
Abstract
Purpose:
Ensuring compliance to treatment protocol, especially regular visit to treating facility, is an important aspect of clubfoot management. However, the factors affecting compliance to follow-up schedule are myriad.
Methods:
A cross-sectional study was undertaken among caregivers of clubfoot patients from a tertiary referral clubfoot clinic in a developing country. Hospital records were reviewed to collect demographic data and subjects were classified as either “regular” or “irregular” if they missed ≤3 and >3 scheduled hospital visits, respectively. Various factors that could affect compliance such as family size, number of children, literacy of caregiver, occupation of breadwinner, and time taken to travel to hospital were studied. Caregivers were probed regarding the reason for their irregularity.
Results:
A total of 238 patients were included, of which 138 formed the “regular” group and the rest 100 formed the “irregular” group. Patients in the regular group were significantly younger (mean age 43.8 months) compared to the irregular group (59.8 months; p = 0.001). The mean follow-up period in the regular group was 28.1 months and in the irregular group was 33.8 months. On univariate analysis, age, duration of follow-up, and transport duration were found to be significant between the two groups. However, multivariate analysis revealed that female children with clubfoot are more likely to be irregular as compared to males (p = 0.038).
Conclusion:
In a developing country setting, higher age and being a female child are associated with irregularity to hospital visit protocol. At clubfoot clinics, identifying these children and counseling their caregivers might improve compliance.
Introduction
Clubfoot is the most common congenital deformity of the extremities with an incidence about 1 in 1000 live births per year worldwide. 1,2 With the advent of Ponseti method of treatment, it is well established that most clubfoot patients can lead a near-normal life when they are adequately treated in childhood. 3 However, neglected patients suffer from lifelong disability and handicap.
The challenges to clubfoot treatment in developing countries are very different from the rest of the world. Our study tries to identify those children who are likely to miss hospital visits in India. Our hypothesis was that female children, especially those in families with three or more children, get neglected and miss scheduled appointments at clubfoot clinic.
Materials and methods
A cross-sectional study was conducted at a tertiary referral clubfoot clinic in India from January to March 2014. We included all patients registered with our clubfoot clinic and had completed at least 6 months of follow-up. We excluded patients aged more than 18 years, those who did not consent for the study, and those who could not be contacted with best possible efforts. Hospital records were reviewed to collect necessary demographic data and follow-up visit data. Patients were divided into two groups: “regular” group who missed ≤3 scheduled follow-up visits and “irregular” group who missed >3 visits.
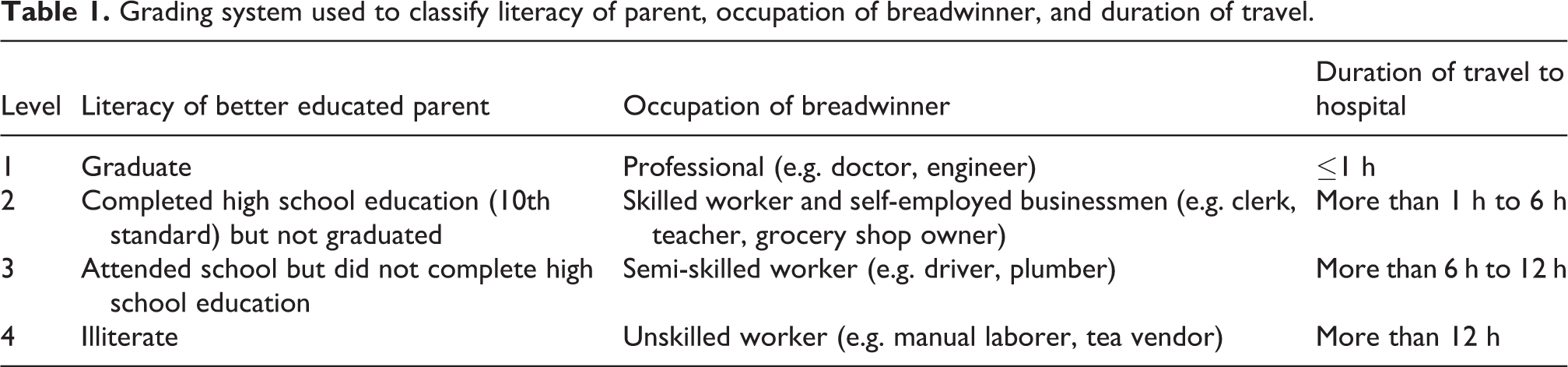
Caregivers of patients were contacted during the scheduled hospital visit, and a questionnaire was administered after taking consent. Those who missed the hospital visit were contacted over phone and the same questionnaire was completed. Caregivers were probed regarding the family size, number of living children, literacy of parents, occupation, and duration taken to travel to the clinic. Caregivers in the “irregular” group were probed regarding the reason for their irregularity. The collected data were tabulated. Family size was classified as “small” when the family had ≤2 children and as “large” if it had ≥3 children. Literacy of parent, occupation of breadwinner, and duration of travel were divided into four levels. The levels for literacy and occupation were adapted from updated Kuppuswamy’s socioeconomic scale (see Table 1). 4 Statistical analysis was performed using STATA statistical software STATA version 11.0 software (Stata Corporation, College Station, TX).
Grading system used to classify literacy of parent, occupation of breadwinner, and duration of travel.
Results
Of the 251 patients enrolled, 13 could not be contacted leaving a total of 238 patients for final analysis (see Table 2). The regular group had 138 patients, and the irregular group had 100 patients. Patients in the regular group were significantly younger (mean age 43.8 months) compared to the irregular group (59.8 months; p = 0.001). The male:female ratio of the regular group was 3.2:1 and of the irregular group was 1.9:1. Bilateral affection was more common in both groups (54% in both groups). Syndromic association was noted in 18% patients in the regular group and 22% patients in the irregular group, while the rest had idiopathic clubfoot.
Comparison of variables between the two groups.

Abbreviations: UL: unilateral; BL: bilateral
aThe boldface values indicate significant difference between the two groups.
The mean follow-up of patients in the irregular group (33.8 months) was significantly higher than the regular group (28.1 months). Twenty-four percent of the patients in the irregular group belonged to a family with three or more children as against 15% in the regular group. At least one parent was a graduate in more than 40% of the cases in each group. In most cases, in both groups (approximately 78%), the breadwinner of the family performed either a level 2 or a level 3 occupation. These data demonstrate that the two groups were similar with respect to education and economic factors. Ninety-one percent patients in the regular group had to travel for 6 h or less to reach the hospital, while 24% of those in the irregular group had to travel for more than 6 h (p = 0.022).
Multivariate analysis was performed by considering statistically significant factors and those hypothesized (see Table 3). A logistic regression model was used. The factors that qualified for the analysis include age, sex, family size, duration of follow-up, and travel time. Duration of follow-up and travel time lost their significance, while family structure remained nonsignificant. Only two factors, age and sex of the child, remained significantly different between the two groups. A female child is 2.6 times more likely to be irregular than a male child.
Multivariate analysis using logistic regression model performed on factors at 15% level of significance.

aThe boldface values indicate significant difference between the two groups.
Of the reasons cited by caregivers in the irregular group for being irregular, overcrowding of the hospital tops the list, with 43% respondents feeling so (see Table 4). One-third of the respondents experienced difficulty in transportation, while another third encountered problems within family. Seventeen parents were irregular because they erroneously thought that further follow-up was not required as the foot “appeared” normal. Subsequent pregnancy hampered regular hospital visit in 15% of respondents.
Reasons cited by guardians of children in irregular group for irregularity in follow-up.a

aCertain caregivers had multiple responses.
Discussion
The management of clubfoot has witnessed a drastic change over the past three decades. Ponseti method of casting and bracing has gained universal acceptance among orthopedic community. 3 While most patients who stick to the treatment protocol lead a fully functional life, relapse is common among treatment defaulters. 5 It is difficult to foresee which patient will relapse after complete correction. However, relapse, if diagnosed early, can be treated appropriately and future disabilities can be avoided. 6 Thus, the importance of visiting the treating hospital at scheduled date cannot be overemphasized.
Numerous factors can affect the regularity of hospital visit. Several authors, while attempting to study these factors, administered questionnaires to physicians providing clubfoot care. 13 –15 In our study, we administered the questionnaires directly to caregivers of clubfoot patients thus reducing observer bias. Further, our study had better power compared to many other studies, as we recruited a relatively large sample of 238 patients. 2,7 –9
It is well-known that challenges faced by developed, developing, and underdeveloped countries in providing health care are very different from each other. Pirani and Carlson assessed the factors affecting compliance to treatment in Uganda. 2 Despite excellent results, around 40% of children failed to complete the phase I treatment of Ponseti method. Overcoming various hurdles, they surveyed 10 patients and found that inability to pay for transportation, women relocating to different villages, and lack of support from child’s father as important reasons for noncompliance. These results were confirmed by Kazibwe and Struthers, again from Uganda, wherein they found significant association between compliance to clinic visit and distance traveled, transport costs, and family support. 8
In our study, financial issues played negligible role as both groups were similar with respect to occupation of the breadwinner. Although we did not find significant association between duration of travel and irregularity to hospital visit on multivariate analysis, about one-third of the caregivers of irregular patients cited difficulty in transportation and crowded hospital as reason for their behavior.
On the other hand, Dobbs et al., from United States (a developed country), reported that recurrence following Ponseti method was more common if parental education was high school or less. 5 They did not find significant association between noncompliance and gender, race, parental marital status, source of medical insurance, or parental income. In our study, both groups were similar with respect to literacy of parent. However, age and sex had an influence on regularity as subjects in the irregular group were significantly older. We also found that a female child is 2.6 times more likely to be irregular as compared to a male. This observation is important because the Indian society usually considers male child to be more “precious” than females. This has been well documented by the high rate of female infanticide and feticide in India. 10,11 But the fact that these social and cultural beliefs are affecting proper follow-up in clubfoot patients is something new to us. In a country like India where literacy rate is improving and health care system is becoming more efficient, deep-rooted cultural beliefs are presenting a major obstacle in ensuring appropriate care of clubfoot children.
Our study has few limitations. We did not look into the level of correction and compliance of bracing. Numerous studies have assessed factors affecting bracing compliance and level of correction. 12
They were primarily aimed at studying the effectiveness of bracing protocol and challenges faced. It is now well established that in a corrected clubfoot, bracing can be discontinued after 4 years of age but follow-up needs to continue up to skeletal maturity.
Further, even compliant children can have under-corrected clubfoot if they have complex clubfoot. As our primary aim is to assess the factors affecting the intentions of the caregiver and the difficulties faced by them, we preferred regularity of hospital visit as a marker for compliance than the level of correction.
On conclusion, social beliefs (female children being considered less “precious”/“important” than males) are now presenting a major obstacle to clubfoot management in India. Compliance to hospital visit decreases as the length of follow-up increases. These factors are frequently missed and identifying these children and providing appropriate counseling can go a long way in ensuring regular follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.