
Abstract
The moment arm of gluteus medius proportionated to distance from femoral head tends to be decreased postoperatively in valgus-impacted femoral neck fractures treated by in situ internal fixation. The aim of this article is to introduce a new gentle technique to correct the deformity. The innovative technique of Minimally Invasive Closed Reduction for Impacted Femoral neck fractures (MICRIF) mainly focused to disimpact valgus neck fractures into anatomical position. Patients were positioned on the fracture table to fix the hip joint in abduction and internal rotation. A 2.4-mm diameter Kirschner wire was inserted a few centimetres outside the iliac crest piercing the acetabular beak to enter the femoral head, followed by repositioning of the lower extremity from abduction into neutral. This method provides satisfactory anatomical reduction. Thereafter, a surgical implant was applied to osteosynthesize the reduced fracture. This simple technique effectively provides anatomical reduction in valgus impacted femoral neck fracture.
Background
The occurrence of femoral neck fractures is increasing rapidly in ageing societies, such as in East Asia. Non-displaced or valgus-impacted femoral neck fractures are generally stable and successfully fixed in situ without anatomical reduction. 1 –3 Bony impaction at the fracture site contributes to bony healing with a low rate of non-union and femoral avascular necrosis. 4
On the other hand, postoperative functional results of this fracture decrease, compared with preoperative function. 5 We believe surgeons should be aware of factors that may lead to decreased postoperative functional levels. In our outpatient service, a number of patients with valgus-healed femoral neck fractures complain of weakness around the operated hip. Using the mean Harris Hip Score, Song et al. 6 reported that the functional score was significantly lower in a group with a valgus impaction of greater than 15° (82.0 score) when compared to those with a less than 15° valgus impaction (88.8 score) (p = 0.041). This result may be based on the fact that femoral neck fractures often combine with horizontal shortening or a decreased offset that may lead to weakness during abduction. 7,8 Our previous study also demonstrated that a 15° valgus impaction, using biomechanical computerized bony models, decreases the moment arm of abduction by approximately 10% and that only abduction of hip joint at the operated side was significantly lesser when compared with the healthy contralateral side during clinical examination. 9 This clinical result coincides with the report of Zlowodzki et al. 8
To amend for the faults of conventional treatment, it is worth reducing valgus impaction of femoral neck fractures into the anatomical position. However, to our knowledge, only few groups address this problem. 10 To allow for practical and general use, the anatomical reduction procedure should be simple and effective, taking into account the minimal operative incision size for implanting, without devastating surrounding anatomical circulatory structures. To the best of our knowledge, there are no methods mentioned to resolve this problem.
The purpose of the current study is to introduce an innovative closed reduction technique to disimpact valgus femoral neck fracture into the anatomical position. Although we have described the rationale behind it, contrasting anatomical reduction with in situ fixation (valgus position) over postoperative results is out of the scope of this study.
Technique
Minimally Invasive Closed Reduction for Impacted Femoral neck fracture (MICRIF), provisionally fixated femoral head through trans-acetabulum
Prior to scrubbing, patients with impacted fractures were positioned on the fracture table and closed reduction was attempted by gradual application of longitudinal traction or lateral force to the thigh under image intensifier observation in the anteroposterior (AP) view. Since the traditional closed reduction technique was mostly unsuccessful, we proceeded to perform our reduction technique. First, surgeons should confirm the concerted motion between the femoral head and the intertrochanteric lesion during rotation. The arm of the fracture table was fixed in abducted position and in internal rotation, so as to sustain a plane connecting the femoral head and neck horizontally, considering anteversion of the proximal femur. If combined with a sagittal plane deformity of retroversion, a downward manual reduction force was applied on the anterior thigh. Once reduction was confirmed through an axial view, bandaging of the distal thigh to the fracture table would effectively maintain reduction of retroversion during the succeeding valgus correction.
After scrubbing, minimum invasive reduction commenced under image intensifier observation in AP view. (1) A long needle was introduced caudally following a course 1QFB lateral to the iliac crest, advancing the needle tip to reach the acetabular beak and not the femoral head. Directing the needle at a slightly oblique angle against the horizontal line, anterior to inferior, may facilitate this step. (2) Using the needle as a guide, a 2.4-mm diameter Kirschner wire was manually inserted through the gluteus muscles aiming for the same target area as the needle (Figure 1). The Kirschner wire was directed to the centre of femoral head in lateral view, when possible. (3) It was then drilled forward for about 2 cm, piercing the acetabulum and entering the femoral head. This manoeuvre stabilizes the hip joint in the abducted position. (4) The arm of the fracture table was loosened. (5) The lower extremity was repositioned from abduction into the neutral position until the valgus would be disimpacted into the acceptable anatomical position (Figure 2). During disimpaction, slight traction force is applied to the leg, while supporting the patient’s lower thigh. Surgeons must be cautious of pivoting motion of the traction apparatus to avoid compression at the fracture site. (6) Afterwards, internal fixation system proceeded.

A Kirschner wire travelling from 1QFB lateral to iliac crest, outside the iliac wall and piercing the acetabular beak into femoral head.
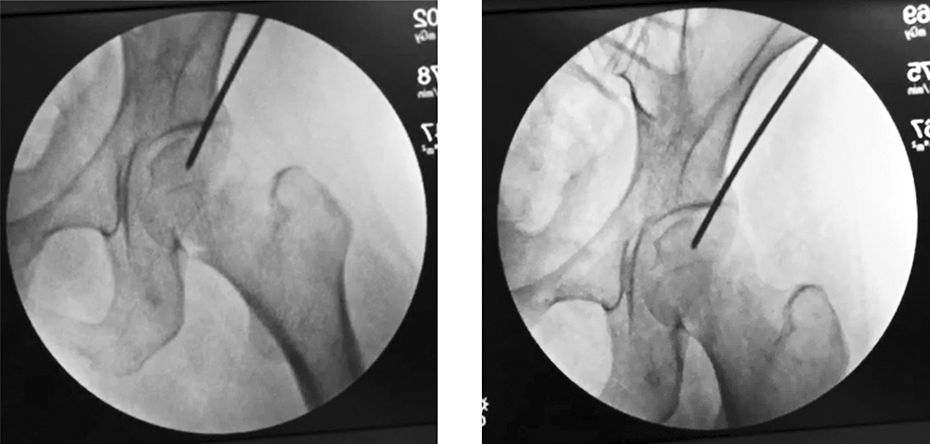
Percutaneous trans-acetabular reduction method. Provisionally fixed in abduction (left). Manual reposition of the leg into the neutral position leads to anatomical reduction of the fracture (right). A slight traction force to the leg should be applied to preclude compression.
Ethics approval and informed consent
This study was approved by the Ethical Review Board of our Hospital. All patients signed a written informed consent before enrollment into this study.
Discussion
Our reduction method (MICRIF)
Our closed reduction with fixation through the trans-acetabulum is a relatively simple technique that provides for successful anatomical reduction. This was confirmed by the intraoperative image intensifier. There are three noteworthy features of this method: (1) “joystick” manoeuvring of the Kirschner wire through tight soft tissues to disimpact the fracture is unnecessary. Altering the position of the operative limb could effectively achieve the anatomical position. (2) The Kirschner wire in the femoral head could be tightly immobilized to the acetabulum as it successfully transfixes the adjacent osseous structures. An additional Kirschner wire beside the first wire would further enhance stability, if bone quality is deemed fragile. (3) This technique does not require rotational motion, hence lesser risk of compromising the nutritional vessels surrounding the femoral head.
There are several articles proposing repositioning of valgus impaction. Lorich et al. 10 suggested a percutaneous technique where two wires are positioned superior to the greater trochanter into the fracture line before attempting cranial reduction via a “joystick motion”. Mahajan et al. 11 introduced method to transfix the femoral head into the pelvic tear drop, which contributes to reduction of a displaced varus deformity, although not specifically for a valgus impaction. Our proposed technique may be similar to Mahajan et al., 11 although their anatomical reduction may be difficult to obtain with the above-mentioned technique as tissue structures such as the iliotibial band, the gluteus medius, the gluteus minimus and tight fascia may hamper the manipulation. In addition, the method may involve some risk to intra-pelvic vital structures to obtain definite purchase of the guide pin.
The approach of Watson and Jones involves making a 10 cm or more skin incision to allow for muscular retraction. 12 This may be an alternative choice for displaced fractures and less applicable to impacted fractures. The skin incision is quite large and disproportional for a small implanting procedure.
Another indication for the management of displaced fractures in young patients
Percutaneous anchorage of the femoral head to the acetabulum would facilitate the chance of successful closed manipulation to obtain near-anatomical reduction. Therefore, even in young patients with displaced femoral neck fracture, MICRIF would be a worthwhile manoeuvre to attempt before proceeding to a formal open reduction. We expect this technique will simplify ordinal manual reduction.
Implant for preserving anatomical reduction
After anatomical reduction has been accomplished, surgeons are required to utilize implants for osteosynthesis such as a fibular allograft, 10 Hansson Pinloc 13 and a novel locking plate, 14 expecting to maintain anatomical reduction for disimpacted valgus femoral neck fractures without a recurring valgus deformity.
Clinical results of anatomical reduction
In our limited experience, we have attained acceptable anatomical reduction. Almost 30 cases in less than 3 years with this technique required no additional method for reduction. We believe this technique easy to perform even less experienced surgeons.
There were no occurrences of wire breakage, acetabular fractures, nor early osteoarthritic changes around the pin insertion as there was minimal cartilage damage. However, results regarding bony union, avascular necrosis, early functional recovery and measurement of muscular strength are beyond the range of this current study.
Conclusions and future direction
This current study introduces a new and simple method that enables anatomical reduction of valgus impacted femoral neck fractures. Further studies will be needed to demonstrate better functional recovery and lesser postoperative complications among anatomically reduced patients, until this technique is advocated as recommended practice. We suggest surgeons to initially try our closed reduction technique (MIRCIF) in patients with moderate or severe valgus impaction, or in the young patient with displaced femoral neck fractures, otherwise worse prognosis is deemed.
Footnotes
Acknowledgements
The authors acknowledge Professor Shinichi Yoshiya, Department of Orthopedics, Hyogo Medical College, for his long-term encouragement and suggestion; Michael Teraoka for his English correction; and Shunsuke Takahara, Department of Orthopedics, Hyogo prefectural Kakogawa Medical Centre, for naming this technique.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.