
Abstract
Purpose:
Reverse shoulder arthroplasty (RSA) improves pain and function with very good satisfaction. Concerns exist about some activities of daily living (ADLs) involving internal rotation. The purpose of this study was to report how patients with bilateral RSA perform various ADLs.
Methods:
Thirty-one primary bilateral RSA patients (average age 76 years; 21 women and 10 men) completed a survey to assess various outcomes. The average time between the second arthroplasty and the survey was 2.7 years (range 1.0–7.8 years).
Results:
All clinical parameters were favorable. All patients reported being able to easily manage toileting and 87% reaching their back pocket. However, 29% found difficulty and 39% were unable to wash their back or put on bra. In comparison with various unilateral arthroplasty types, there was no statistical difference in overall activities (p < 0.05).
Conclusion:
Bilateral RSA can provide good functional outcome and high satisfaction. Patients manage most ADLs easily with some limitations in activities requiring extreme internal rotation.
Introduction
Reverse shoulder arthroplasty (RSA) has demonstrated reliable pain relief, good function, and high patient satisfaction in patients with cuff tear arthropathy (CTA). 1 –5 These patients have had poor results when treated with total shoulder arthroplasty (TSA). 6 RSA has also shown superiority in pain and function compared to hemiarthroplasty (HA) for CTA. 7 Indications for an RSA have expanded over the years. RSA has demonstrated good outcomes in several other indications including irreparable massive rotator cuff tear with pseudoparesis, rheumatoid arthritis with rotator cuff deficiency, previous shoulder resection with the absence of rotator cuff tendons, fracture sequelae, failed fracture fixation, failed previous shoulder arthroplasty, and irreparable three- and four-part proximal humerus fracture in the elderly. 8 –11
As the number of RSA increases, 12 more patients may require bilateral RSA, particularly given the fact that there is a high prevalence for bilateral rotator cuff disease in patients over 60 years of age and these tears progress over time. 13 –15 This means a number of patients with CTA are at risk for contralateral involvement which may ultimately progress to symptomatic arthritis. 15 In addition, TSA has been shown to have a 16.8% rate of eventual rotator cuff failure with increasing incidence of failure with time with revision to RSA. 16 Despite good outcomes for many indications, active internal and external rotation may not reliably improve after RSA. 4,5,17 Because suboptimal shoulder rotation may adversely affect many activities of daily living (ADLs), 18,19 surgeons may be opposed to performing bilateral RSA. Also, the increased constraint of the reverse arthroplasty design may lead surgeons to recommend low-to-medium demand activities to avoid subsequent implant loosening or mechanical complications.
There are three studies reporting the outcomes of staged bilateral RSA. 20 –22 Two of them have reported the effects of bilateral RSA on some ADLs. 20,22 The principal conclusion is that patients with bilateral RSA are able to perform some of the most important ADLs requiring rotation. 20,22 However, these studies have only included eight specific activities. Difficulty with ADLs especially those requiring a large amount of internal rotation, such as in toileting, washing behind one’s back, and placing a bra, are a concern as is the overall intensity of the activity level.
The purpose of this study was to specifically report how patients with bilateral RSA perform on the important ADL and the patient’s relevant low-, medium-, and high-demand activities.
Materials and methods
Following Institutional Review Board approval, the Mayo Clinic Joint Registry was used to identify 62 patients who underwent bilateral RSA performed from 2005 to 2012 with a minimum 1-year follow-up as had been used in previously reported patient activities at our institution. 23,24 Thirty-one patients (21 female and 10 male) responded to the survey. The average age at the time of completed survey was 76 years (range 55–94 years). Of the 62 shoulders treated in these 31 patients, the diagnosis was CTA in 45 shoulders, osteoarthritis with rotator cuff deficiency in 13 shoulders, rheumatoid arthritis with rotator cuff deficiency in 2 shoulders, locked anterior dislocation with massive rotator cuff tear in 1 shoulder, and osteoarthritis with severe posterior subluxation in 1 shoulder.
The study methodology was identical to previously reported evaluation of patient-reported activities following TSA, HA, and unilateral RSA. 23,24 A survey questionnaire was designed to evaluate the current level of daily and athletic activity following shoulder replacement. 23 –25 The previously validated patient questionnaire, providing high levels of agreement with the surgeon’s assessment included closed-ended questions that require a participant to fill in a circle with respect to their operated shoulder. 25 The questionnaire includes a pain scale (1 = no pain and 10 = severe pain), current pain medication usage (none, over the counter, narcotic, or Means both over the counter and narcotic both), a diagrammatic representation of active range of motion (ROM; forward flexion in degrees, external rotation in degrees, and internal rotation scaled 1–8), and a 10-point strength scale (1 = normal strength and 10 = complete paralysis) for each shoulder. 25 Additionally, patients were asked about their level of satisfaction with their shoulders both before and after bilateral RSA. Patients were able to answer on a 0–10 scale that corresponded to poor, fair, good, very good, and excellent. American Shoulder and Elbow Surgeons (ASES) Form (ASES) 26 and Simple Shoulder Test (SST) 27 scores were also obtained from these data. The patients were also given a questionnaire with a choice of 70 activities that the patient could indicate participation in over the past year (sporting activities and hobbies). There was also a question about current occupation (full-time, part-time, disabled, unemployed, and retired) and type of work. 23,24 Questions were added regarding the ability or amount of difficulty for the patient to perform ADLs, which included activities requiring large amounts of internal rotation such as the ability to manage toileting and fastening bra.
Questionnaires were mailed to potential participants with a cover letter explaining the purpose of the study and a consent form to be returned with the completed questionnaire in a prestamped, addressed envelope. Recipients were given the option to decline participation in the survey by checking a box at the end of the cover letter and returning it, instead of the completed survey. To maximize the response rate, the survey was first sent, followed by a second mailing to nonresponders 1 month later. Telephone call reminders began 1 month after the second mailing to nonresponders. Telephone calls included five call attempts before a person would be considered a noncontact. This would include two daytime calls, two evening calls, and one weekend call. Surveys were then resent to those participants who were contacted on the telephone and had agreed to complete the survey, but who no longer had a copy.
Response data, including the numerical data and the respondents’ written comments, were collected for the study group. Activities were categorized subjectively by the authors into three groups depending on the imposed demand on the shoulder replacement: low-, medium-, and high-demand activities. A low-demand activity was defined as an activity that does not impose a repetitive stress on the shoulder, does not involve heavy lifting, and most shoulder movements are below shoulder height. A moderate-demand activity was defined as an activity with the potential for repetitive stress and may involve lifting moderate loads up to 20 lbs and occasional overhead activity. A high-demand activity involves activities with repetitive stress, potential for heavy loads (greater than 20 lbs), and regular movements overhead. Patients were, in turn, classified as low, medium, or high demand, depending on their response to their highest level of activity participation, be it a single higher activity or multiple higher levels of activities reported. The distribution of low-, medium-, and high-demand activities in the sample was compared to a historical cohort of patients undergoing unilateral RSA, TSA, and HA. 23,24
All operations were performed by one of four surgeons (RHC, JWS, JSS, and one nonauthor). Operative reports were reviewed. The implants employed in the present study included 24 Delta Xtend (DePuy, Warsaw, IN, USA), 4 Aequalis (Tornier, Minneapolis, MN, USA), 31 Comprehensive reverse (Biomet, Warsaw, IN, USA), and 3 Encore (DJO surgical, Austin, TX, USA). Glenosphere sizes, humeral version, and subscapularis repair were recorded for all of the 31 respondents. After reverse arthroplasty, all patients underwent a similar postoperative rehabilitation program according to the Mayo Clinic protocol. Shoulders were supported in a sling or shoulder immobilizer for a minimum of 6 weeks postoperatively. During that time, passive ROM was allowed including internal rotation to the abdomen, elevation to 120°, and external rotation to either neutral to 20° based on surgeon preference. In some cases, such as a revision procedure, patient therapy was delayed until 6 weeks. At 6 weeks, an active-assisted program was started for all patients, allowing movement in internal rotation to behind the back, external rotation to 30°, and elevation to 150°, as was isometric strengthening. At 3 months, lightweights (<10 lbs) could be used. Following recovery from surgery (at 4–6 months), patients were allowed to perform “higher” level of activity but advised to avoid more than occasionally heavier lifting (>25 lbs) and to avoid activities with forceful impact.
Statistical analysis was performed using SAS version 8.2 (SAS Institute, Cary, NC, USA) by the Division of Biostatistics. Descriptive statistics were used to summarize all data. Intragroup comparisons for age group (patients < vs. ≥ 80 years of age), sex (males vs. females), hand dominance, first operation versus second, and indication for surgery (CTA vs. other indications) were made for the clinical and functional outcomes (ASES, SST, pain, ROM, and strength) using an unpaired t-test. This test was also employed to compare the ROM and strength between the first and second RSA. The χ 2 test was used to compare the distribution of level of activity between the bilateral RSA patients and the historical cohort of patients undergoing unilateral RSA. A correlation analysis was conducted between age, humeral retroversion, and glenosphere size with ROM and strength using a Spearman’s test. The α level was set at 0.05. Inferential statistics was conducted using JMP statistical software version 10.0 (SAS institute).
Results
Of the 31 respondents, 21 were retired, 2 worked full-time, 4 worked part-time, 3 were unemployed, and 1 did not respond to this question. The average follow-up from the first RSA was 4.1 years (range 1.8–8.8 years). The average follow-up from the second RSA was 2.7 years (range 1–7.8). A summary of the self-reported clinical data is found in Table 1. Table 2 provides a summary of all patient-reported activities following bilateral RSA. The top three commonly reported activities in each group included cooking (74%), baking (68%), and driving (61%) for low demand, gardening (48%), lawn mowing (35%), and leaf raking (29%) for medium demand and snow shoveling (32%), wheelbarrow (23%), and shoveling dirt (23%) for high demand. No patients described themselves as being permanently or temporarily disabled because of their shoulders.
Postoperative clinical data (self-reported).

ASES: American Shoulder and Elbow Surgeons; SST: simple shoulder test; RUE: right upper extremity; LUE: left upper extremity.
a Pain (1 = No pain; 10 = Severe pain).
b Active internal rotation (1 = level of greater trochanter; 2 = midbuttock; 3 = sacrum; 4 = L5; 5 = L1; 6 = T10; 7 = T6; 8 = T4).
c Strength (1 = normal; 3 = good; 5 = fair; 7 = poor; 10 = complete paralysis).
Patient-reported activities.a
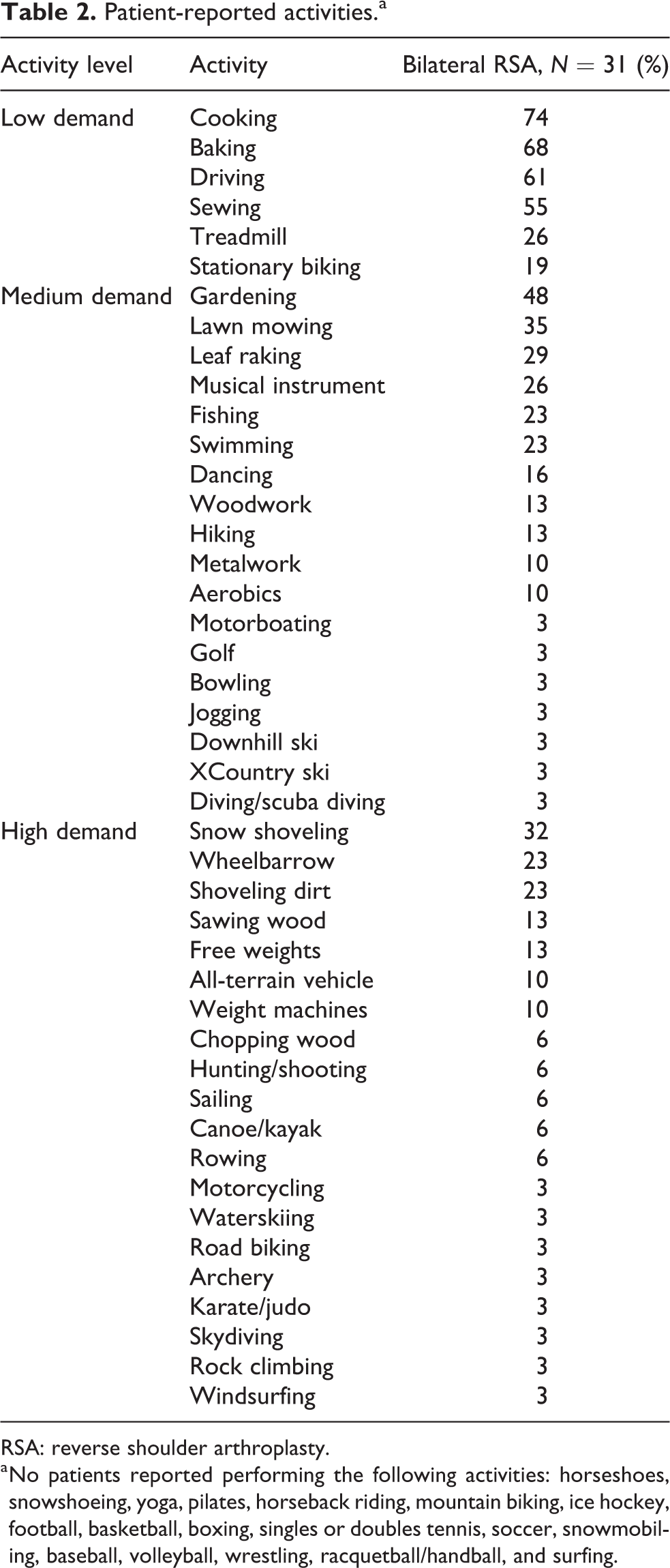
RSA: reverse shoulder arthroplasty.
a No patients reported performing the following activities: horseshoes, snowshoeing, yoga, pilates, horseback riding, mountain biking, ice hockey, football, basketball, boxing, singles or doubles tennis, soccer, snowmobiling, baseball, volleyball, wrestling, racquetball/handball, and surfing.
ASES scores averaged 78.6 (range 30–100) and SST scores averaged 7.6 (range 2–12). Of the 31 responses, patients rated their overall shoulder pain at an average of 1.4 on a scale of 0–10 with 0 = no pain and 10 = severe pain. Of the 31 patients, 8 patients (25%) reported taking medication for their pain, and of those, 3 patients (10%) required narcotic medication for the pain. Average level of satisfaction responses was poor (1.5) before surgery and very good (7.7) after surgery. Of particular interest is how people described their ability to perform tasks related to internal rotation of the upper extremity. The additional questions in the style of the SST are summarized in Table 3, with all patients being able to lift their arm to shoulder level, although this decreased to 28% if lifting 8 lbs with arm straight was required. Difficulties with ADLs were asked in the format of functional questions of the ASES score, which are summarized in Table 4. In all, 84% of the responders reported no to some difficulty tucking in a shirt in back of the torso. Similarly, 87% reported no to some difficulty reaching their back pocket and 100% reported being able to manage toileting with no to some difficulty. However, when washing their back or putting a bra on, 29% found it very difficult and 39% stated that they were unable to perform these tasks.
Ability to perform activities.a
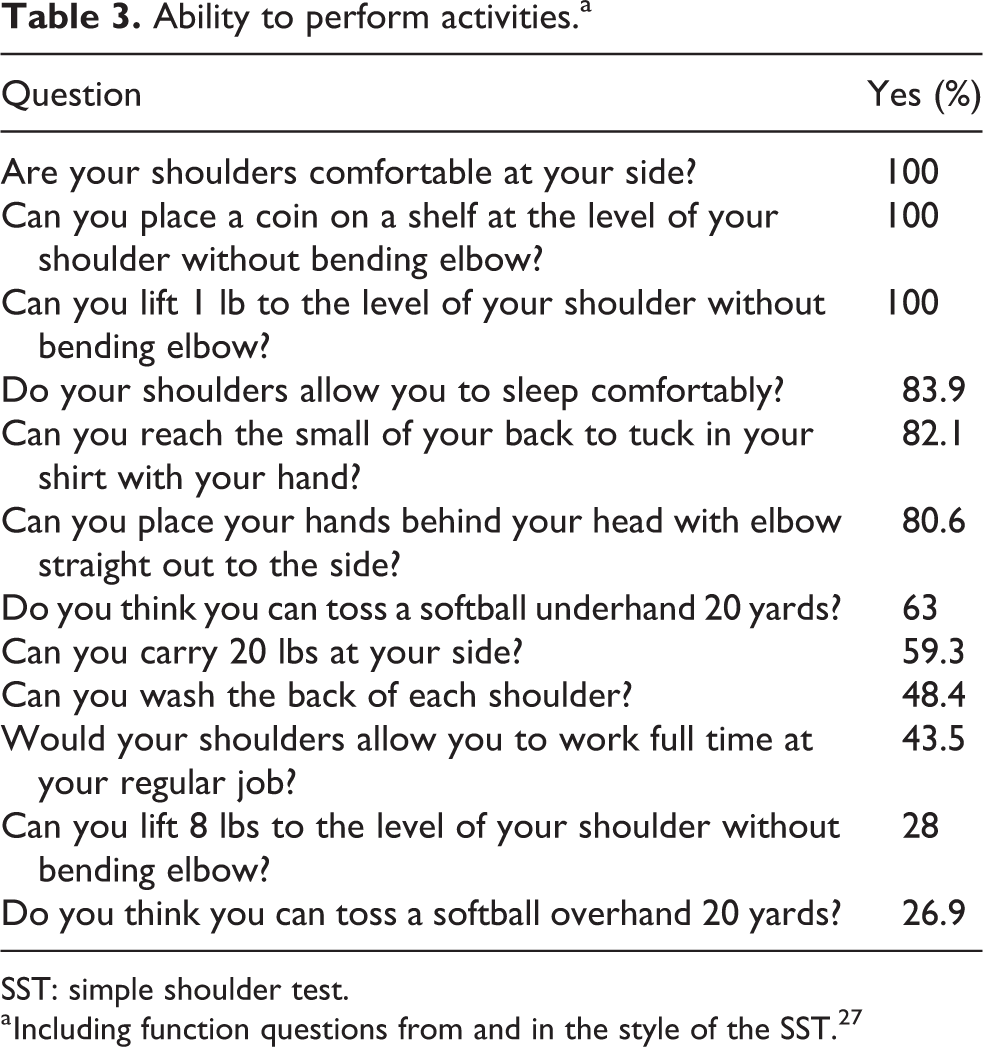
SST: simple shoulder test.
a Including function questions from and in the style of the SST. 27
Amount of difficulty with varying activities.a
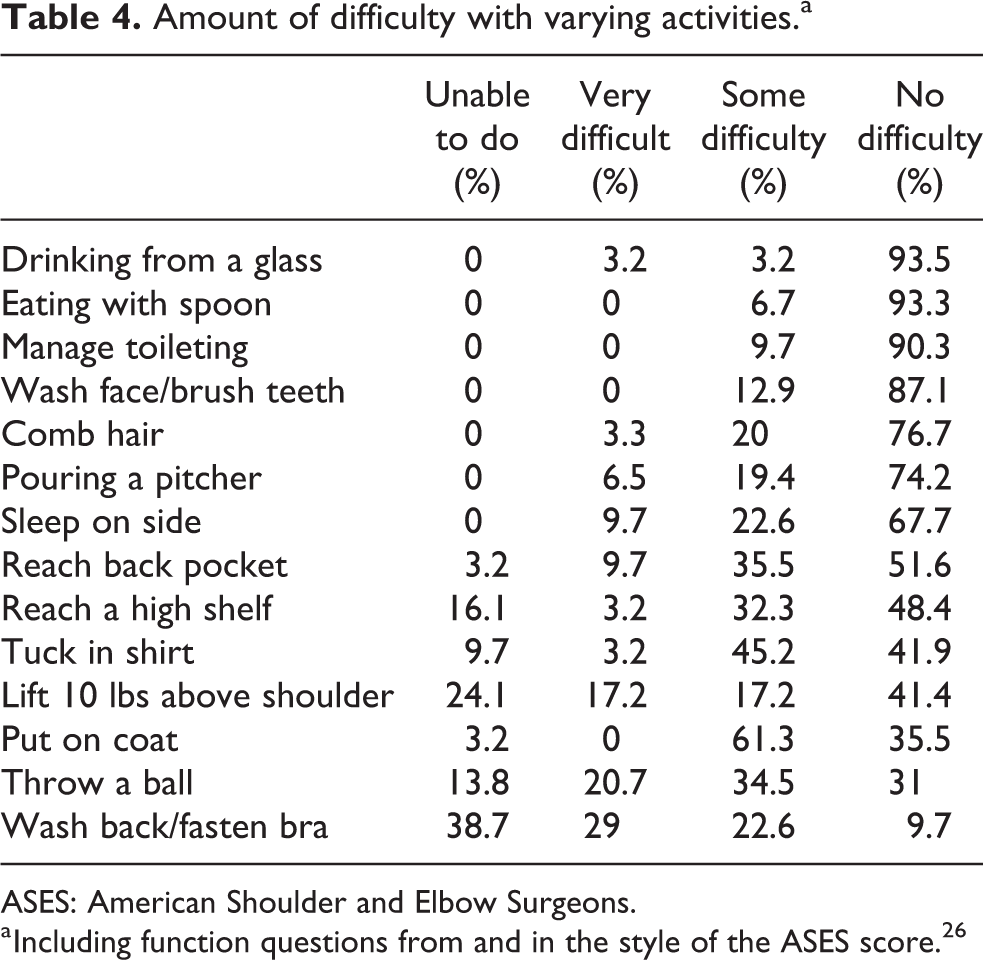
ASES: American Shoulder and Elbow Surgeons.
a Including function questions from and in the style of the ASES score. 26
A subgroup analysis was performed. With the numbers available, there were no significant differences for ASES score, SST score, pain, forward flexion, external rotation, internal rotation, and strength according to age subgroups (<80 years vs. ≥80 years), gender (males vs. females), hand dominance, first operation versus second, or indication for surgery (CTA vs. osteoarthritis with deficient rotator cuff, rheumatoid arthritis, or instability). Also, there were no significant differences between the first and second RSA for forward flexion, external rotation, internal rotation, and strength. With the numbers available, there were no significant correlations between age, humeral retroversion, subscapularis repair, and glenosphere size in relation to motion.
Our data were then compared with data from this institution in patient reported activities in unilateral RSA, TSA, and HA. 23,24 Table 5 summarizes and compares the distribution of patients’ overall activity level as low, medium, or high demand based on the highest reported level of activity for each patient. Similar distribution was seen in demand levels in bilateral RSA compared to unilateral RSA and TSA. There was no statistical difference in the activity level between those patients with bilateral and those with unilateral RSAs (p = 0.95).
Highest reported activity level and comparison with previous studies.

BRSA: bilateral reverse shoulder arthroplasty; RSA: reverse shoulder arthroplasty; TSA: total shoulder arthroplasty; HA: hemiarthroplasty.
a Patients were placed into low, medium, or high demand based on their highest reported level of activity.
Discussion
The principal finding of this study was that from our responses that patients undergoing bilateral RSA were able to be active and perform basic ADLs at an average of 2.7 years after their second surgery. The most common activities were cooking, baking, and driving for the low-demand group, gardening, lawn mowing, and leaf raking for the medium-demand group and snow shoveling, wheelbarrow, and shoveling dirt for the high-demand group. These activities are comparable to those reported after unilateral RSA, TSA, and HA. 23,24 RSA has generally been used for low-demand patients over 70 years of age but is accepted in younger patients if appropriately indicated. This is likely due to the expansion of the indications for RSA, the improvements in the implants, and the optimization of results. This results in the need for optimizing implant survival but also to be able to offer patients a surgical solution that will not preclude them from keeping active. The average age in this study was 76 years, but five patients were younger, with the youngest being 55. Outside of expert opinion articles, 28 it is not known which activities are possibly detrimental to the longevity of the implant. Our article shows that 55% of patients were able to return to high-demand activity, but we do not know what effect this will have long term, and survival data in the future may help determine appropriate activities. Due to the complex nature of failed RSA treatment, surgeons may be hesitant to allow their patients to return to a higher level of activity.
This study is the largest reviewed series to date of patients who have undergone bilateral RSA. The overall results in the present study are comparable to those in previous reports in terms of clinical outcomes, functional outcomes, and patient’s satisfaction. 20 –22 However, there are some differences between this study and those published by other authors. Our study included all diagnoses outside of revision surgery. Wiater et al. also included patients outside of CTA, 21 while the other two studies were limited to CTA diagnosis only. 20,22 The ROM in the present study was obtained as self-reported by patients, whereas in previous research ROM was clinically obtained. 20 –22 Thus, the mean forward elevation seen in the present study of 163° as opposed to the previously reported (from 120° to 144°) may be explained by differences in the assessment methods and may not be comparable. However, self-reported outcomes have been shown to have good patient–physician agreement. 25 Finally, although in the present study there were no differences in the outcomes between the first and the second RSA, improved results in the first compared to the second have been previously reported. 21,22 This was not seen in our study as well as no difference in repair of subscapularis or glenospere size. Four months was the closest interval between replacements with most occurring within the first year after the first RSA in our series of patients. Other studies have shown that 2- to 3-month intervals would be sufficient between surgeries. 20,22
With regard to ADLs after RSA, the majority of concerns are in activities that require the greatest amount of internal rotation. Patients with TSA on one side and RSA on the contralateral side demonstrate similar good satisfaction and forward elevation, but internal rotation averaged L1 for RSA and T8 for TSA. 29 This has led some physicians to avoid surgical treatment with bilateral RSA due to perceptions of unsatisfactory outcomes and dysfunction in ADL due to difficulty with internal rotation. 7,30 Patients may find difficulty rising from chair or seated position, especially wheelchair bound patients, as both abduction and internal rotation are required. The amount of internal rotation for perineal hygiene can be variable and dependent on the patient’s body habitus, such as height and weight, and may also be based on subjective measurements. While one study found improvements in internal rotation after RSA, 31 most studies have reported limited improvements in internal rotation. 20,21,32 Namdari et al. showed a maximum internal rotation of 102.2° needed to tuck in a shirt or unfasten a bra, but did not assess perineal hygiene in their study. 19 Raiss et al. found that genital hygiene requires a maximum internal rotation of 126° using three-dimensional motion analysis. 30 The biggest concern is for the patient to be able to perform personal hygiene with at least one extremity. All patients in our study were able to do this with no to only some difficulty. Similarly, Stevens et al. reported that all patients were able to perform hygiene; however, 3 of the 15 patients could only do this with one arm. 20 In another study, Morris et al. reported that 1 of 11 patients was unable to perform perineal hygiene and dress without assistance. 22 In this regard, Triplet et al. found that patients undergoing TSA were more likely to reach behind the back for washing and fastening bra compared to RSA but found no differences in managing toileting. 33 Outside of fastening bra and washing one’s back (38.7% unable to do and 29% found very difficult), internal rotation activities were able to be performed by most patients without any or only some difficulty. Overhead activities of lifting 10 lbs over the shoulder, reaching a high shelf and throwing a ball were the other activities that patients had difficulty with in our study.
Technical considerations during surgery may be able to improve internal rotation. Although we did not detect a difference in our study, subscapularis repair, humeral version, glenosphere sizing, and soft tissue tensioning may all effect the amount of achievable ROM. Internal rotation in TSA literature is partially related to healing of subscapularis. 34,35 Gerber et al. have described that not repairing subscapularis in his early experience with RSA led to inability of patient to reach behind their back as well as instability and anterior escape. 36 The overall version of the shoulder construct may be modified to better adapt to the patient’s condition in cases of bilateral RSA, sacrificing external rotation in favor of the ability to reach behind. Improvement in ADL with neutral humeral placement (instead of using 20° of retroversion) has been reported, 37 but this has not been studied in terms of increasing internal rotation. Use of a larger glenosphere sizes increases the amount of motion prior to bone-implant impingement allowing for a greater arc-of-motion. Finally, proper soft tissue tensioning may allow more motion. A tight component seating may decrease risk of instability but may forfeit motion, not allowing for internal rotation necessary for perineal care. Tight seating has been shown to increase tension on teres minor allowing for better external rotation function, 21 but this may forfeit internal rotation ability and further research in this area is needed. Under-tensioning also places the implant at increased instability risk, although the over-tensioned implant may cause acromial complications. The surgeon should strive to achieve a stable implant which can maximize its ability to achieve the desired motion.
There are several limitations related to the current study. First is the lack of preoperative scores and activity levels for comparison; however, the scope of this study was to evaluate patient-reported activities and followed methodology that had previously been used in previous questionnaire studies. 23,24 Second, this study was a survey with a 50% response rate; however, this is similar to rates found in previous questionnaire studies. 23,24 Therefore, there may be a possible selection bias and information may not be representative of all of the patients. As well, patients may have a recall bias; continued data collection at regularly scheduled follow-up visits may be more accurate to describe patient’s activities. Third, although this is the largest review of patients undergoing bilateral RSA to date, the sample is still relatively small, which may increase the risk of type-II error to detect significant differences in the outcomes. This may also be true in our subgroup analysis, which did not find any differences in subscapularis repair, hand dominance, glenosphere sizing as well. Fourth, the present study provided a mid-term follow-up; given the concerns regarding the longevity of these implants, a long-term follow-up would be important to correlate activity and survival. Finally, a final limitation is the lack of a control or comparative group with which to compare our patients to those of a similar demographic and age-matched cohort.
This study provides insight into expectations for the patient undergoing bilateral RSA. The surgeon can have more confidence that the patient will be able to perform toileting activities, although this concern should still be discussed in the counseling and consent process. The patient may be able to return to high-demand activities, but at this point we do not know the long-term effects of these activities on survival of the implant and this should also be discussed with the patient. This is of increasing concern as RSA becomes more frequently used in younger and more active patients. Future studies in this area will be beneficial.
Conclusions
The principal conclusion of this study is that patients undergoing bilateral RSA have good function and satisfaction, but also no to little difficulties in general activities and most ADL, including those requiring more internal rotation such as reaching the back or toileting. The surgeon may be less apprehensive of performing bilateral RSA due to concerns of limitations in essential hygiene activities. Patients are able to return to most activities, although long-term survival data still need to be examined to determine their effects.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.