
Abstract
Background:
Total knee arthroplasty (TKA) is an important option in the management of severe osteoarthritis. Despite excellent long-term results following TKA, the immediate postoperative period is often associated with pain, bleeding, edema, and reduced range of movement. Cryotherapy has been shown to provide some benefit in addressing these factors but results are largely controversial. This study aims at reviewing the current existing literature on the effects of cryotherapy following TKA.
Methods:
A comprehensive review of the current literature on the use of cryotherapy in knee arthroplasty was performed. The literature search was performed using PubMed, Cochrane Library, Google Scholar, and cross references using the search words “cryotherapy” AND “knee arthroplasty” for articles published between January 1990 and November 2016.
Results:
A total of 51 articles were analyzed and 24 of them were selected based on clinical relevance.
Conclusion:
Immediate and early postoperative management following TKA remains challenging. Cryotherapy has been shown to have some benefits but the severe lack of level 1 studies supporting its use make it difficult to reach a suitable conclusion. Further multicenter randomized controlled trials with representative populations and fair comparison of devices are needed.
Keywords
Background
Osteoarthritis (OA) of the knee is one of the leading causes of disability worldwide. 1 The age standardized incidence of knee OA is 3.8% across the world and 80% of patients over the age of 75 have radiologically proven OA. 2 Knee OA can lead to severe pain and loss of function.
Total knee arthroplasty (TKA) is one of the major options for the management of end-stage knee OA. 3 Excellent improvement in pain, mobility, quality of life, and function has been reported both in the early term (within 3–6 months postoperatively) and in the long term up to following this procedure. 4 Despite the encouraging results of TKA, the immediate postoperative period is often associated with significant issues such as pain, surgical blood loss, and localized edema resulting from tissue damage and the inflammatory response. 5 These are considered crucial factors due to their influence on postoperative opiate use, requirement for blood transfusion and its associated risks 6 as well as a negative impact on postoperative rehabilitation. This can result in increased length of stay and increased cost to the treating unit. 7
In spite of progress in anesthesia and multimodal pain management, TKA remains a challenging procedure for many patients. This has led to the use of nonpharmaceutical management adjuncts such as cryotherapy to address the immediate postoperative concerns described earlier.
The aim of this article is to review the role of cryotherapy, the proposed pathophysiology behind its use, its evolution with time, and a review of the existing literature on its efficacy and potential risks associated with its use following TKA.
Physiology of action
Cryotherapy involves the application of a cold substance, such as ice, to the skin surrounding inflamed soft tissues and joints. The theoretical physiological benefits of clinical cryotherapy have been widely documented since its use in the 1960s and the effects of ice have been demonstrated in several animal and human studies. 8,9 The proposed mechanism of action is that a reduction in temperature reduces intra-articular temperature and limits pain through reducing nerve conduction velocity in addition to promoting immediate vasoconstriction, reducing vascular spasm and slowing down of blood flow, ultimately decreasing tissue edema. 10
The intra-articular temperature reduction is transient. 11 Studies in animal models have demonstrated that excessively low temperatures or prolonged cooling results in a paradoxical increase in local edema. 12 Despite immediate vasoconstriction and reduction in blood flow, cryotherapy could lead to delayed vasodilation and disruption of secondary hemostasis. Evidence also exists, showing that local application of ice could impair hemostasis, leading to prolonged bleeding time, increased clotting time, reduced platelet aggregation, and increased clot formation time, although this has not been shown to be an issue in patients without pre-existing coagulopathy. 13
Some authors have reported limited benefit of cryotherapy on alleviating pain 14 or reducing blood loss 15 and inconsistent findings on decreasing swelling and improving mobility 16 post-TKA. The following discussion addresses these issues.
Methods
A review of the current literature relating to the use of cryotherapy following TKA was performed.
Outcome measures
The following outcome measures were analyzed and defined as: Pain: measured postoperatively using a subjective pain scale such as Visual Analogue Scale (VAS) Blood loss: measured as volume of blood noted in postoperative surgical drains or drop in hemoglobin levels postoperatively Edema: determined by measurement of knee circumference postoperatively in centimeters/inches using a tape Range of motion: measured as the degrees of flexion and extension at the knee joint postoperatively
Types of studies
Eligible studies included only full-text meta-analyses, systematic reviews of randomized controlled trials (RCTs), and true RCTs (where allocation was completely unpredictable) or controlled clinical trials published in the English language.
Participants
Participants were limited to adults who underwent primary elective TKA of any type indicated for severe OA. Studies where participants underwent unicompartmental knee arthroplasty were excluded.
Search strategy
The literature search was carried out using PubMed, Cochrane Library, Google Scholar, and cross references using the search words “cryotherapy” AND “knee arthroplasty” in the abstract/title of articles published between January 1990 and November 2016. In addition to the included articles, reference lists and related articles on Pubmed were examined for possible additions.
Data collection
The first author (AT) independently assessed the titles, abstracts, and keywords for the search results. Inclusion of articles was performed by first analyzing potentially relevant article titles and subsequently reviewing the corresponding abstracts. In cases where further information was needed, appraisal of the full text article was performed to determine its eligibility for inclusion. Full-text review of all other eligible studies was also performed and any reasons for exclusions were noted.
Results
This search yielded a total of 51 articles. These were reviewed and 24 of them were selected for further review based on clinical relevance and inclusion criteria (Figure 1). Detailed characteristics of these articles are further summarized in Table 1.

Flowchart detailing selection of articles included.
Summary of results from existing literature.
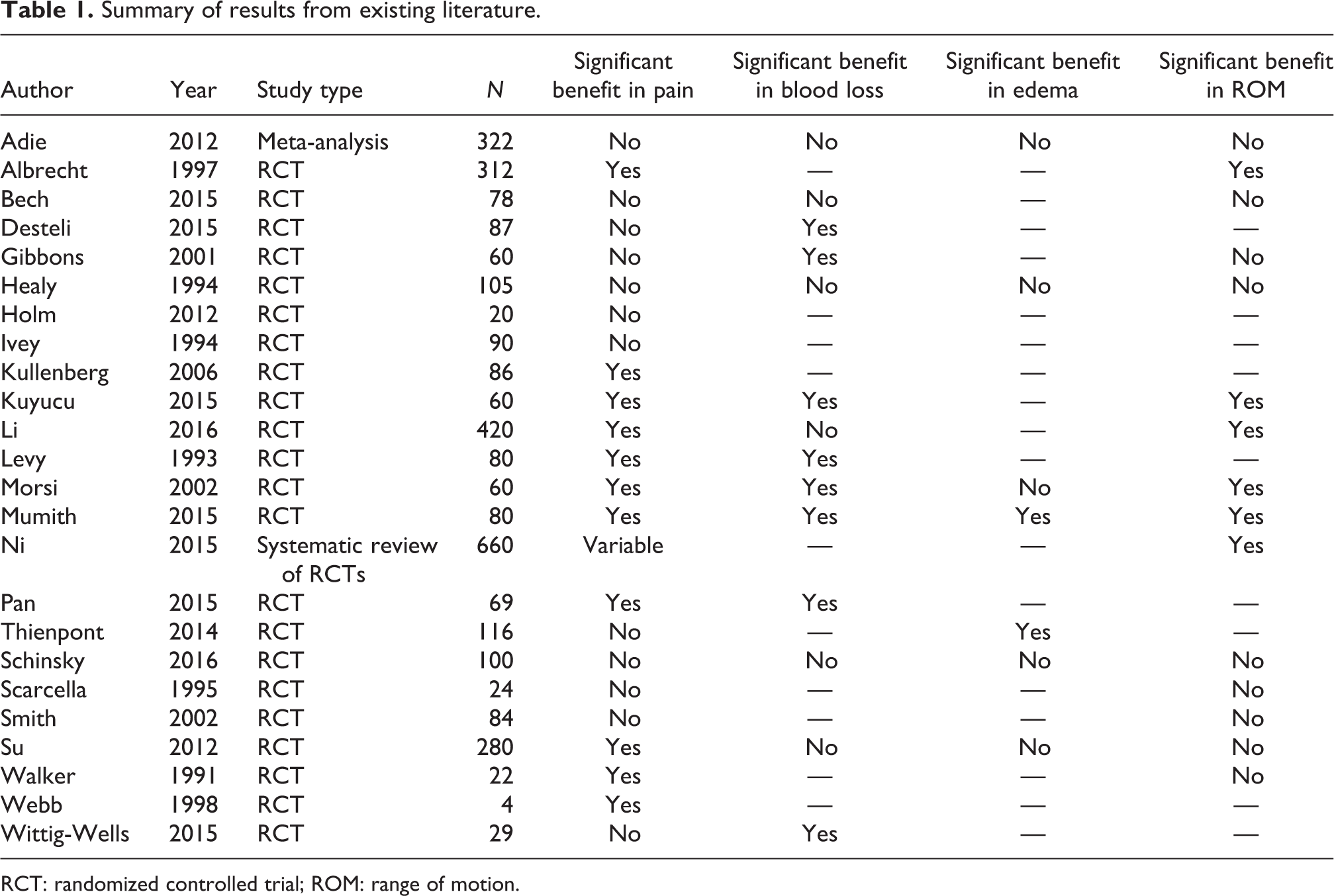
RCT: randomized controlled trial; ROM: range of motion.
Pain
Pain has been the most investigated outcome measure in studies involving cryotherapy post-TKA. Kullenberg et al. 17 observed significantly better pain control and patient satisfaction in patients treated with cryotherapy compared to epidural anesthesia in 86 patients following TKA. However, due to the nature of the interventions, the study is at high risk of performance and detection bias. Similar findings were reported by Morsi 18 and Albrecht et al. 19 who found that continuous cold application resulted in greater than 50% reduction in analgesic demands, although seven patients in the continuous cooling group were excluded from the study due to pain and local skin reactions. Morsi, 18 on the other hand, included patients with bilateral TKA, whereby each patient received both treatments—compression with cooling device as well as no cooling, potentially introducing reporting bias. Levy and Marmar 20 noted mild improvements in narcotic analgesia demands postoperatively when cold compressive dressings were used, although a conflict of interest could exist following the authors’ acknowledgement of the study being supported by the manufacturers of the dressings. Ni et al., 21 on the other hand, found that cryotherapy decreased pain on the second postoperative day only, but not the first or third day.
Smith et al. 22 and Gibbons et al. 23 reported no significant reduction in pain using cold compression dressings when compared to a Robert Jones bandage. Adie et al. 24 undertook a systematic review and meta-analysis of 11 prospective RCTs on cryotherapy post-TKA and found no improvement in pain and analgesia requirements. They noted significant heterogeneity in the studies included and a lack of patient reported outcomes which potentially influences the significance of their results.
There is growing evidence that the use of cryotherapy together with pharmaceutical analgesia is increasing in popularity, 25 although Wittig-Wells et al. 26 found no reduction in pain or improvement in patient satisfaction investigated short-term use of cryotherapy with analgesia compared to analgesia alone. The number of patients included in this study was small however.
Blood loss
Blood loss can be a significant problem post-operatively, requiring blood transfusions at times. Levy and Marmar 20 reported a significant reduction in post-operative blood loss in patients treated with cold therapy compared to controls in a cohort of patients who underwent 10 bilateral and 80 unilateral TKAs with similar findings also shared by Ni et al. 21 Desteli et al. 27 assessed the effect of cryoceutical treatment both pre- and post-TKA versus no intervention. Despite concluding that this approach was effective at reducing peri-operative and postoperative hemorrhage, they did not report a statistically significant difference in need for transfusion between groups. Similarly, Gibbons et al. 23 observed less blood loss in the surgical drains of patients in the cryotherapy group. Morsi 18 also concluded that continuous-flow cold therapy was advantageous in reducing blood loss following TKA. However, the 6-week interval between TKAs in each patient was insufficient to allow hemoglobin levels to normalize, therefore potentially leading to inaccurate measurements of blood loss.
In contrast to the above studies, Smith et al. 22 and Kuyucu et al. 15 found no significant reduction in postoperative blood loss with the use of cold therapy, although Kuyucu et al.’s 15 study also included a number of patients undergoing unicondylar knee arthroplasty.
Postoperative swelling
Relatively, few authors have investigated the effects of cryotherapy on postoperative swelling and edema. Contrasting results were reported by Healy 28 where a positive effect was noted with cryotherapy only when ice was exchanged every 1–2 h and a negative effect in the other patient group where ice was exchanged less frequently every 4 h. This study, however, was supported by a research grant from the cryotherapy device manufacturer, introducing a conflict of interest. Smith et al. 22 found limited benefit of using cold therapy when compared to compression bandages up to 48 h post-TKA in their RCT. Levy and colleagues 20 reported no improvement in postoperative edema when cryotherapy was applied, although this was measured in only 20 of the 80 patients included in the study.
Range of motion
Restrictions in range of motion (ROM) can hinder early rehabilitation. Kullenberg et al. 17 reported an increased range of flexion when cryotherapy was used post-TKA in their study of 86 patients. This study is, however, at risk of reporting bias after the authors failed to state the effects on knee extension. An improvement in ROM postoperatively (measured as flexion) was noted by Levy and Marmar 20 in their RCT comparing the effects of Cryo/Cuff (Aircast, Vista, California, USA) to Robert Jones bandage. Mumith et al. 29 noted further improvement both in ROM and cost when comparing a novel cooling product, Physicool (Physicool Ltd, London, UK) to Cryo/Cuff.
These findings are however in contrast to those from Healy et al.’s 28 study where Cryo/Cuff dressing application was not associated with increase in ROM (measured as extension) postoperatively at any point. Similarly, Gibbons et al. 23 found no improvement in postoperative motion associated with the use of cryotherapy with similar results echoed by Su et al. 30 as well as Schinsky et al.’s 31 study comparing low-cost ice/gel pack against circulating ice water cryotherapy.
Evolution of cryotherapy
Cryotherapy has gradually evolved over time. First generation cold therapy included basic gel packs and crushed ice in plastic bags. Second generation includes circulating ice water promoting cold therapy such as Cryo/Cuff, whereas third-generation devices enable electronic control of continuous cold therapy. 27
A large disparity in the use of cryotherapy worldwide exists due to conflicting evidence relating to its benefits. Third-generation cryotherapy providers stated that this conflicting evidence was linked to improper cooling technique as traditional ice packs are unable to guarantee a sustained fixed temperature during cooling. This has led to the development of new advanced cryotherapy devices providing continuous extended cooling using continuous flow of cold air. Bech et al. 16 compared the use of a continuous cooling icing device (DonJoy Iceman, DJO Canada, Mississauga, Ontario, Canada) against intermittent cooling via a standard ice bag in the first 48 h postoperatively and found no difference in pain or blood loss. Thienpont 32 also noted no difference in postoperative pain, analgesic consumption, postoperative ROM, swelling or blood loss in patients receiving advance cryotherapy versus cold packs. The authors concluded that the higher economic costs of advance cryotherapy conferred no advantages over cheaper and more readily available ice packs.
Cryopneumatic devices
Interest has recently grown in the combined use of compression and cooling therapy through cryopneumatic devices. Maximizing ROM is a major objective post-TKA. Su et al. 30 found no difference for ROM, swelling or functional testing between a cryopneumatic device (GameReady) and ice packs. Similar findings were also reported by Holmström and Härdin 33 in a prospective, RCT for the Cryo/Cuff when compared to epidural anesthesia. However, better outcomes were demonstrated in two-stage bilateral TKAs by Morsi 18 with the use of these devices.
Risks of cryotherapy
Cryotherapy does have potential risks associated with its use. Human skin can be directly affected by hypothermia. Prolonged duration and overly low temperatures applied in addition to excessively high pressures can compromise skin circulation 27 . Frosbite occurs at temperatures around 10°C and prolonged cooling <5°C can result in necrosis and thrombosis. 32 It has been suggested that cryotherapy should be contraindicated in individuals with cold urticaria, cryoglubinemia, and paroxysmal cold haemoglobinuria. 23 In addition, it has been recommended that at least 20 min of cessation should be encouraged between 2-h long cryotherapy sessions 30 .
Conclusion
Management of postoperative pain following TKA still poses a challenge. Nonpharmaceutical adjuncts such as cryotherapy are becoming increasingly popular and have evolved from simple ice packs to more refined devices employing electronically controlled cold fluid or air circulation. Current published evidence supporting its use is controversial. This is potentially due to variation in the devices used and their application (type, frequency, or duration). It is therefore difficult to derive a firm conclusion on the benefits of its use. Further research in the form of multicenter RCTs with representative patient populations is needed to examine the effect of cryotherapy on postoperative pain management, length of stay, and postoperative function post TKA and also to compare the devices available.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.