
Abstract
Background:
Literature on outcomes of arthroscopic Bankart repair at the intervening time intervals in traumatic recurrent dislocation of shoulder joint is limited.
Study Design:
Case series.
Subjects and methods:
A prospective review of 30 shoulders, aged 20–40 years with clinically and magnetic resonance imaging established findings that were treated with primary arthroscopic Bankart repair and followed up for a minimum of 2 years. Outcomes were evaluated using Rowe score and University of California at Los Angeles (UCLA) scoring system.
Results:
The mean age was 26.40 years. All patients had definite trauma history. Average number of dislocation was 13.77 + 18.435 (range: 3–100). Time duration from first dislocation to surgery was an average of 4.80 + 3.576 years. The average size of the lesion was approximately 31% of the glenoid circumference. The number of suture anchors used for fixation did not correlate significantly with any of the scores. The mean Rowe and UCLA scores were 94.16 ± 9.7 and 33.83 ± 3.32, respectively, at final follow-up. The average duration of hospital stay was 7 days. Of the 30 patients, 2 (6.66%) had dislocation events post-operatively. Returns to pre-injury level were available for 27 (90%) of 30 patients. Multivariate analysis of independent Variables: age; side and number of dislocations, time to surgery, duration of surgery, size of lesion, number of anchors, and concurrent Hill–Sachs lesion, shown to have no significant relationship to outcomes.
Conclusion:
Arthroscopic Bankart repair is an effective and safe technique for treating anterior glenohumeral instability in patients with recurrent traumatic shoulder dislocation.
Introduction
The glenohumeral joint is the most common major joint of the body to dislocate. In general population, the incidence of traumatic shoulder dislocation is 1.7% and it is more common in men, contact athletes and enlisted persons. 1,2 Anterior shoulder instability contributes 90% of all instabilities. 3 The stability of the shoulder joint is imparted by static and dynamic structures. The glenoid socket, whose concavity is deepened by circumferential fibrocartilaginous labrum, the joint capsule and its thickenings, the coracohumeral ligament and the superior, middle and the inferior glenohumeral ligaments and the joint compression provided by rotator cuff and long head of biceps tendon. 4,5
The labrum is a fibrocartilaginous structure that doubles the anteroposterior depth of the glenoid socket from 2.5 mm to 5 mm and deepens the concavity to 9 mm in the superoinferior plane. Additionally, it increases the surface area of contact for the humeral head and thus, enhances the stability of the joint and provides attachment of the glenohumeral ligaments.
The causes of anterior dislocation of shoulder are usually trauma; a sports injury, road traffic accident, assault or fall. It might occur in any situation where an anteriorly directed force acts on the shoulder with the arm in an externally rotated position, or a strong and sudden externally rotating force is applied on the abducted arm and pull of the surrounding muscles during a seizure. 3 Traumatic dislocation or subluxation of the shoulder leads to avulsion of the glenoid labrum from the anteroinferior part of the glenoid rim, the so-called Bankart lesion and elongation of the capsular ligamentous restraints, also. 6 A Bankart lesion is found in over 80% of shoulders with recurrent shoulder instability. 7,8 The frequency of dislocation keeps increasing with time and overhead activity, and it is termed as recurrent when dislocation occurs more than once. 3 Several risk factors have been encountered in recurrent dislocations, include traumatic aetiology of the first dislocation, age, anterior labral periosteal sleeve avulsion (ALPSA) lesion and superior labrum anterior and posterior (SLAP) lesion. Re-dislocation rate is up to 90% in patients under 20 years of age at first dislocation, but only about 10% in patients over 40 years of age. 9 –11 The supporting structures such as the capsules and ligaments become weaker with each dislocation and more susceptible to further dislocation. 12
More than 200 different types of surgeries have been described. However, no single procedure has been found to be absolutely effective. 13 Arthroscopic Bankart repair using suture anchors was introduced in 1999. 14 These arthroscopic procedures address both capsuloligamentous laxity and labral pathologies, hence demonstrate low recurrence and failure rates. 15 –17
The purpose of our study was to evaluate the outcomes of arthroscopic repair of Bankart at the intervening time intervals in traumatic recurrent dislocation of shoulder joint.
Material and methods
Thirty cases were enrolled in the prospective study, which was conducted at the Institute of Army Base Hospital, between June 2011 and May 2013. Patients, who have a history of traumatic recurrent shoulder joint dislocation with Bankart lesion underwent primary arthroscopic Bankart repair using suture anchors, with a minimum follow-up of 2 years. All surgical procedures were performed by two different surgeons. We included those patients aged 20–40 years of either sex, recurrent anterior dislocation of shoulder joint with clinically and magnetic resonance imaging established findings.
Exclusion criteria for this study were (1) traumatic or multidirectional instability; (2) posterior instability; (3) previous surgery of the affected shoulder; (4) shoulder dislocation for the first time; (5) patients having large Hill–Sachs lesion or a large bony Bankart lesion (defect >25% requiring reconstruction); (6) full-thickness rotator cuff tears; (7) evidence of infection, avascular necrosis of humeral head, chronic dislocation, inflammatory or degenerative glenohumeral arthropathy, frozen shoulder; (8) psychiatric illness that precludes informed consent and (9) symptoms of impingement syndrome – rest pain at shoulder referred to insertion of deltoid, night pain, painful arc of shoulder. Written informed consent was obtained from patients for publication and accompanying images.
Surgical technique
The same arthroscopic technique was used in each case which was performed under general anaesthesia in the supine position. Surgery was performed in the lateral decubitus position. Stability testing was performed to confirm clinical diagnosis before arthroscopic evaluation. Operative extremity was placed in 45–60° of abduction and 20–30° of forward flexion with twin traction unit to provide optimal exposure for instrument placement, distraction and internal rotation of the glenohumeral joint.
The bony landmarks and portals were marked with a skin marking pen. The arthroscope was introduced via a standard viewing posterior portal and the joint was inspected in a systematic way. The site and extent of the Bankart lesion was noted and the associated pathology was addressed. Two anterior working portals were made by an outside-in method for inspection of the rotator cuff, the glenohumeral ligaments and the subscapularis tendon. Then, complete mobilization of avulsed and fibroses labrum was done from its retracted position. The glenoid rim was made raw using a shaver, burr, or rasp as suitable. Once the labrum is reducible, appropriate number of suture anchors according to the size of the lesion were inserted one by one from inferior to superior along the glenoid rim. After the insertion of each anchor, one of the limbs of the suture was pulled through the overlaying loose labrum with the help of an angled suture passer. The labrum was tied down over the glenoid edge, reattaching it firmly to its proper position. Throughout this study, the same type of suture anchors were used. These were titanium-made and 2.8 mm in size (Arthrex, Naples, FL, USA). Once the required number of anchors were inserted and tied to the satisfaction of the surgeon, a final inspection was done of the repaired capsulolabral complex. Capsular plication was not performed with the Bankart repair. Any posterior labral pathology was addressed in a similar fashion. In cases where a type II SLAP tear was also present, a shaver was used to debride the superior glenoid neck. Intervention for Hills–Sachs lesions and glenoid defects was not made in any case. The scope was then withdrawn and the portals were closed using skin sutures only. The sutured wound was dressed with compressive dressing and a shoulder immobilizer was applied.
Post-operative management
All the patients were rehabilitated according to the same protocol. In the first 2 weeks, a sling was used and maintained continuously, being only removed for pendulum exercises and for elbow and wrist flexion–extension. At this moment, the patients were evaluated by the surgeon and physiatrist. At the 3rd and 4th weeks, the priority was the range of motion (ROM). Active-assisted ROM in the plane of the scapula was progressed to 90°. After 4 weeks, the immobilizer was discontinued and active-assisted ROM was progressed in forward flexion and external rotation. Patients were also taught to do isometric rotator cuff exercises during this period. From 6 to 12 weeks, gradual strengthening was added. Non-contact sports were allowed after 3 months. Contact sports were allowed after 6 months.
Outcome
Preoperative assessment including age, mechanism of injury, number of dislocations and duration after first dislocation to surgery was noted. Intraoperative findings including associated and size of lesions, and number of anchors used in the repair were documented. Post-operative assessment included recurrence and any other complications. Outcomes were evaluated at 3 months, 6 months, 12 months and 2 years using Rowe score 18 for stability, ROM and overall function, and University of California at Los Angeles (UCLA) 19 scoring system for pain and function.
Statistical analysis
Statistical analysis was done in two sets using the Statistical Package for the Social Sciences (SPSS) software version 16. In the first set, multivariate analytical tests were done to calculate the correlation between the various patient parameters and the outcome scores. Limit for significance of correlation coefficient was used for the extent of correlation. In the second set, the progression of the various scores over time was analysed. Trends of score improvement were studied to detect at what period of time the significant changes and improvements were taking place. In the case of Rowe and UCLA scores, which are composed by adding several sub-scores, each of the sub-scores was analysed separately. Pairwise comparison was done between each of the scores to see statically significant changes of scores over time periods. p Values <0.05 were considered statistically significant.
Results
The demographic and individual variables are summarized in Table 1. Analysis of the outcome related to sex was not possible as the number of female patients (n = 2) was not enough for a valid statistical analysis. The most frequent cause included sports injuries (56.66%), followed by fall directly onto the shoulder (16.66%), lifting weight (16.66%), road traffic accidents (6.66%) and in one patient the cause was jerk during starting a power generator engine. All 30 shoulders had a Bankart lesion. Associated lesions are reported in Table 2. The number of suture anchors used in patients varied from 3 to 5 depending upon the type and size of the lesions. On average, 3.86 anchors were used per case. Average operating time was 94 min (range: 55–130 min).
Demography and individual characteristics.

aData are reported as mean ± SD or n (%).
Associated lesions.

HSL: Hill–Sachs lesion; SST: subscapularis tendon tear; BC: biceps contusion; GD: glenoid defect; SLAP: superior labrum anterior and posterior.
Outcome measures
Risk factors and their coefficients are shown in Table 3. There were no significant differences in Rowe total score before surgery and at 3-month follow-up, but after 6 months there was a steady and significant improvement up to the 2nd year. Pain scores showed that no significant improvement occurred in the scores at the 3rd month but a significant improvement was seen from the 6th month onwards. Patient satisfaction with the affected shoulder improved steadily from the preoperative state, at every follow-up until 2 years. Variation of scores with time was shown in Table 4. Multivariate analyses tests were done to evaluate independent risk factors predicted UCLA and Rowe scores (Table 5). The number of suture anchors used for fixation did not correlate significantly with any of the scores. Two shoulders (6.66%) had dislocation events post-operatively. Both were traumatic falls while climbing rope, one was dislocated at 16 months and the other was at 20 months after surgery. There was no subtle instability in any other patient. Blood loss was minimal in all cases. No patients required post-operative intensive care or blood transfusion for any reason. There were no neurological or vascular injuries. No post-operative infection was noted. However, the average duration of follow-up was 23.17 months. We were able to follow up 27 shoulders for a total of 2 years, 30 shoulders until their 1 year. Two were excluded from the study due to traumatic re-dislocations and one shoulder was lost to follow up at 2 years.
Variation of score with time.a
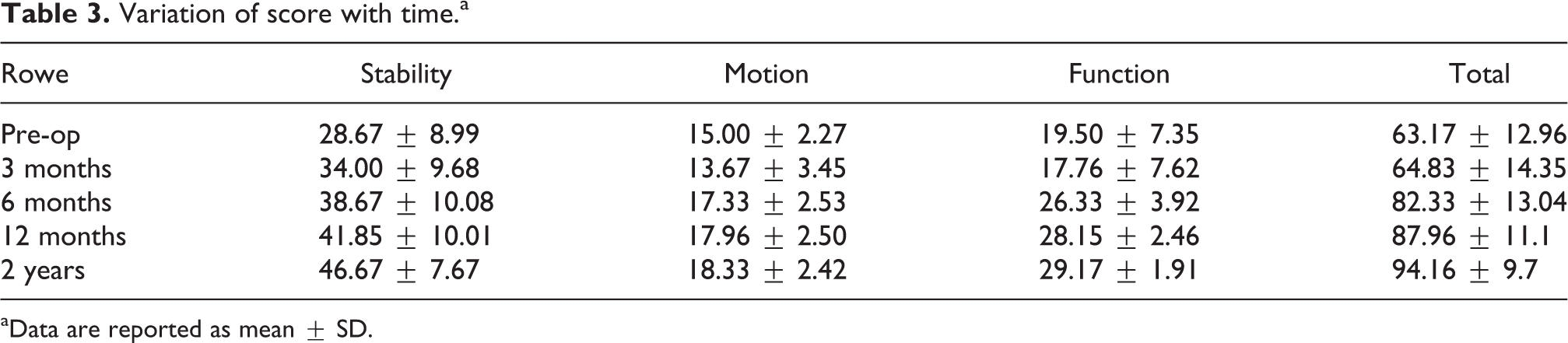
aData are reported as mean ± SD.
Variation of score with time.a

UCLA: University of California at Los Angeles.
aData are reported as mean ± SD.
Independent risk factors predicting outcome identified by multivariate analysis.
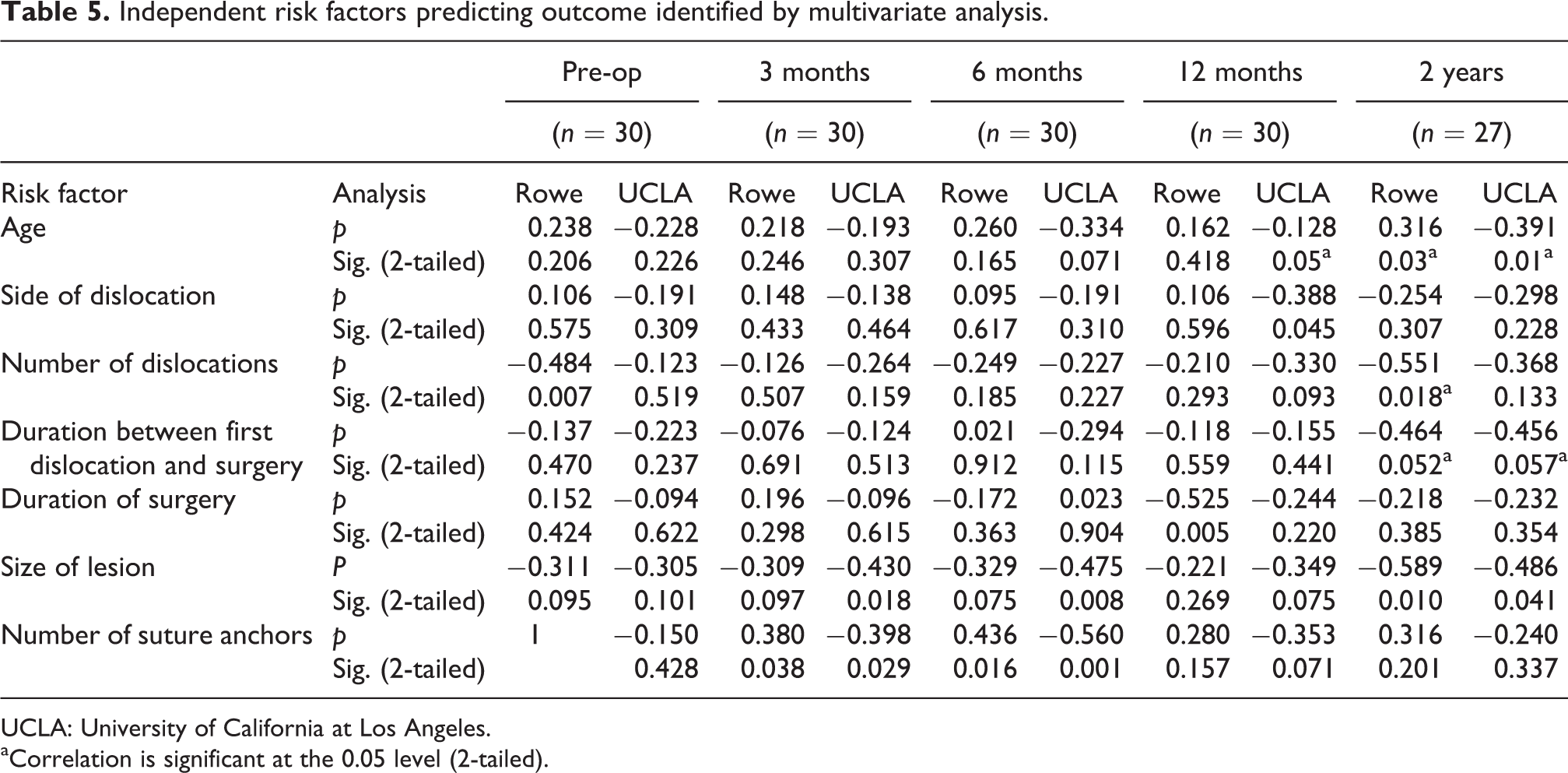
UCLA: University of California at Los Angeles.
aCorrelation is significant at the 0.05 level (2-tailed).
Discussion
The principal findings of this study suggest that arthroscopic Bankart repair is an effective surgical option for traumatically induced shoulder instability in adolescents at time intervals follow-up. In our study, the mean age was 26.40 years (range: 20–40 years). Fourteen patients were under 25 years of age, consistent with other studies. Marquart et al. 20 had an average of 25.3 years, Hayashida et al. 21 reported an average age of 26 years, in Cho et al. 22 it was 24 years and in Carriera et al. 15 it was 27 years.
In our series, the number of female patients (n = 2) made it impossible to perform any valid analysis on whether sex is a significant factor influencing the outcome. Males are generally more involved in a variety of sports and occupations requiring heavy lifting, so they stand a greater risk of re-injury after the first dislocation. In our series, side and dominancy did not have any bearing on the outcome of the surgery as per the scores. In Hayashida et al., 21 there were 30 right and 17 left shoulders, and 32 of the 47 total were dominant. Seedek et al. 23 series had 24 right and 16 left shoulders. However, they have not commented upon the relevance of the specific side of the injury on functional outcome and the occurrence of re-dislocation.
The initial traumatic event was noted in all the patients in the study. This matches published studies, where sporting injuries tend to be the commonest cause of the first dislocation. 21,23 A few of our patients had trauma of an unusual nature causing their dislocation, which included a fall from bed and fall of heavy object over shoulder.
In our series, the average number of dislocations was 13.77 + 18.435. We analysed that any number of dislocations sustained before surgery did not affect the post-operative functional outcome. Marquart et al. 20 reported the average number of dislocations at 5.5, before the patients underwent surgery. The patients in Seedek et al. 23 series had an average of 7.7 dislocations, whereas O’Neill et al. 24 and Carreira et al. 15 examined the preoperative number of dislocations to be 3 and 8.3, respectively. Other studies too have not noted any effects of the number of dislocations sustained per se on the post-operative results. 15,20,23,24 In our series, the patients had undergone more number of dislocations, that is, the condition had become more disabling before the patients sought medical help. This is presumably due to the patients’ lack of awareness about the nature of the problem or the fact that it is amenable to surgical correction. Also, the relative difficulty of accessing a tertiary healthcare centre in our healthcare setup affects the help-seeking behaviour of most of our patients.
Our analysis showed that the duration from first dislocation to surgery was related to the outcome after 12-month follow-up. It was an average of 4.80 + 3.576 years. The Pearson correlation was negative, showing that the longer the duration, the worse the result. Seedek et al. 23 reported 39.6 months was an average duration. Carreira et al. 15 found this figure to be 47 months, whereas O’Neill et al. 24 had 10 months of average duration. Studies have shown that the long-standing the lesion, the more likely the Bankart lesion is to become an ALPSA, so this association seems to be logical. The presence of an ALPSA lesion or degeneration in the avulsed labrum might be associated with a worse prognosis when repaired arthroscopically. 10 Similar to the case of the number of dislocations sustained, this discrepancy may be due to lack of awareness and health-seeking behaviour in our patient population. This finding further supplements our observation that patients in our healthcare setup wait longer till the condition becomes more disabling before seeking medical help.
In present study, we have evaluated the size of the lesion intraoperatively and quantified it in degrees considering that total glenoid circumference to be 360° suggest each hour on the clock face is equivalent to 30° of lesion. For example, a lesion from 2 o’clock to 5 o’clock position encompasses 90° or 25% of the glenoid circumference. In our study, the average size of the lesion was approximately 31% of the glenoid circumference. We could not find any reference in the available studies about the size of the lesion per se to make a comparison of this finding and its possible significance. In our study, the size of the lesion did not have any significant correlation with any of the scores post-operatively.
In our study, 11(36.66%) shoulders had no associated lesions other than the Bankart. In remaining shoulders, 19 (63.33%) had a Hill–Sachs lesion and 1 (3.33%) had a bony glenoid defect <25% not requiring reconstruction. The presence of a Hill–Sachs lesion had been reported to be 100% (54/54) by Marquart et al., 20 whereas in Seedek et al. 23 series it was 15% (6/40). The occurrence of a SLAP tear had been reported to be 5% (2/40) by Seedek et al., 23 whereas Carreira et al. 15 reported a SLAP tear in 27% (18/69) of his patients. The presence of a Hill–Sachs lesion did not have any correlation with the outcome in our patients. Our results were consistent with O’Neill DB 24 who had noted no influence of a Hill–Sachs lesion or a small osseous Bankart lesion on the operative outcome. The number of patients with subscapularis tendon tears and biceps tendon contusions were few to make a valid statistical analysis.
Seedek et al. 23 reported the average operating time was 72 min. In our study, patients were reported much later. Therefore, the contractures and fibrosis that occurred in the avulsed labrum were more extensive and hence obviously taken longer time to mobilize adequately. Our statistical analysis had yielded a significant correlation between lower preoperative shoulder scores and longer operating time. No correlation was however found between the operating time and the post-operative scores at any of the follow-ups. There was no statistical correlation between preoperative shoulder scores and the number or duration of dislocations and associated lesions.
In the current study, a mean of 3.86 suture anchors were used. In Seedek et al. 23 series, it was reported that stability had been achieved with the use of fewer than three suture anchors. Patients who had only two suture anchors did not have a higher rate of recurrence. In a study by Watch et al., 25 they suggested that the use of fewer than four suture hooks could have been one of the reasons for failure. A systemic review showed that patients operated using two anchors had a higher incidence of recurrence instability (35%) compared to patients operated using three or more anchors (20%). 26
The studies published in the literature do not give the specific scores at the intervening time intervals and straightaway state the scores at the end of the study. On comparison of the scores, the preoperative Rowe score in Marquart et al. 20 study and Hayashida et al. 21 study was 31.8 ± 12.8 and 30.8, respectively. Cho et al. 22 reported the components of the score separately. His preoperative Rowe stability score was 17 ± 10, motion score was 18 ± 2 and function score was 10 ± 0, adding up to a total mean preoperative Rowe score of 45 ± 11. The final total Rowe scores in the other studies mentioned above were 92.1 ± 19.1, 91.3 and 93 ± 10, at average follow-ups of 3.7 years, 28 months and 24 months, respectively. 20 –22 This final score of our study correlates well with the aforementioned studies. In our study, the UCLA system also followed the pattern of the Rowe score. Most of the sub-scores and the total score made no significant progress in the 3rd month, with the scores improving from the 6th month onwards. This is similar to the value reported by Seedek et al. 23 ; they also used the UCLA system for evaluation in their series. Their preoperative total score was 20.15 ± 4.03 and at the end of follow-up was 32.07 ± 4.82. The trends in the individual subheadings were not described separately in their report. Most of the sub-scores and the total score made no significant progress in the 3rd month, with the scores improving from the 6th month onwards.
The average duration of hospital stay was 7 days, significantly longer in our study. It was mentioned that this stay included the period allotted for pre-op investigations and pre-anaesthetic clearance. Also, after the surgery, patients were not discharged immediately but were kept until wound inspection had been done on the second post-operative day and physiotherapy under direct supervision till the 4th or 5th day.
Marquart et al. 20 reported a failure rate of 7.5% (4/54). Of the four re-dislocations, three occurred after significant trauma. Hayashida et al. 21 had a failure rate of 6.4% (3/47). Among the three failures in their study, two patients had a subluxation about 16 months after the surgery, and one patient re-dislocated after a significant injury during sports 30 months after the surgery. Cho et al. 22 reported a failure rate of 4.9% (3/61), and all three of the re-dislocations in their patients occurred during sports after significant trauma. Carriera et al. 15 reported a 7% failure rate in their series. In the present study, two shoulders (6.66%) had dislocation events post-operatively. Both were traumatic falls while climbing rope, one was dislocated at 16 months and the other was at 20 months after surgery, which were consistent with reported studies.
The outcome scores at the end of 2 years were comparable with the results of other studies using the same scores. A significant finding, noticed in both the scoring systems, was that the scores showed no significant improvement at 3rd month follow-up but had improved at the 6th month, implying that most of the clinical and functional recovery after surgery becomes apparent between the 3rd and 6th month. Returns to pre-injury level were available for 27 (90%) of 30 patients.
A limitation of our study was short follow-up. Although the power of the test calculated was above 80%, indicating that the sample size was adequate, a larger patient group would be preferable so that the data are more valid. The lack of a control group and randomization to eliminate the various kinds of bias were other drawbacks of this study. Nevertheless, this study does represent one of the largest investigations of Bankart tears in this specific, homogeneous population.
Conclusion
Arthroscopic Bankart repair is an effective and safe technique for treating anterior glenohumeral instability in patients with recurrent traumatic shoulder dislocation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.