the anterior inferior iliac spine and the posterior inferior iliac spine, and a single retrograde anterior column guide pin was inserted through the superior pubic ramus (c). The navigation computer interface showed the close adherence of the actual retrograde anterior column screw (pink) to the planned intraosseous screw trajectory (yellow screw) across multiple views/reconstructions (d). The anteroposterior radiograph of the pelvis taken after 3D-guided navigation screw fixation (e) and at 6 months after fixation showing optimal bone union (f). The 3D-reconstructed CT scan of the pelvis at 6 months after fixation also showed union of both fractures (g).
Three patients had grossly displaced pelvic fractures requiring closed reduction and fracture stabilization with an anterior pelvic external fixator. This included patient 8 who was the only patient in our series with haemodynamic instability on presentation, necessitating urgent retroperitoneal pelvic packing and selective arterial embolization (Figure 4). Following closed reduction, CT scan and navigation planning were performed for all three patients, with the pelvis geometry securely maintained by the external fixator through to the completion of 3D-guided navigation screw fixation.

A 101-year-old female patient (patient 8) fell from a standing height and sustained a Tiles B2 fracture of the pelvis with a displace left ilium fracture and a left anterior column fracture (a). The axial cut of the CT scan of the pelvis revealed the degree of displacement of the left ilium fracture (b). She was haemodynamically unstable on arrival requiring emergency closed reduction and anterior pelvic external fixation, retroperitoneal packing and selective internal iliac artery embolization (c). A second CT scan of the pelvis and surgical planning was performed with the ilium fracture stably reduced (d). The coronal and axial reconstructions in the follow-up CT scan taken at 1 month after fixation showed the precision and close proximity of all screws afforded by the 3D-guided navigation technique (e). Optimal fracture reduction and fixation at the left sacroiliac joint was achieved. The follow-up anteroposterior and left iliac oblique radiographs at 10.5 months showed optimal fracture union (f).
The mean operative times for the preoperatively and intraoperatively planned surgeries were 93.7 ± 32.4 and 133 ± 38.3 min, respectively. When put into context of the number of screws inserted, the mean operative time per screw was significantly lower in the preoperatively planned patients (24.9 ± 11.9 min) than in those planned intraoperatively (40.6 ± 7.9 min) (p < 0.05). The mean blood loss in all 17 patients was 94.1 ± 26.6 mL. The pain severity represented by the VAS was documented in 16 patients throughout hospitalization, and the mean improvement in VAS post-operatively was 3.3 (95% CI: 2.4–4.0, p < 0.0001). There was an early surgical complication of iliac crest pin tract infection and six perioperative medical complications: three cases of urinary tract infection, two cases of acute delirium and one case of upper gastrointestinal bleed from a duodenal ulcer.
Three patients defaulted follow-up, and the remaining 14 patients were followed up for at least 1 year with a mean follow-up duration of 18.7 ± 2.8 months. Five patients were walking unaided, seven patients required an ambulatory aid (a cane, quadripod or frame walker) and two patients were wheelchair-dependent. The ambulatory function of eight patients was restored to premorbid levels. The mean VAS for pain severity for all 14 patients at follow-up was 0.36 ± 0.50. Screw backout was seen in seven patients and was noted on radiographs at a mean of 3.8 ± 1.0 weeks with no progression or new incidences of migration in the period that followed. The mean backout distance was 8.3 ± 4.4 mm and aside from a palpable prominence beneath the skin in one patient, it was not associated with pain or impingement symptoms. There was one case of intra-articular perforation of an anterior column screw (patient 7).
Complete fracture union was seen in 13 of the 14 patients at a mean of 6.8 ± 1.4 weeks. Only one patient had a fracture non-union. There were no cases of fracture displacement or neurological deficits following fixation. There was no 30-day or 1-year mortality in this series of patients. Table 3 summarizes these findings.
Follow-up duration and patient functional and radiological characteristics at follow-up.a
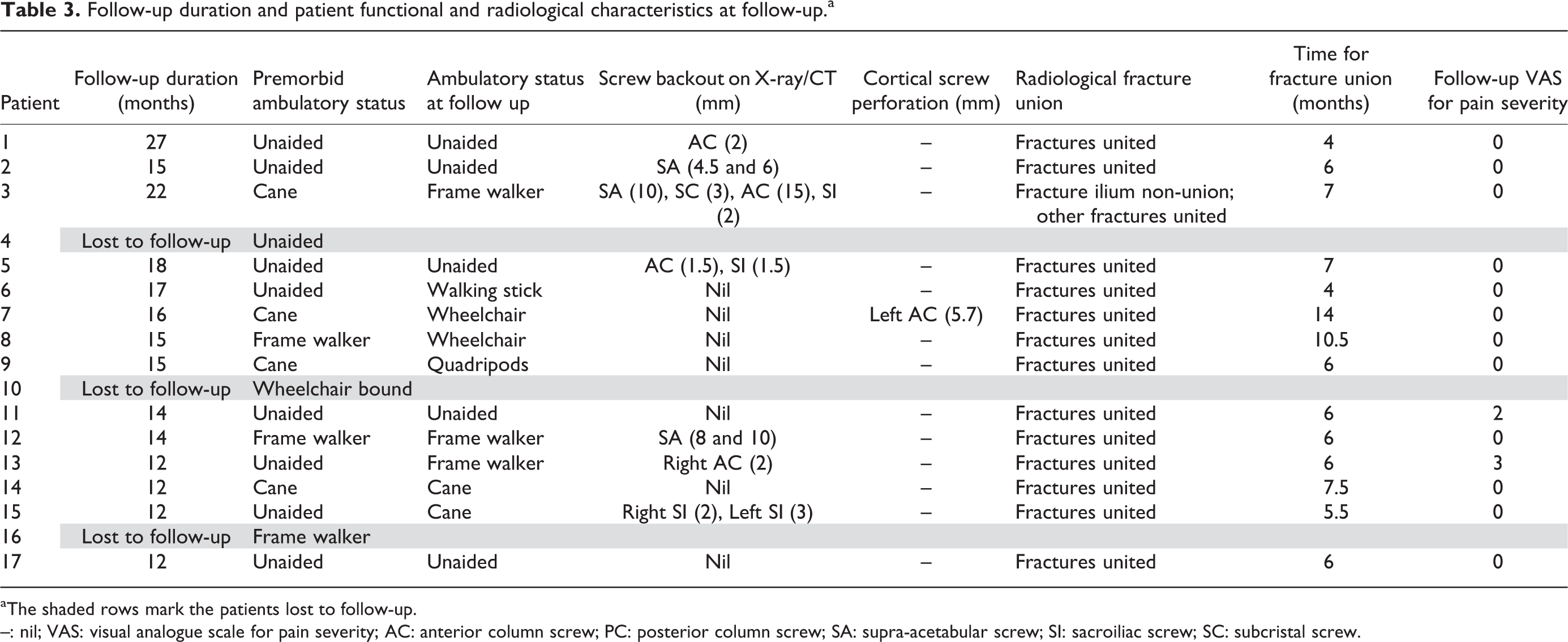
aThe shaded rows mark the patients lost to follow-up.
–: nil; VAS: visual analogue scale for pain severity; AC: anterior column screw; PC: posterior column screw; SA: supra-acetabular screw; SI: sacroiliac screw; SC: subcristal screw.
Discussion
Up to 60% of dorsal hemipelvis structures such as the sacrum, sacroiliac joints, and spinopelvic junction, may be missed. 8,11 They are poorly visualized due to overlapping bowel gas shadows. CT scans or radionuclide bone scans diagnosed 94% of sacral fractures missed on plain radiographs. 11 In this series, the multiplanar CT scan has served as a reliable imaging modality in the diagnosis and surgical planning of FFP.
Unlike patients of high-energy trauma, those sustaining FFP are often haemodynamically stable with nondisplaced fractures. FFP generally affects elderly patients who frequently have a myriad of medical co-morbidities including osteoporosis and compensated ambulatory statuses. The patients in our series had a mean age of 80.1 ± 8.2, and a mean of Charlson comorbidity index of 4.9 ± 0.6. Nearly half of them required some form of ambulatory aid before their injuries, which was similar to that reported by Mears et al. 13 With this demographic profile, patients are at increased risk of perioperative surgical and medical adverse events and complications of prolonged immobilization. A combined, multidisciplinary collaboration has been shown to reduce time to surgery, perioperative complications and mortality and overall improved outcomes in these patients. 18 The treatment aim is to shorten the period of immobilization, thereby minimizing adverse events associated with immobility, to restore pre-injury level of function and independence, to achieve pain relief and prevention of long-term pain, and to initiate osteoporotic treatment to prevent future fractures.
In managing fragility fractures in our hospital, we adopted a multidisciplinary approach under a standardized protocol involving early co-management with physicians, anaesthetists and fracture liaison nurse. It served to facilitate early definitive surgery and reduce co-morbidity-related complications through medical and physical optimization. In our series, dependent premorbid ambulation was seen in 8 of the 17 patients who required either ambulatory aids or a wheelchair. Further decline in patient autonomy and mobility can be curbed by early physiotherapist intervention. 18 With an ageing population and rising incidence of osteoporosis, similar management strategies can also be beneficial to patients with FFP. In our practise, ambulatory physiotherapy was started soon after admission. For patients potentially requiring additional social care, financial assistance or residential homes, social workers were actively involved in early discharge planning to accommodate to their individual needs upon discharge.
Radiographic evidence of osteoporosis was reported in 93.0% of patients with pelvic fractures. 12 In a study involving 60 patients with FFP, over half of the patients had been diagnosed with osteoporosis before their injuries, but only about a third of them were treated accordingly. 2 A similar observation of undertreated osteoporosis was reported in a separate study, despite 70% of the patients had pre-existing osteoporosis. 10 Underdiagnosis and suboptimal treatment of osteoporosis must be proactively avoided. As shown in our series, it is not uncommon for elderly patients to have sustained previous fractures or concomitant extra-pelvic fragility fractures at first presentation, underscoring the importance of bone health management. All patients in our series received supplementary calcium and vitamin D on hospital admission. Initial workup was performed to exclude common medical causes of low bone mineral density such as hypocalcaemia and renal impairment leading to secondary hyperparathyroidism. Arrangements for dual-energy X-ray absorptiometry (DEXA) scan were made at the time of hospitalization.
Bisphosphonates were conservatively prescribed in our series, because its use in our hospital underwent a major revision during time of this study. This has led to the current bone health prescription programme and the backbone of the fragility fracture management protocol in our hospital. It facilitates patient stratification based on risk of further fragility fractures and identifies patients that indicated for bisphosphonates. Follow-up for patients on bisphosphonates is also streamlined to assess treatment response and detect adverse effects of the medication such as musculoskeletal pains, gastrointestinal symptoms, bone turnover suppression and atypical fractures and jaw osteonecrosis.
Concomitant fractures, if present, must be addressed early to achieve early mobilization and avoid common yet devastating complications of immobility. Patients having failed conservative management are candidates for early operative treatment for the same reasons. In our series, surgical fixation of pelvic fractures led to rapid and significant reductions in pain, facilitating early rehabilitative efforts. In our experience, patients who decline an indicated operative fixation often forgo a certain degree of ambulatory independence at follow-up. Aside from traditional open approaches to the pelvis and screw fixation techniques, pelvic external fixator with supra-acetabular pins, or the less preferred iliac crest pins, is also a definitive treatment option. However, its use as a temporary or definitive treatment is associated with aseptic pin tract loosening, infection and injury to the lateral femoral cutaneous nerve. 23,24 Its use as definitive treatment also entails an extended period of hospitalization.
3D-guided navigation MIS of the pelvis enabled precise insertion of screws within narrow safety margins. A previous study on pelvis models derived from the Chinese population showed anterior columns accommodating screw diameters of 11.20 ± 1.73 mm. 25 In this series, Asnis III 6.5 mm screws for anterior column fracture fixation could be safely inserted in all patients without penetrating the hip joint or inner cortex of the superior pubic ramus. This required fine adjustments of screw dimension and orientation during the preoperative planning phase. Intraoperative fluoroscopy further confirmed guide pin and screw positions and only a few, screw-specific views were required. For example, the inlet and outlet views of the pelvis allowed assessment of the anteroposterior and superoinferior positions of the sacroiliac screws, the obturator oblique outlet view of the pelvis was used to assess the supra-acetabular screw trajectory (Figure 3(c)). Although radiation exposure and time to surgical personnel was not recorded in this series, the usage of intraoperative fluoroscopy was limited to only a few views for each guide pin and screw. The importance of a good familiarity with the pelvic anatomy and understanding of its variations cannot be overemphasized. The navigational apparatus supplements, but in no way supplants, surgical knowledge and judgement. Despite the precision afforded by 3D-guided navigation, surgeons must be well versed with the surgical knowledge and technique in fluoroscopy-guided MIS as well as the traditional open approaches to the pelvis.
Overall, screw migration occurred in just over half of the patients at a mean of 3.8 ± 1.0 weeks, and the mean backout distance was 8.3 ± 4.4 mm. No progression or new incidences of migration were detected radiologically thereafter. Sacroiliac screw loosening is theorized to occur due to a consistent pattern of diminishing cancellous bone density lateral to the sacral foramina. 26,13 However, in our practise, sacroiliac screws placement surpassed this region to the midline of the sacral vertebra where bone density was higher. Moreover, over tightening of the partially threaded screws to effect interfragmentary compression was avoided due to osteoporotic bone. This could have permitted some degree of fracture dynamization and produced what appeared to be radiological evidence of screw backout or loosening. No cases of fracture displacement due to screw migration was noted in our series, thus the significance of this radiological phenomenon remains unclear.
Screw migration was especially striking in patient 3, a 72-year-old lady who presented with progressive atraumatic sacral and groin pain for 1 month (Figure 5). Radionuclide bone scan revealed a severely osteopenic pelvis fractured at multiple sites, and each fracture displayed varying degrees of chronicity and bone resorption. She proceeded with intraoperative planning and screw fixation of the pelvis. An anterior pelvic external fixator was deemed necessary to reinforce the fixation in view of the poor bone stock and suboptimal screw purchase identified intraoperatively. Unfortunately, an infection of the iliac crest pin tract developed requiring debridement, antibiotics and premature removal of the loosened external fixator. The infection resolved but non-union of the ilium fracture and backout of all screws ensued. In spite of this, she reported no pain symptoms since early follow-up and her ambulatory function was restored to premorbid levels.
A 72-year-old female (patient 3) presented with progressive atraumatic sacral and groin pain for 1 month. Initial plain radiographs (a), CT scan of the pelvis (b) and 3D-reconstructed CT scan of the pelvis (c) showed a Tiles B3, multiple fractured pelvis involving the right superior and inferior pubic rami, left superior pubic ramus, bilateral sacral ala and left ilium extending to the acetabular dome and iliac crest. The pelvis was severely osteoporotic, and the fractures demonstrated different stages of union indicating cumulative fractures over a period of time. Closed reduction with an external fixator, intraoperatively planning and navigation-guided screw fixation were performed. The external fixator was kept in situ to augment fixation stability and within 1-month screw loosening was observed (d). Further screw migration occurred early and non-union of the left ilium fracture was noted on subsequent radiographs (e). The patient walked with a frame and had no pain around the pelvis at follow-up.
Cement augmentation through modified screws with fenestrations at the leading end can minimize screw loosening and enhance the stability of the fixation in osteoporotic bone. 27,28 In a series of 12 patients treated with cement-augmented screw fixation, full weight bearing walking was initiated immediately following surgery and all regained their pre-injury functional status without significant pain. 28 Another similar series reported no cement-related complications and optimal pain control, and that patients were allowed full-weight-bearing ambulation post-operatively. 29 Published data from mechanical studies in cadaveric hip models are varied with cement-augmented sacroiliac screws shown to have similar to significantly higher construct stiffness and pull-out strength compared to uncemented screws. 30,31 In theory, bone union of the fracture surfaces are not jeopardized as they are spared of the cement, 29 but the long-term outcomes are uncertain due to paucity in clinical trials. A recent clinical trial demonstrated improved bone mass and reduced pedicle screw loosening with the use of teriparatide (human recombinant parathyroid hormone) for 6 months after spinal fusion compared to bisphosphonates alone. 32 However, as screw migration in our series occurred during the early post-operative period, it is uncertain whether pharmacological therapy will alter the course of its development.
Patient ambulatory statuses were restored to premorbid levels in 8 of the 14 patients and a step-wise decline was noted in the remainder of the patients. Residual pain symptoms may not fully account for the latter, as the mean VAS for pain severity at follow-up was 0.36 ± 0.50. In reality, its causes may be multifactorial, such as those observed in patients with FFP managed conservatively, that is, reduced functional autonomy and increased community care or need to be institutionalized. 11 –13 Hopf et al. reported favourable ambulatory outcomes after percutaneous iliosacral screw fixation at 31 months, with 16 of the 22 patients reported as having no or minor restrictions of mobility. 14 We believe that a longer follow-up period in our series will elucidate our observations.
Limitations of this study include its relatively small patient sample, its inherent retrospective design and lack of objective functional scoring for each treated patient. Furthermore, the heterogeneity of the study population, injury patterns and concomitant injuries may complicate analysis and direct comparison with similarly conducted studies. Immediate pain relief following surgery by this technique is evident, but further studies with serial functional scoring in a larger patient sample will help validate the encouraging outcomes noted on follow-up.
Conclusion
The rising and projected economic burden and incidence of fragility fractures of the pelvis are causes for concern. Prompt diagnosis that comes with heightened clinical awareness, appropriate imaging diagnostics and early mobilization are critical towards favourable patient outcomes. Because of the inherent physical and medical heterogeneity of patients, treatment should be individualized and a multidisciplinary approach adopted in their overall management. 3D-guided navigation percutaneous screw fixation represents a safe, effective and accurate approach to pelvic fracture fixation that offers immediate post-operative pain relief and facilitates early weight-bearing mobilization.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.