
Abstract
Purpose:
Surgical management of a young patient with a stable but painful acromioclavicular (AC) joint but normal imagining is a challenging problem. A standard arthroscopic excision of distal clavicle seems too aggressive. An alternative procedure is arthroscopic debridement of the joint, particularly the often torn meniscus, and chondroplasty. This study demonstrates in younger patients the medium-term result of arthroscopic debridement of a painful AC joint.
Methods:
Fifty-three young adult patients with a stable but painful AC joint, and virtually normal magnetic resonance imaging (MRI) scan, had arthroscopic debridement of the AC joint. Follow-up was with questionnaire and American Shoulder and Elbow Surgeons Shoulder Score (ASES).
Results:
Mean age was 29 years (18–39), 41 male, 31 dominant arm. Twenty-two patients demonstrated additional shoulder pathology. Two patients had a later distal clavicle excision. Five patients had later surgery to other areas of the shoulder but had an asymptomatic AC joint. Thirty-eight patients completed the ASES questionnaire at mean 44 months (24–86) post-operation. The mean ASES score was 82.8 (52–100). There was no association between ASES score and AC joint disease severity found at operation (p = 0.25). Seven patients had ongoing shoulder symptoms, although none were severe enough to warrant any treatment.
Conclusion:
In this young group of patients with arthroscopic AC joint debridement, most had good relief of the AC joint related symptoms. This is a worthwhile procedure in the young patient, with quick recovery, and does not preclude further AC joint surgery later.
Introduction
Shoulder pain arising from the acromioclavicular (AC) joint is common. It is a diagnosis most commonly seen in older patients, related to AC joint degeneration and arthritic change. X-rays may reveal distal clavicular osteolysis or arthritis and magnetic resonance imaging (MRI) may show oedema of the distal clavicle. 1,2 Non-operative treatment can provide symptom relief in some patients. However, failing this, excision of the distal clavicle is the standard treatment via an open or arthroscopic approach.
AC joint pain is at times seen in younger patients, often with normal imaging studies and a stable joint. The management of these young patients who fail conservative treatment is controversial, as standard operative treatment with excision of the distal clavicle is difficult to justify. In these difficult patients, the senior author (SB) has described and performed arthroscopy of this small AC joint with debridement of the chondral surfaces and the meniscus. 3
This article aims to review the efficacy of AC joint arthroscopic surgery for treatment of AC joint pain and subsequent dysfunction in a group of young patients with no or minor imaging changes.
Material and methods
Ethics approval for this study was given by Monash University, Clayton, Australia.
Details of patients who had undergone the procedure of AC joint arthroscopy between 2002 and 2011 was prospectively recorded as a planned study and retrospectively analysed. The technique of AC joint arthroscopy has been published previously. 3 Adult patients under the age of 40 years at the time of surgery with a minimum of 2 years since the surgery were included. For those not contactable for medium-term follow-up, the most recent follow-up data are presented (Figure 1). Diagnosis of AC joint pathology was made on O’Brien 4 or Bell Van Riet 5 test and response to intra-articular local anaesthetic injection. Each patient had failed an intra-articular cortisone injection and a period, determined by the patient, of conservative management, predominantly resting the shoulder, before progressing to operation at a mean 14.20 weeks (range 5–58, SD 12.175). Normal X-ray and only minor change on MRI, such as a thickened capsule or small effusion, were prerequisites for inclusion. Exclusion criteria included instability of the AC joint, or on imaging an AC joint with an abnormal X-ray or with more than minor MRI change, in particular any oedema of the distal clavicle on an MRI was an exclusion.

CONSORT flow diagram.
Pre-operative demographic and clinical examination data included the history of AC joint symptoms and details of pre-operative physical examination. This included AC joint tenderness and positive O’Brien’s and/or Bell Van Riet tests. A prerequisite for inclusion was a reduction in pain with either the O’Brien or BVR test following an AC joint intra-articular local anaesthetic injection. Intra-operative notes and photographs were reviewed to characterize the pathological findings within the AC joint, as well as other glenohumeral pathology, such as the presence of internal impingement. 6 Short-term results of the operation, including those that were not available for longer term follow-up, and further management since this index procedure was also obtained from the patient medical records.
Overall intra-operative grading of the AC joint was completed in accordance with the following criteria: Grade 1 = chondral surfaces grade 1–2 and meniscus 1–2 Grade 2 = chondral surfaces grade 1–2 and meniscus 3 Grade 3 = chondral surfaces grade ≥2 and meniscus 4 Grade 4 = chondral surfaces grade ≥2 and meniscus 5
An attempt was made to contact all patients and invite them to participate in the post-operative follow-up study. This included completion of the validated shoulder scoring instrument, the American Shoulder and Elbow Surgeons Shoulder Score (ASES). 7 In addition, they were questioned as to occupation and lifestyle changes, ongoing symptoms and overall satisfaction.
Operative technique
Under general anaesthetic the patient is placed in the lateral decubitus position and secured using a suction mattress (Olympic Vac-Pac, Seattle WA, USA). The arm is placed in a traction system (Kaltec, Adelaide, Australia) and 15 pounds of longitudinal traction applied. The shoulder and arm of the affected limb are prepped and draped. As an initial step, a glenohumeral joint arthroscopy is routinely performed using the standard 4 mm arthroscope via a posterior portal. The subacromial space is then inspected using the same portal. Any pathology found in either area is treated at that stage in the appropriate manner.
The AC joint is then initially approached by a posterior portal using a 2.8 mm arthroscope (Dionics, Smith and Nephew Inc, Andover, MA, 01810, USA). The exact position of the AC joint is initially determined by placing a needle from a superior direction into the AC joint. The position of the posterior portal is then determined by a second, long, spinal needle. This is passed from posterior to anterior attempting to traverse the centre of the AC joint. The posterior portal is then made with a small stab incision. The trocar and cannula are then advanced through this posterior portal transversely across the AC joint and the anterior portal is established using a second stab incision over the tip of the emerging trocar and cannula. The trocar is removed, and the arthroscope partially inserted into the cannula. Debridement is undertaken using a 2.9 mm shaver (Dionics EP-1, Smith and Nephew Inc, Andover, MA, 01810, USA) with a full radius mini blade. The shaver tip is placed in the end of the cannula and advanced into the centre of the AC joint by gradually withdrawing the cannula and advancing the shaver.
Once within the joint the pathology is identified and documented. Any meniscal tearing is debrided, and the chondral surface is smoothed if necessary. If there is a complete tear in the meniscus, as is commonly present then both sides of the meniscus are readily viewed and debrided. The meniscus is debrided back to stable healthy appearing tissue. If the meniscus is intact, then following debridement of the first compartment an attempt to view the other side is made by reinserting the trocar. The larger portals are closed with 3/0 nylon and the stab portals with steri-strips.
Results
Data analysis was completed by a statistician using the ‘R’ package. 8
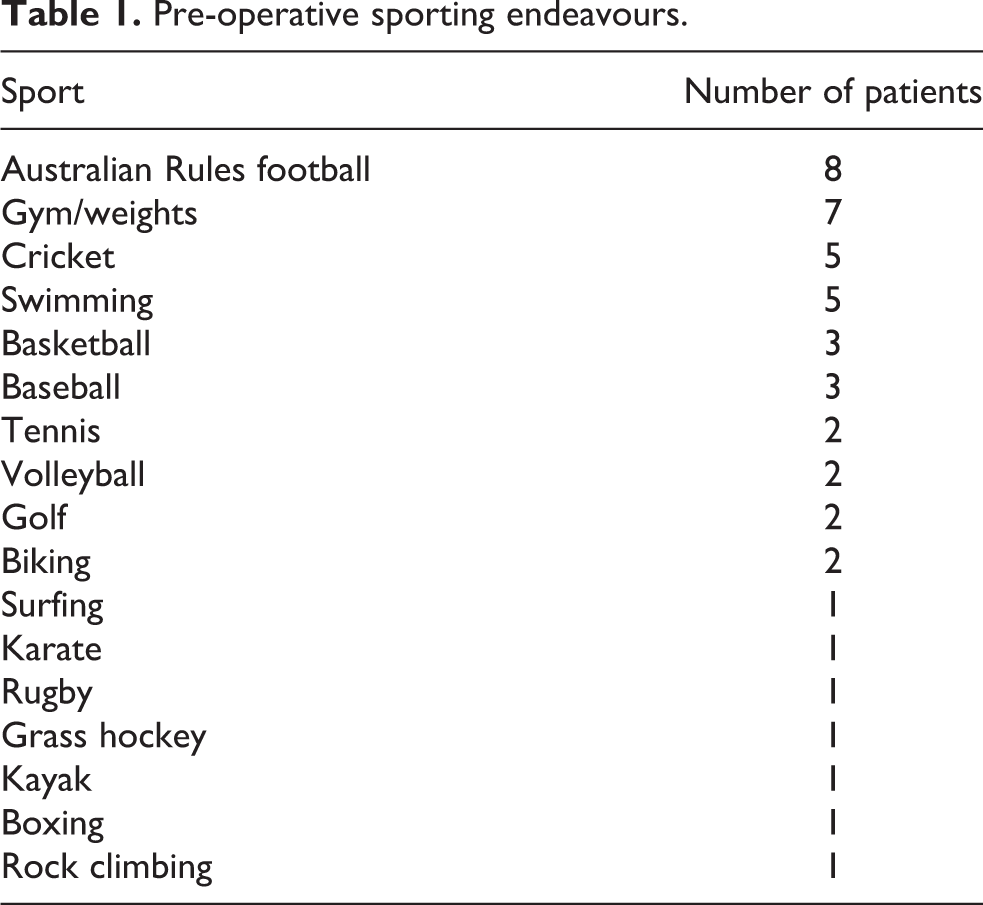
Fifty-three patients with a mean age of 27.8 years (range 18–39 years) at the time of operation underwent AC joint arthroscopy; 77.4% of patients were male (n = 41); 58.5% had an operation on their dominant side AC joint (n = 31). All patients reported their level of physical activity; 15.1% (n = 8) were elite athletes and 30.2% (n = 16) played sport at a local club level. They reported a variety of pre-operative sporting endeavours (Table 1). Pre-operatively, 18.8% of patients had minor AC joint changes on MRI, such as mild capsular swelling or a small effusion.
Pre-operative sporting endeavours.
Intra-operatively, there were 22 grade 1 joints, 18 grade 2, 9 grade 3 and 4 grade 4 joints. Generally, the clavicle side revealed greater chondral damage. Only two of these patients had bone on bone arthritis in the AC joint (Table 2).
Intra-operative findings.a

aChondral grade: 1 = normal or minor change, 2 = moderate change, 3 = area of subchondral bone; Meniscus grade: 1 = intact, 2 = intact with partial tear, 3 = small full thickness tear, 4 = large full thickness tear, 5 = absent
No significant association was seen between MRI and intra-operative disease grades (p = 0.16), even in the higher grades (p = 0.29).
Two patients failed treatment and went on to distal clavicle excision (DCE). The first had a normal MRI and a grade 4 joint at operation and underwent DCE 7 months later, with complete symptom resolution. The second had a normal MRI and grade 2 joint at operation and underwent DCE 14 months later. These two patients were excluded from further analysis.
Twenty-two patients either pre-operatively or intra-operatively were revealed to have some form of other shoulder pathology. This included mild subacromial impingement (n = 5), glenohumeral instability +/− previous stabilization (n = 8), labral fraying (n = 3), Superior Labrum Anterior Posterior (SLAP) tear (n = 2), Partial Articular-sided Supraspinatus Tendon Avulsion (PASTA) lesion (n = 1), rotator cuff pathology (n = 1). Seven patients had evidence of internal impingement and six had poor internal rotation range on pre-operative examination (<70°). There was no significant association between either poor internal rotation and disease severity (p = 0.09) or internal impingement and disease severity (p = 0.43).
Three went on to arthroscopic subacromial decompression, 10 to 24 months following the index procedure. Two patients went on to have glenohumeral stabilization procedures, 4 months and 1 year following the index procedure. At the time of surgery, the AC joint in these patients was asymptomatic. Three of these four patients completed the ASES questionnaire after the secondary procedure at a mean 77.7 months post-op (range 56–86 months).
The remaining 47 patients were invited to complete the ASES questionnaire and 35 of this other group of patients agreed. The mean time to questionnaire completion was a mean 43.5 months (range 24–86 months) post-operation. Thirteen patients were unable to be contacted to complete the ASES score. Of those total 38 patients who completed the questionnaire, there was a mean ASES score of 82.8 (range 57–100). There was no significant association between post-operative ASES score and disease severity at operation (p = 0.25). At telephone interview one patient reported he went on to win the world championship 100 m butterfly title 8 months following the procedure.
Only 10 of the 38 patients were available for formal clinical follow-up at a mean 43.5 months (range 24–70, SD 17.229). With a mean ASES score of 80.8 (range 56.7–96.7), they were considered to be a representative selection of the patient group. One patient in this group had positive O’Brien and Bell Van Riet tests and an ASES score of 63. The remaining nine had a normal AC joint examination, with negative AC joint compression tests. Those in this group with a poor ASES score had negative AC joint compression tests, indicating that their residual symptoms were related to other shoulder pathology.
The thirteen patients who were uncontactable for the medium-term follow-up study had a mean standard clinical follow-up of 3.3 months (range 0.5–9.5 months). At their last post-operative review 100% of patients were O’Brien or Bell Van Riet compression test negative.
Post-operative complications were minimal with one case of post-operative capsulitis which resolved without treatment.
Discussion
AC joint pain is at times seen in the younger population, often associated with sporting overuse. In the absence of MRI abnormalities, the pain would be due to inflammation which could be related to damage to the meniscus in the joint or the chondral surfaces.
Initial treatment is always conservative, however this at times fails. In these failed cases surgery needs to be considered. Traditional treatment has been excision of the distal clavicle, which however does produce some anterior-posterior instability of the distal clavicle. 9 In this young age group excision of the distal clavicle seems very aggressive and is difficult to justify. Direct debridement of the intra-articular structures with maintenance of the ligaments is an alternative. This treats the pathology which is causing the inflammation, and entirely maintains the stability of the joint, which is important in high level overhead athletes. This straightforward procedure, with rapid recovery, cannot lead to instability-related symptoms post-operatively. This technique has now been performed in 53 patients.
The patient group consisted of young patients with varied occupational and sporting habits.
MRI scans were normal for most patients, with only 10 patients demonstrating minor changes. On statistical analysis there was no significant association between the severity of AC joint MRI changes and the disease severity found at arthroscopy. This suggests that MRI may not be as sensitive as would be desired in detecting the degree of AC joint pathology.
At the time of operation 41.5% of patients had concomitant pathology, either known pre-operatively or diagnosed at arthroscopy. Although these conditions potentially could have contributed to shoulder pain it was felt clinically, in particular with a positive O’Brien or Bell Van Riet test pre-operatively, that the AC joint was the primary pathology causing pain in each case, and in all the symptom pain resolved, and the AC joint compression tests were negative, with a diagnostic AC joint local anaesthetic injection. An article by Brown reported the frequent association of arthroscopically diagnosed additional shoulder pathology in patients having excision of the distal clavicle for AC joint symptoms. They reported that in the less than 50-year-old group that 42% had a labral tear. 10 So, it was to be expected that in the group of patients in this study that additional pathology would be found in many at the arthroscopic examination.
The limitations of this study include the loss to follow-up of 13 patients, and the relatively small patient numbers limiting the significance of statistical analysis. However, as this is a very low morbidity procedure with a rapid recovery, it would appear that with only 2 patients requiring further AC joint surgery, and a mean ASES score of 82.8 for the remainder, that this simple procedure was successful in the large majority of patients in relieving the AC joint related pain. It is therefore a successful option to address AC joint pain, although perhaps only in the short term. We could not find any long term follow-up studies of the natural history of AC joint pain in a young population. This was a very active sporting population of athletes who were not in general prepared to undertake a long period of conservative management, nor give up their sport.
Progression of the AC joint disease in the long term is perhaps to be expected in these young patients with early degeneration. However, by avoiding bony excision in the short-term, sporting prowess should not be compromised, as it may be with distal clavicular excision, enabling the athletes to compete for a longer period. If finally, the AC joint arthritis pathology and symptoms progress to an unacceptable level, then excision of the distal clavicle is still able to be carried out, without compromise from the previous surgery.
Conclusion
The results of AC joint arthroscopy with debridement of the joint without excision of bone in a relatively young population are reported. It was successful in most in settling the AC joint related pain. Many patients however had other associated pathology which caused ongoing symptoms.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.