
Abstract
Background/objective:
Arthroscopic surgery in knee osteoarthritis is controversial with many studies refuting its efficacy in recent literature. This study aims to evaluate the mean duration to knee arthroplasty, and the effect of microfracture on the need for subsequent knee arthroplasty in patients above the age of 55 undergoing arthroscopic procedures for osteoarthritis.
Methods:
One hundred and nine consecutive patients with diagnosed osteoarthritis who underwent arthroscopic surgery performed from January 2000 to December 2012 on patients aged 55 years and above by a single surgeon were reviewed retrospectively. Demographic data, age at operation, comorbidities, perioperative details and information of subsequent total knee arthroplasty were collected and analysed.
Results:
There were 38 males and 71 females in our study group. The group was predominantly Chinese (51.38%), with hypertension and hyperlipidaemia being the most common comorbidities, each affecting 57.8% of our study cohort. All patients had a preoperative radiograph and a magnetic resonance imaging confirming the diagnosis of osteoarthritis associated with meniscal tears. Fifty-eight knees underwent microfracture along with arthroscopic meniscectomy. The mean follow-up duration was 127.5 months (10.5 years, range: 67–212 months). Twenty three patients (20.91%) underwent knee arthroplasties subsequently, with the mean duration to arthroplasty being 65.0 months (5.5 years, range: 7–166 months). The odds ratio of avoiding knee arthroplasty with microfracture was 1.03 (95% CI = 0.410–2.581).
Conclusion:
Arthroscopic procedures could possibly delay the need for subsequent knee arthroplasty for approximately 65 months in older patients with osteoarthritis. However, microfracture does not affect the duration between therapeutic arthroscopy and subsequent arthroplasty. Our long-term retrospective study provides an additional step in the understanding of the impact of arthroscopic procedures and a prospective case–control study would be an ideal follow-up to fully justify the application of arthroscopic procedures to delay knee arthroplasty.
Introduction
Osteoarthritis is a leading cause of disability, affecting more than 250 million people worldwide. 1 Radiographically confirmed symptomatic osteoarthritis affects more than nine million people in the United States alone. 2 In China, the prevalence of knee osteoarthritis was 14% in males and 27% in females aged between 55 and 59. 3,4 In Japan, prevalence of symptomatic osteoarthritis was 23% in males and 38% in females. 3,5 The incidence of osteoarthritis is expected to increase with age, and in Singapore it is estimated that the proportion of population aged 65 years and above will increase by 316% from 2008 to 2040. 3 Degenerate meniscal tears are common in patients with osteoarthritis of the knee with a considerable proportion being asymptomatic. This poses a diagnostic challenge to clinicians to determine whether presenting symptoms are caused by the meniscal tear, osteoarthritis, or both. 2
Nonetheless, when medical therapy fails to relieve pain from osteoarthritis, arthroscopic lavage, debridement and partial meniscectomy have been known to be options for patients with mechanical symptoms. 6 More than 90% of patients with symptomatic osteoarthritis have meniscal tears identified on magnetic resonance imaging (MRI). 7 With arthroscopic meniscectomy being the most common orthopaedic procedure performed in the United States 8 costing nearly US$5000 each, 6 many studies have been conducted to evaluate the effectiveness of this procedure. While there are studies suggesting the benefits of arthroscopic debridement and meniscectomy in patients who have osteoarthritis, 9 –12 several studies have refuted its efficacy in recent literature. Patients who underwent arthroscopic meniscectomy did not show a significant difference in patient reported outcomes compared to those who underwent physical therapy alone. 2,13 Moseley et al. showed no significant differences when comparing outcomes between arthroscopic debridement or lavage and sham surgery. 6 A recent meta-analysis performed by Brignardello-Petersen et al. showed that the benefits of arthroscopic debridement or partial meniscectomy on health-related quality of life was minimal. 14 Furthermore, there was a suggestion that there was a higher risk of arthroplasty with previous arthroscopic surgery. 14 Patients with osteoarthritic symptoms generally consent to undergo arthroscopic procedures with hopes of avoiding arthroplasty. In studies evaluating the effectiveness of arthroscopic procedures in patients with osteoarthritis, subsequent knee arthroplasties are regarded as failure of these procedures. 9 Most of these studies have been performed on Western populations.
With paucity of data in the Asian context, this study aims to evaluate the mean duration to knee arthroplasty and the effect of microfracture on the need for subsequent knee arthroplasty in patients above the age of 55 undergoing arthroscopic procedures for osteoarthritis.
Materials and methods
Design of study, setting and participants
We performed a retrospective, single surgeon study by reviewing consecutive knee arthroscopies performed from January 2000 to December 2012 by the senior author of this study at a tertiary teaching hospital. Our institutional review board waived approval for this study due to its retrospective nature and non-interaction with patients.
We included patients if they fulfilled the following inclusion criteria (1) aged 55 and above; (2) presented with clinical symptoms of knee osteoarthritis such as pain, swelling and mechanical symptoms of locking, catching and mechanical block to flexion or extension of the knee; (3) had radiographic evidence of at least Kellgren and Lawrence Grade III osteoarthritis; (4) had MRI findings of osteoarthritis and meniscal tear; (5) underwent a trial of conservative treatment which consisted of 2 weeks of oral non-steroidal anti-inflammatory drugs followed by an extra-articular pericapsular injection of a steroid (Triamcinolone) admixed with a local anaesthetic agent (Lidocaine 1%) and stretching exercises; (6) had residual joint line pain following conservative treatment and (7) underwent arthroscopic meniscectomy and/or debridement. For the purposes of this manuscript, debridement refers to the arthroscopic procedure of smoothening or trimming of frayed edges of either meniscus or cartilage. Patients with an intact meniscus found on arthroscopy were excluded.
Surgical techniques
All patients underwent general anaesthesia. Surgery was performed in supine position with a pneumatic tourniquet applied on the operated limb throughout surgery. Standard anteromedial and anterolateral arthroscopic portals were created. Diagnostic arthroscopy was then performed with evaluation of the patellofemoral joint, medial and lateral parapatellar gutters, intercondylar notch, medial and lateral tibiofemoral joint compartments. A 3.5 mm full radius shaver was then used for debridement of unstable chondral flaps. The menisci were then probed to look for any unstable flaps. Partial meniscectomy was performed if there was a component of the meniscal tear that interposed into the weight-bearing portion of the tibiofemoral joint. Partial meniscectomy was performed either by an arthroscopic shaver, arthroscopic scissors or an arthroscopic punch or a combination of the above instruments. Indication for microfracture in our patients was for decompression of the subchondral bone in an attempt to treat symptoms of pain rather than as a cartilage restorative procedure. Microfracture, if performed, was done after all necessary arthroscopic procedures so that the marrow elements are not diluted by the arthroscopy fluid. All patients were operated by the same surgeon using similar technique. The procedure was performed wither as a day surgery or patients were admitted to the hospital for one night. On the day of surgery, patients were kept for 6 h at the post-operative care unit for monitoring prior to discharge. Patients who were admitted were discharged the following day after being reviewed by the surgeon. All patients had standardised post-operative care and given appropriate oral and parenteral analgesia. Patients were allowed to ambulate on full weight-bearing status in the immediate post-operative period. Patients attended outpatient physiotherapy for muscle strengthening, proprioceptive training and gait training after surgery. They were then reviewed by the specialist at 2 weeks post-operatively for a clinical review of their symptoms and wound status. They were then continued on outpatient follow-up variably. Total knee arthroplasty (TKA) was offered as a surgical option to patients who had persistent clinical symptoms of osteoarthritis such as pain, swelling, mechanical symptoms of locking, catching and/or mechanical block to flexion or extension of the knee at a minimum of 6 months following arthroscopy.
Data handling and statistical analysis
Electronic health records and hardcopy medical records were queried. Data on patient’s gender, age at operation, comorbidities (diabetes, hypertension, hyperlipidaemia, gout and stroke), ethnicity and intraoperative data were collected. National electronic health records were screened to ascertain if the patient had undergone a TKA in any other public healthcare institution. Failure of arthroscopic meniscectomy and debridement was defined as the need for subsequent knee arthroplasty.
Data was collected on Microsoft Excel 2016 (Microsoft, Redmond, Washington, USA). Student’s t-test was used to compare the mean duration to arthroplasty and the mean age during procedure in the ‘Meniscectomy only’ group compared with ‘Meniscectomy and Microfracture’ group. Z-test was used to compare the proportion of patients of different gender, ethnicity and comorbidities between both groups, and the odds ratio of avoiding knee arthroplasty with microfracture was calculated. All statistical analyses were performed on IBM SPSS Statistics for Windows Version 22.0 (IBM Corp, Armonk, New York, USA).
Results
Thirty-eight patients were male and 71 patients were female (Table 1). Fifty six of them were Chinese, five were Malays, 35 were Indians, while 13 were of minor ethnicities in our population, comprising of Caucasian, Sri Lankan, Indonesian, Cambodian, Filipino and Sikh origin (Table 1). The most common comorbidities were hypertension and hyperlipidaemia, each afflicting 63 patients (57.80%) in our study population (Table 1). Diabetes mellitus affected 24.8% of our study population (Table 1), in keeping with national prevalence. Four patients had a past medical history of gout, while four patients had a cerebrovascular accident previously (Table 1). There were no differences in demographics between patients who had meniscectomy alone and those who had meniscectomy and microfracture (Table 2).
Demographics and comorbidities of patients in study population.

Comparative demographics and comorbidities of patients who underwent ‘meniscectomy alone’ and patients who underwent ‘meniscectomy and microfracture’.

a Student’s t-test was used to compare the mean age during procedure between ‘meniscectomy alone’ and ‘meniscectomy with microfracture’ groups.
b Z-test was performed to compare the proportion of patients of different gender, ethnicity and comorbidities between ‘meniscectomy alone’ and ‘meniscectomy with microfracture’ groups.
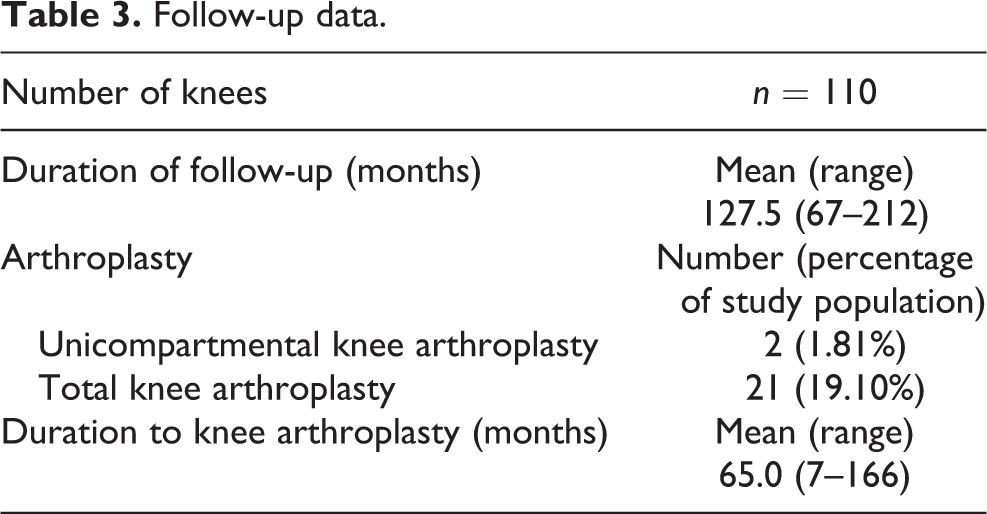
The mean follow-up for our patients was 127.5 months (10.6 years), with the shortest follow-up duration being 67 months. Twenty-three patients (20.91%) underwent knee arthroplasties subsequently, with the mean duration to arthroplasty being 65 months (range: 7–166 months; Table 3). Microfracture was performed concurrently in 58 knee arthroscopies (52.73%). There was no difference in the mean duration to arthroplasty in the meniscectomy only group compared with meniscectomy and microfracture group (63 months vs. 65 months; p = 0.665). The odds ratio of avoiding knee arthroplasty with microfracture was 1.03 (95% CI = 0.410–2.581; Table 4) and is therefore not significant.
Follow-up data.
Microfracture and the need for subsequent arthroplasty.

Discussion
The controversy over the role of arthroscopic surgery in patients with osteoarthritis has generated much interest in the Orthopaedic community. There is a concern that arthroscopic surgery in these patients would lead to an accelerated progression of osteoarthritis. 15 There is also evidence to suggest that patients with advanced osteoarthritis are unlikely to benefit from knee arthroscopy. 16 With a lack of literature on Asian patients, we aimed to evaluate the mean duration to knee arthroplasty and the effect of microfracture on the need for subsequent knee arthroplasty in patients above the age of 55 undergoing arthroscopic procedures for osteoarthritis. We hope that this will provide a knowledge base for future prospective studies.
The mean age at arthroplasty for our study was 64 years (range: 55–76 years). A study by Brophy et al. showed that patients who underwent knee surgery had TKA at a significantly younger age of 59 years compared to 67 years in those who did not. 17 In their study, they also reported that the age at the time of arthroscopy was associated with a higher odds of subsequent arthroplasty. In a study by Winter et al., patients with a mean age of less than 65 had a yearly incidence of knee arthroplasty of 1.87% compared to 5.13% in those with a mean age of more than 65. 15 In our study, the mean age at which patients underwent arthroscopic surgery was 60 years. This could explain the slightly older age at which subsequent arthroplasty was performed. Furthermore, the mean age of 64 at time of arthroplasty seems to be consistent in the country of origin of this study as seen in a study by Thambiah et al. 18
In our study, older patients with end-stage osteoarthritis who would be by current opinion considered poor candidates for arthroscopic surgery, had a mean survivorship of 65 months, or approximately 5.5 years prior to undergoing TKA. Comparatively, the mean duration to knee arthroplasty following arthroscopy reported in a meta-analysis of 20 studies was 3.4 years. 15 In another study which closely resembles our patient population in terms of severity of knee osteoarthritis, the mean duration to knee arthroplasty was 4.4 years. 19 The patients in our study had a better mean survivorship following arthroscopic surgery compared to that reported in Western studies. Five and half years would be considered a significant amount of time till knee arthroplasty, which in itself has a limited lifespan. The authors believe that in patients who are refractory to maximum medical therapy and those who are too young for knee arthroplasty, arthroscopic surgery could be an effective and viable option, provided the indications are correct.
After the introduction of MRI in clinical practice, bone marrow lesions (BMLs) have emerged as a central component of many different inflammatory and non-inflammatory disease affecting the musculoskeletal system including the knee joint. The presence of BMLs in osteoarthritis has been related to mechanical loading and increased subchondral stress and has been shown to be associated with progression of disease, cartilage loss and subsequent risk of TKA in most studies. 20 –22 The earliest hypotheses pertaining to BML formation focused on reduced microcirculation, leading to ischaemia and increased intraosseous pressure. 23 On the basis of this hypothesis, the senior author of this study used microfracture in the area of the BML formation to relieve pressure in an attempt to alleviate pain rather than a cartilage restoration technique. Microfracture has been shown to provide clinical benefit in the osteoarthritic knee. 24 It is a relatively simple procedure that can be done concurrently with other arthroscopic procedures and requires minimal equipment. Given the fact that microfracture was undertaken more for symptom relief rather than for cartilage restoration, it comes as no surprise that we found the odds ratio of avoiding knee arthroplasty with microfracture was 1.03 (95% CI = 0.410–2.581). Indeed, concerns have been raised regarding the efficacy of microfracture in delaying osteoarthritis and preventing further surgery. 25 This is consistent with our study findings, where patients with microfracture are as likely to undergo subsequent knee arthroplasty compared to those without.
Complications associated with arthroscopy are minimal. In a systematic review done by Brignardello-Petersen et al., the risk of mortality and nerve injury is close to zero, while the risk of infection and venous thromboembolism is two and five for every 1000 patients, respectively. 14 With low rates of complications and its effectiveness in delaying or even preventing the need of knee arthroplasty, arthroscopic surgery presents itself as a viable surgical alternative in patients with degenerative osteoarthritis with or without meniscal tears. In our series of patients, no complications were reported or documented following arthroscopic surgery.
This is a single surgeon, single centre study with standardised preoperative, operative and post-operative procedures for all patients. This will reduce bias and inter-surgeon or inter-centre variability, thus improving the consistency of our results. This is also a long-term study with a mean follow-up duration of 127.5 months (10.5 years), providing insight on the long-term outcomes of patients post arthroscopic meniscectomy. However, the strengths of the study must be interpreted in light of its weaknesses as well. This is a retrospective study with inherent bias and effects of confounding. There was no control arm of patients with osteoarthritis not undergoing arthroscopic surgery. We also did not report functional outcome scores. Compared to other studies on the same topic, the number of patients in our study is small although post hoc analysis showed adequate power. Despite these weaknesses, we still believe that our findings provide valuable information for an Asian cohort for future prospective studies.
Conclusion
Arthroscopic procedures could possibly delay the need for subsequent knee arthroplasty for approximately 65 months in older patients with osteoarthritis. However, microfracture does not affect the duration between therapeutic arthroscopy and subsequent arthroplasty. Our long-term retrospective study provides an additional step in the understanding of the impact of arthroscopic procedures and the duration to subsequent arthroplasty. A prospective case–control study would be an ideal follow-up to fully justify the application of arthroscopic procedures to delay knee arthroplasty.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.