
Abstract
Deep vein thrombosis and pulmonary embolism, collectively referred to as venous thromboembolism, constitute a major global burden of disease. Although deep vein thrombosis in the upper extremity is less common than lower extremity, it has been associated with similar adverse consequences. We have had experienced with one case of subclavian vein thrombosis and fatal pulmonary embolism after proximal humeral fracture surgery. The purpose of our report is to raise awareness to orthopedic surgeons that pulmonary embolism can occur with proximal humeral fracture surgery and patients with high risk factors should be considered for anticoagulation therapy.
Introduction
Upper extremity deep vein thrombosis (UEDVT) are uncommon, accounting for 1% to 4% of all DVT cases. The annual incidence of UEDVT is about 1/100,000 or 2/100,000. 1,2 Although most of the DVT occurs in the lower extremities, UEDVT is a clinical entity with potentially devastating complications 3 and has similar incidence for the risk of pulmonary embolism. 4 Prompt diagnosis of this condition is paramount, and early intervention is generally recommended to reduce the risk of thromboembolic complications and pulmonary embolism. Although the treatment for UEDVT remains controversial, recent evidence suggests that systemic anticoagulation may limit the risk of thromboembolic complications. 5
Approximately 70–80% of proximal humerus fractures occur in females, and they are the third most common osteoporotic fracture of old people after hip and distal radius fractures. 6 Little evidence exists on the incidence of subclavian vein thrombosis after proximal humeral fracture surgery. 5,7 We present the case of a 57-year-old woman who was diagnosed with an UEDVT post-proximal humerus fracture surgery and died of fatal pulmonary embolism. The patient was informed that the related data would be submitted.
Case presentation
A 57-year-old woman presented to the emergent trauma center with a painful shoulder after falling down the stairs. Examination showed obvious deformity of the right shoulder with a restricted range of motion. She had a swollen upper arm, with no abnormalities with radial pulse and neurological examination. She underwent a radiograph of the right shoulder which showed comminuted fracture of proximal humerus with infraglenoid dislocation (Figure 1). She had no previous surgery or medical problem, no family history of blood clotting disorders, and was not smoking. The preoperative D-dimer blood test (Asserachrom
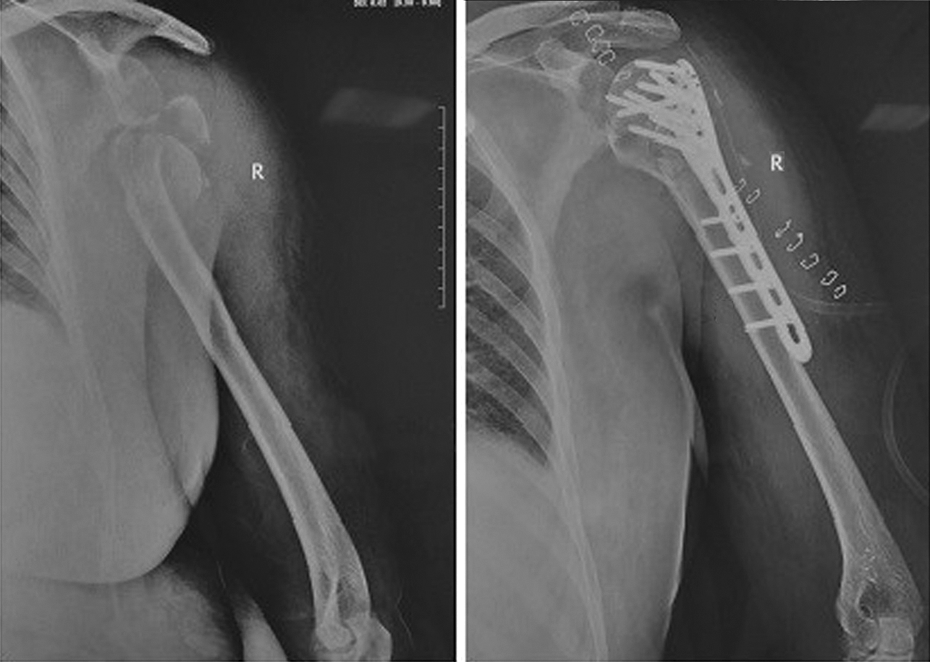
Comminuted fracture of proximal humerus with infraglenoid dislocation (pre- and postoperation).
On the first postoperative day, the shoulder dressing was changed. She was out of bed with sling for the affected limb. The radial pulse was found to be intact, and the neurological function was grossly intact on repeat examination. On the second day, a repeat radiograph showed satisfactory reduction of proximal humerus (Figure 1). On the third day after operation, the patient felt pain and swelling in the affected limb. D-dimer reexamination results was 1.87 μg/ml. Despite the risks and adverse consequences of pulmonary embolism fully informed by her doctors, she was willing to accept a Doppler ultrasonography and refused to take a whole-body enhanced CT. A Doppler ultrasonography was performed and the presence of a thrombus extending the proximal of the right subclavian vein with irregular blood flow was revealed (Figure 2). The patient was placed in a thoracic–humeral bandage for motion restriction. Cardiovascular consultation was asked for therapeutic anticoagulation therapy with the direct oral factor Xa inhibitors rivaroxaban 8 (15 mg twice a day). On the fourth postoperative day 10 a.m. on her way to the downstairs in preparation for her discharge, she suddenly felt chest pain and dyspnea. Five minutes later, she was admitted to the emergency department with unconsciousness. All resuscitation efforts failed, and the patient was pronounced dead. The autopsy revealed that right pulmonary artery lumen was filled with a 11 mm × 4.5 cm emboli, and a large clot was noted in her right subclavian vein. Moreover, no thrombosis was found in the lower extremity veins. The final cause of death was a fatal pulmonary embolism (Figure 3).
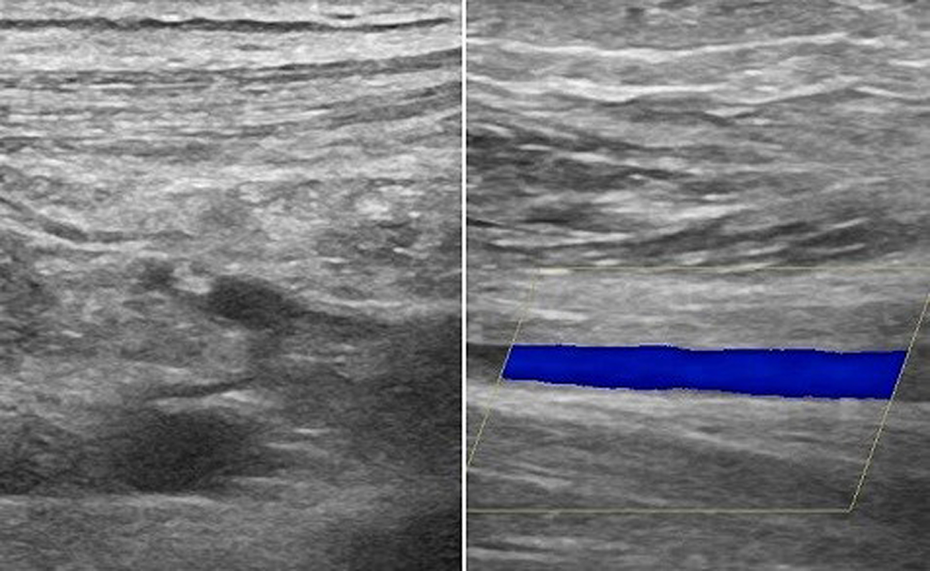
Doppler ultrasound of the right upper extremity showing complete thrombosis of the proximal subclavian vein with irregular flow in the upper arm.

Autopsy pathological photograph of the right pulmonary artery, revealing a 11 mm (diameter) × 4.5 cm (length) emboli filled in the right pulmonary artery lumen.
Discussion
UEDVT is a rare thrombotic disorder, but it has a potential for considerable morbidity in the form of pulmonary embolism. 9 It cannot be diagnosed based on clinical features alone, since the signs and symptoms are not specific. D-dimer and imaging tests, such as Doppler ultrasonography and computed tomography venography, are therefore warranted to confirm or refute the diagnosis. However, D-dimer test and CT venography may be less desirable as a first-line test, since it is low specificity and time-consuming and costly respectively. Doppler ultrasonography is a widely available, noninvasive test and does not require nephrotoxic agents to be administered. 10 A recent systematic review of the accuracy of diagnostic tests for upper-extremity deep venous thrombosis found 97% (95% CI, 90–100) sensitivity and 96% (CI, 87–100) specificity for compression ultrasonography. 11
The knowledge on the cause, complications, and clinical outcome of patients with UEDVT is not well-defined because of the scarcity of the disease and most of the available information is from case reports or studies of small sample size. 4,12 In our report, it is probable that the endothelium of the subclavian vein was injured because of the proximal humerus fracture dislocation. For the more, the application of traction–countertraction technique during operation may have contributed to the development of UEDVT in our patient. Although this patient was a health woman who had no medical problem and history of disorder, she experienced the traumatic fractures and surgery. Moreover, this patient was diagnosed as subclavian vein thrombosis based on the clinical, laboratory, and radiological evidence, as well as subsequently treated with rivaroxaban. Unfortunately, she was died of fatal pulmonary embolism finally confirmed by autopsy. It is not our intention to provide definitive thresholds on which to base therapeutic decisions for patients with high risk factors. Our intention is to emphasize the extremely high mortality of pulmonary embolism and that we should take preventive and treatment measures through comprehensive consideration of all aspects of the patients’ characteristics.
There were few articles concerning pulmonary embolism after upper limb surgery previously. Scott reported a 24-year-old athletic man who had brachial vein thrombosis and pulmonary embolism developed after glenohumeral joint debridement. 13 Rockwood also reported two cases of pulmonary embolism after elective shoulder surgery, 7 but it has no reports about fatal pulmonary embolism after proximal humerus fracture surgery. The patient reminds us that it is necessary for patients with proximal humeral fracture have a Doppler ultrasonography for upper extremity deep vein to refute thrombus.
In summary, the thrombosis of the subclavian vein is rarely documented after surgery and possibly underdiagnosed condition. Orthopedic trauma surgeons must be alert to the possibility that pulmonary embolism can occur after proximal humeral fracture surgery and should consider prophylactic measures for patients with identifiable risk factors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.