
Abstract
Introduction:
Engaging Hill–Sachs lesions in recurrent anterior shoulder dislocation have been managed with the remplissage procedure. Clinical and cadaveric studies have reported limitation of rotation after this procedure. We introduce the reverse McLaughlin procedure where the infraspinatus and the underlying capsule are detached and approximated into the Hill–Sachs defect with transosseous sutures. This is a preliminary report using this technique.
Methods:
Seventeen patients with recurrent anterior shoulder dislocations and an engaging Hill–Sachs lesion underwent a Bankart repair and remplissage procedure (n = 9) or the reverse McLaughlin procedure (n = 8). Patients were evaluated using the SF-36, American Shoulder and Elbow Surgeons (ASES), and Constant scores. Clinical assessment of the shoulders was also performed.
Results:
At the final follow-up, all patients in both groups achieved comparable clinical outcome scores. No significant differences were reported in the range of motion of the shoulders between the two groups. There was one dislocation of the operated shoulder in each group after an injury.
Conclusion:
The reverse McLaughlin procedure for engaging Hill–Sachs lesions is simple, easy to perform, and associated with functional outcomes and range of motion at least equivalent to those obtained via the remplissage technique. It may be an alternative to the latter procedure.
Level of Evidence:
III, Retrospective Comparative Study
Keywords
Introduction
Engaging Hill–Sachs lesions are common injuries in recurrent anterior shoulder dislocations. The incidence of Hill–Sachs lesions in anterior shoulder instability has been approximated to be between 40% and 90%. 1,2 Indications for surgical repair of this defect is dependent on the extent of the defect as well as symptoms of instability. 3 Currently, such lesions are commonly treated surgically with the remplissage procedure, 4,5 with good outcomes being reported. 5 –8 However, many patients also experience limitation in external and internal rotation of the joint following this procedure. 6,9 –11 Garcia et al. reported that 66.5% of patients experienced a reduced range of motion in throwing after the remplissage procedure. 10 This limitation in shoulder range of motion has also been shown in cadaveric studies. 9 We postulate that the remplissage procedure that involves a tenodesis of the infraspinatus tendon and posterior capsule could result in postoperative stiffness leading to the reduction in internal and external rotation of the shoulder.
There is still controversy on the optimal treatment of Hill–Sachs lesions with several surgical techniques being described. This ranges from gleno-humeral capsular shift to surgically tightening the anterior capsule, 12 glenoid or humeral head bone augmentation, 13,14 resurfacing, 15 and prosthetic replacement. 13,16
The technique of filling the reverse Hill–Sachs defect with soft tissue has been well-documented and described for patients with significant lesions. The McLaughlin procedure was first described in 1952. 17 This procedure involves an open transfer of the subscapularis tendon to fill a reverse Hill–Sachs lesion on the humeral in patients with posterior shoulder dislocation with minimal restriction in the range of movement of the shoulder postoperatively. 18 –20 For Hill–Sachs lesion in anterior shoulder dislocation, arthroscopic remplissage procedure was performed, first described by Purchase et al. 4 This technique involves arthroscopic capsular and infraspinatus tenodesis into the Hill-Sachs lesion.
We modified the McLaughlin procedure for the treatment of engaging Hill–Sachs lesions in anterior shoulder dislocations. A segment of the infraspinatus and underlying capsule was elevated and reinserted into the posterior superior Hill–Sachs defect. This preliminary report was to review the clinical outcomes of the reverse McLaughlin procedure in patients with engaging Hill–Sachs lesion and to compare them with the outcomes after the conventional remplissage procedure.
Patients and methods
This is a single-institution retrospective study analyzing the clinical outcomes of a consecutive series of patients with anterior shoulder instability who underwent repairs of the anterior labral tear and the engaging Hill–Sachs lesions from 2012 to 2015. Patients selected were followed up for a minimum of 1 year from the date of surgery.
Patients in the study had undergone either the standard anterior labral repair with the remplissage procedure or the anterior labral repair with the reverse McLaughlin procedure for concurrent engaging Hill–Sachs lesions for anterior shoulder instability. Patients for whom postoperative clinical evaluation data were not available (i.e. lost to follow-up), those with a follow-up period of <12 months, and those with previous shoulder surgeries were excluded from the study. Seventeen patients fulfilled the inclusion criteria for the study. Eight had undergone an anterior labral repair with the reverse McLaughlin procedure and nine had undergone the labral repair with the remplissage procedure. All cases of arthroscopic remplissage procedure were performed by one surgeon (BHMT) who is experienced in arthroscopic remplissage procedure and all “reverse McLaughlin” procedures were performed by another senior surgeon who is experienced in performing the novel technique of “reverse McLaughlin” procedure (VPK) that he has described.
All patients had a history of two or more documented anterior dislocations of the shoulder. All had plain anteroposterior and axillary view of the joint. An MRI was performed in the patients before surgery to demonstrate the presence of a Hill–Sachs lesion besides the anterior labral tear. Note was also made of capsular laxity and the presence of a concomitant bony Bankart lesion. The latter group had further computed tomography assessment to document the size of the glenoid defect. Any defect of the glenoid excluded the patient from the study.
All patients had the surgery under general anesthesia in a beach-chair position. A standard posterior viewing portal was made (Figure 1). All intra-articular pathologies were documented. The shoulder was then abducted 100°, extended 10°, and maximally externally rotated. The presence of an engaging Hill–Sachs lesion was documented (Figure 2). The decision to proceed with an arthroscopic remplissage procedure or a mini open reverse McLaughlin procedure was decided by the preference of the individual surgeon. The standard anterior labral repair was carried out using standard portals. 2.9 mm polyether ether ketone (PEEK) knotless suture anchors (Arthrex PushLock™, Naples, Florida, USA) were used for repair of the Bankart lesion.

Posterior viewing portal (*) and an anterior working portal (+).

Visualization of Hill–Sachs lesion arthroscopically.
Reverse McLaughlin procedure
The Hill–Sachs lesion (Figure 3) was localized with the arthroscope and marked with percutaneous needles to delineate the anterior and posterior limits. A mini open lateral approach to the shoulder was performed, the incision being made between the localizing needles exiting the skin. Following a deltoid split, the infraspinatus tendon and underlying capsule were identified and elevated from the greater tuberosity by sharp dissection (Figure 4(a) and(b)). The extent of elevation was indicated by the localizing needles. The floor of the Hill–Sachs defect was curetted and the elevated segment of the cuff and capsule was advanced medially to fill the defect (Figure 5(a) and (b)). The cuff was approximated to the defect using transosseous sutures (Figure 5(b)). The deltoid split was loosely tagged and the skin closed in layers with absorbable sutures. The arthroscopic portals were also closed with absorbable sutures.

Hill–Sachs lesion (*) as shown in the saw bone model. The rotator cuff muscles and tendons have been deliberately left anatomically inaccurate to allow adequate visualization of the Hill–Sachs lesion.
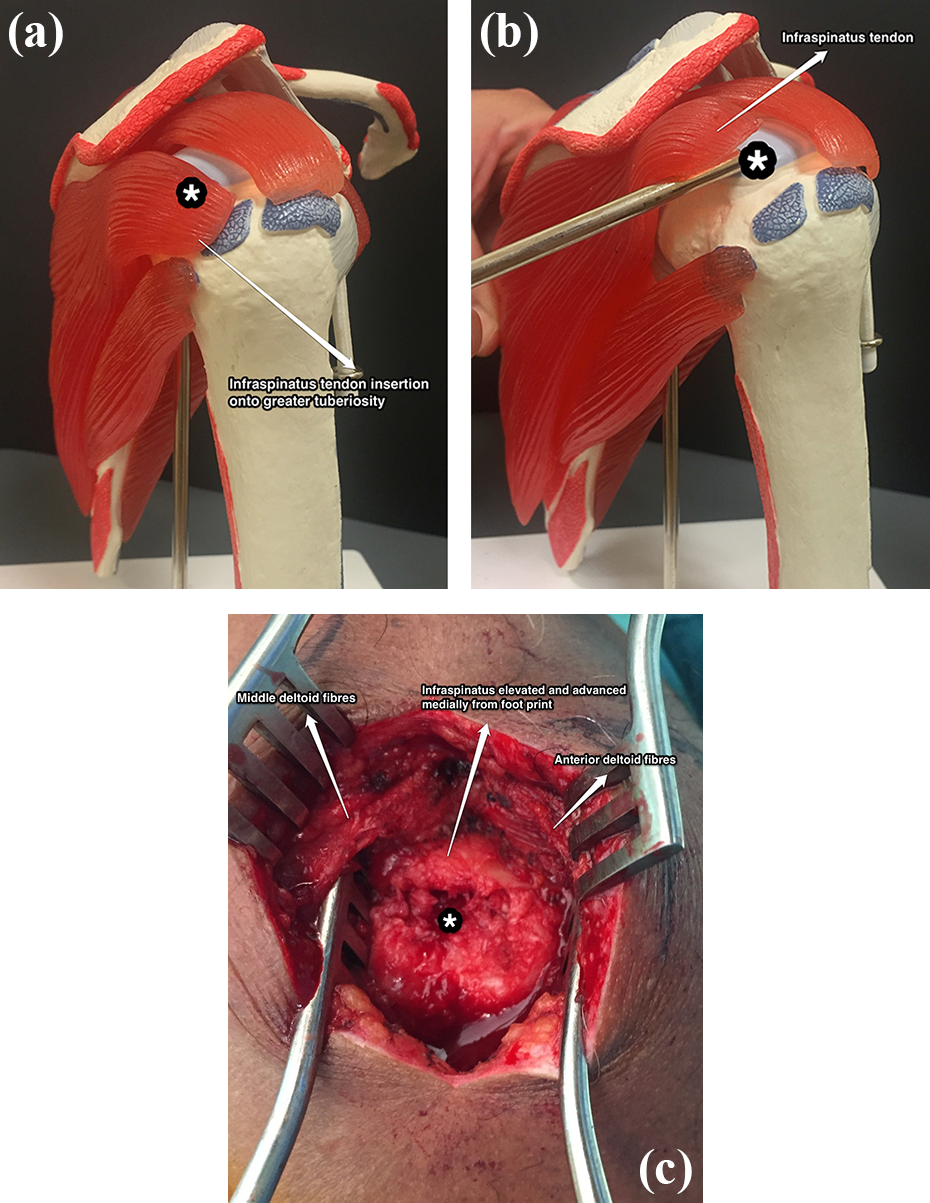
Before (a) and after (b) elevation of the infraspinatus tendon from the greater tuberosity in a saw bone model. Hill–Sachs lesion (*) with the overlying muscles and tendons as shown in the saw bone model. (c). Elevation and medialization of the infraspinatus tendon from the greater tuberosity. Decorticated Hill–Sachs lesion (*) with the overlying muscles and tendons as shown.

Advancement of the infraspinatus tendon insertion medially into the Hill–Sachs lesion (*) showing the completed “reverse McLaughlin” procedure in saw bone model (a) and patient (b).
Arthroscopic remplissage procedure
The arthroscopic Hill–Sachs remplissage was performed using a PASTA repair kit Depuy Mitek Healix Transtend Implant System with two double-loaded 3.4-mm anchors (Depuy Synthes, Warsaw, Indiana, USA), as described by our authors Tan and Kumar. 21 The standard arthroscopic portals were used for the anterior labral repair prior to the remplissage procedure. A slightly lateral and superior posterior portal was made as a Hill–Sachs remplissage procedure was anticipated. A 70° arthroscope was then placed through the anterior portal to view the Hill–Sachs lesion on the posterior aspect of the humeral head. The bed of the Hill–Sachs lesion was abraded with a curette. In the remplissage procedure, an additional accessory portal for insertion of the anchors was performed to ensure the anchors can be optimally placed in the superior and inferior extents of the Hill–Sachs lesion. Two anchors were inserted into the head at the margin of the Hill–Sachs lesion with intervening sleeve of infraspinatus tendon. The remplissage procedure was then achieved with the double pulley method using two double-loaded 3.4-mm suture anchors (Depuy Synthes). This method was then repeated with the second anchor. All incisions were closed with absorbable sutures.
Postoperative rehabilitation
Both patient groups underwent the same rehabilitation program postoperatively. The operated shoulder was immobilized in a universal arm sling for 3 weeks with cryotherapy to reduce pain and inflammation. Subsequent rehabilitation sessions focused on progressive shoulder range of motion and strengthening exercises and optimization of shoulder function to allow return to work and sports over a course of 16 weeks.
Evaluation of outcomes
All patients had a minimum follow-up period of 12 months postoperatively. The research coordinator who was blinded to the surgical management and who was not involved in any of the surgeries carried out the clinical evaluation preoperatively and at 3 months, 6 months, 1 year, and 2 year. The clinical assessments consisted of the American Shoulder and Elbow Surgeons (ASES) scores, Constant score, and SF-36. In addition to the range of motion measurements included in the Constant score, external rotation of the shoulder with the arm at the side was evaluated and assessed using a goniometer.
Statistical analysis
Continuous variables are reported as means. Categorical variables are reported as absolute values and percentages. Subsequent analysis was performed using t-tests for continuous variables (IBM SPSS Statistics version 20). The paired t-test was used to compare preoperative and postoperative scores. The value of p < 0.05 was defined as statistically significant.
This study was approved by the National Disease Specific Review Board.
Results
The demographics of our patient cohort are illustrated in Table 1.
Demographics of the patient cohort.

A total of 17 patients were included in the study, of whom eight patients had undergone the reverse McLaughlin procedure and nine patients had undergone the standard remplissage procedure. Seven of the eight patients were males in the reverse McLaughlin group, and all the patients were males in the remplissage group. There were no other differences in the patient demographics between the two groups: age, gender, handedness, side affected, and dominance of the operated limb.
The mean age at the time of surgery was 25.6 (range 18–67) years. The final evaluation was performed at an average of 16.8 (range 12–34) months postoperatively. The dominant upper limb was injured in six of the eight (75%) patients in the reverse McLaughlin group and six of the nine (67%) in the remplissage group. None of the patients had any neurological or vascular deficits at the time of initial assessment.
There was no significant difference in the mean time taken for the procedure in the two groups. The mean time for the Bankart repair with the reverse McLaughlin procedure was 104 (range 87–123) min and 91 (range 75–107) min for the Bankart repair with the remplissage procedure (p = 0.056).
Outcome scores
The results of the outcomes scores at follow-up are summarized in Figures 6 to 9.
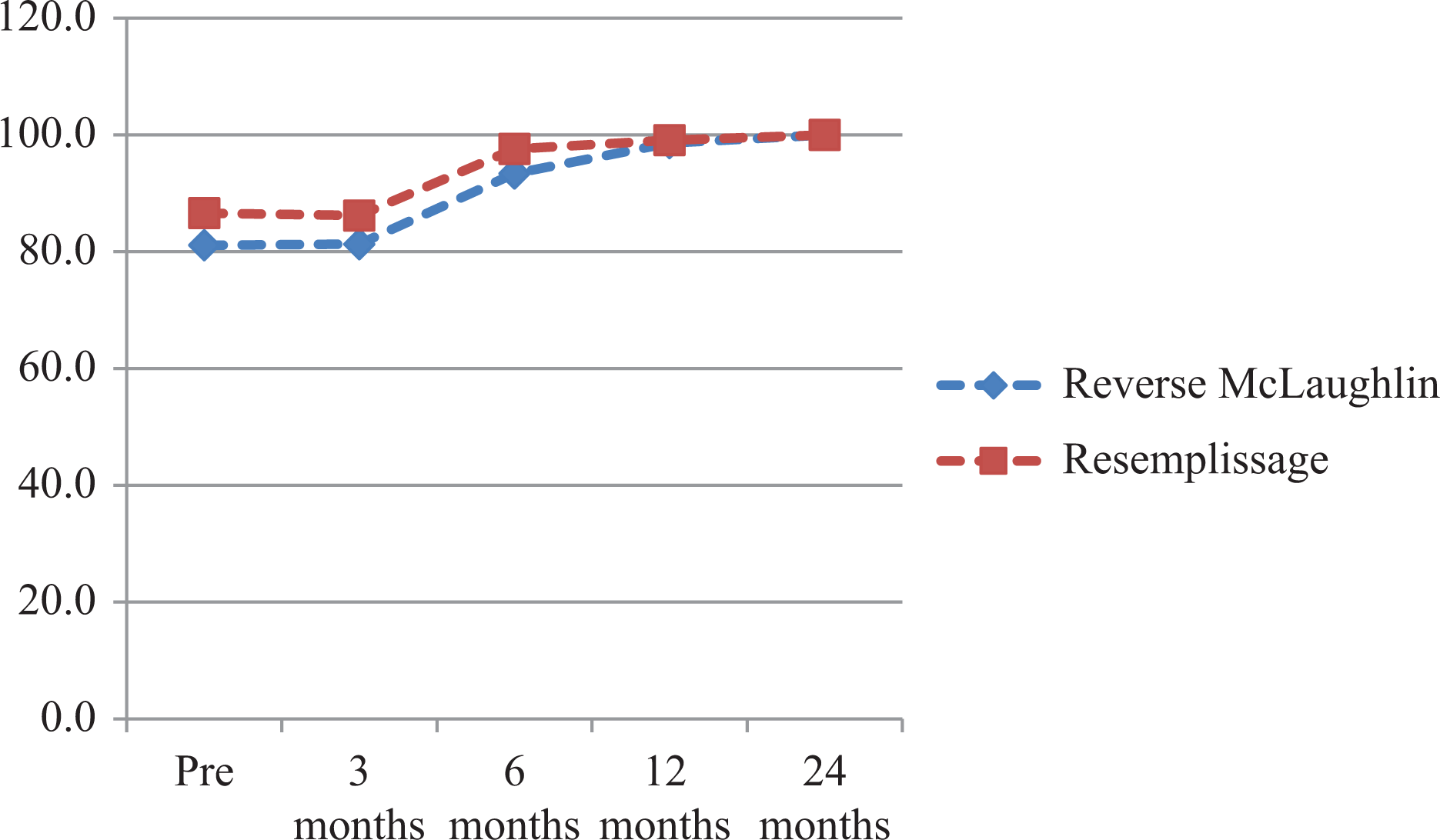
Mean ASES scores of the “reverse McLaughlin” and remplissage groups. ASES: American Shoulder and Elbow Surgeon.
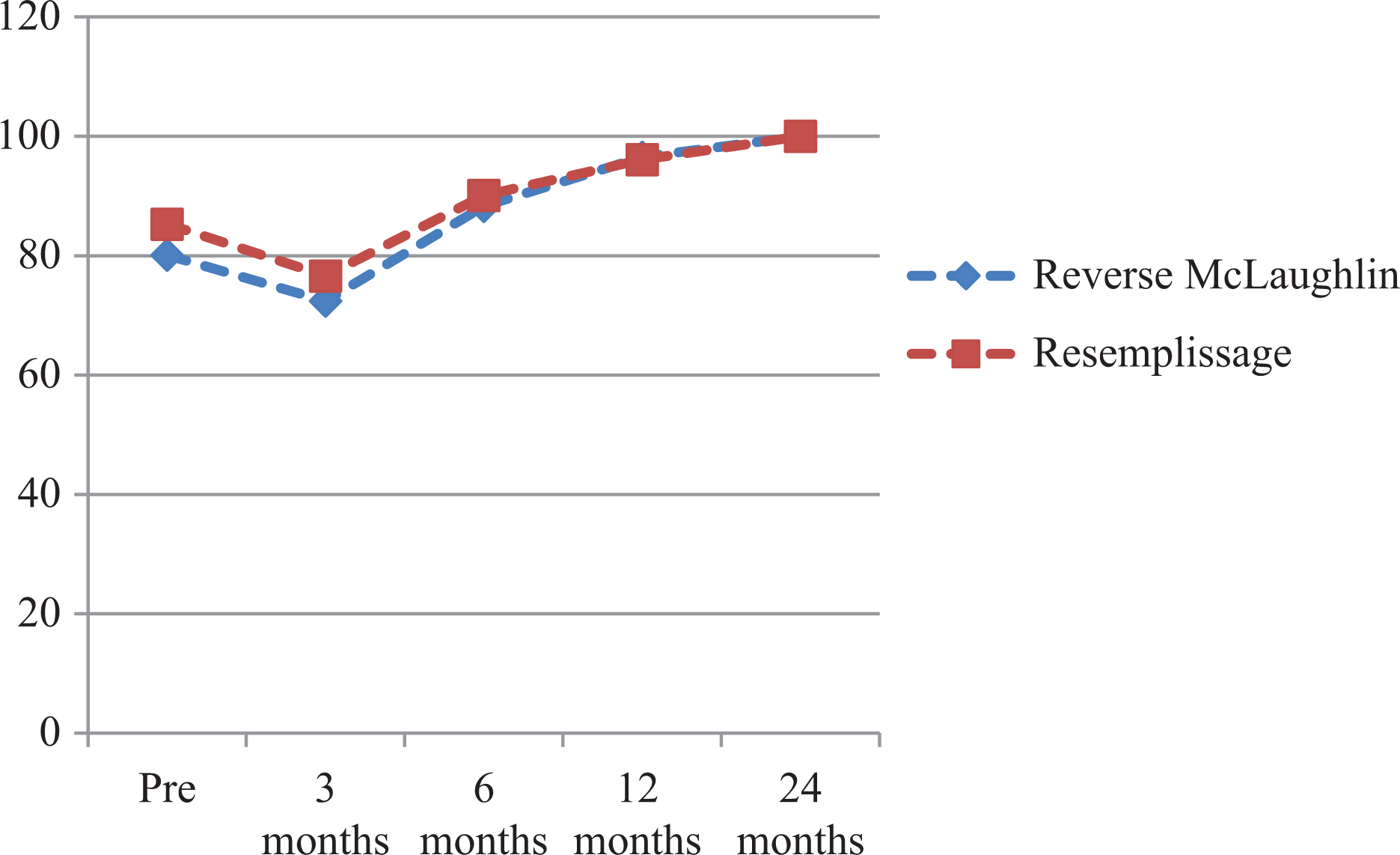
Mean Constant scores of the “reverse McLaughlin” and remplissage groups.

(a) Mean SF-36 PCS scores of the “reverse McLaughlin” and remplissage groups. (b) Mean SF-36 MCS scores of the “reverse McLaughlin” and remplissage groups.

(a) Mean ER (arm at side in degrees) of the “reverse McLaughlin” and remplissage groups. (b) Mean Constant score (IR) of the “reverse McLaughlin” and remplissage groups. ER: external rotation; IR: internal rotation.
ASES score
There were no significant differences in the preoperative scores in the two groups of patients. The two groups showed similar improvements in the postoperative scores over 3 months, 6 months, and 1 year postoperatively (Figure 6).
Constant score
A similar preoperative Constant score was documented for both groups of patients. Improvement in scores was similar over the different time periods. At 1 year, the Constant score for the Reverse McLaughlin group was 96.5 (range 87–100) while that for the remplissage group was 96.1 (range 84–100) (Figure 7).
SF-36 scores
The mean SF-36 PCS scores and SF-36 MCS scores were similar between the two groups, and the same pattern was observed over the following time points: 3 months, 6 months, and 1 year postsurgery (Figure 8).
External and internal rotation
The results of the functional external rotation (ER) are summarized in Figure 9(a) and (b). There were no significant differences in the mean ER between the two groups preoperatively and at 3 months, 6 months, and 1 year postoperatively.
The results of the mean Constant (internal rotation (IR)) range of movement scores are summarized in Figure 9. There were no significant differences in the mean Constant (IR) score between the two groups preoperatively and at 3 months, 6 months, and 1 year postoperatively (Figure 9).
Complications
One patient in the reverse McLaughlin group redislocated the operated shoulder after a fall 2.5 years postoperatively, which required a manipulation and reduction under sedation. She was treated nonsurgically and did not incur any further episodes of dislocation.
One patient in the remplissage group dislocated the operated shoulder 13 months postoperatively during overhead exercises in the gym. He underwent an arthroscopic Laterjet procedure and recovered well postoperatively. He did not experience any further dislocations in the further 1 year of follow-up after the procedure. None of the other cases required revision surgery or encountered complications.
At the final clinical follow-up, all patients had returned to work. Six of the eight patients in the reverse McLaughlin group and seven of the nine patients in the remplissage group had returned to their pre-injury sports. There was no instability subjectively or objectively on apprehension testing in any of the patients.
Discussion
We have shown that the reverse McLaughlin procedure has comparable clinical outcome score to the remplissage procedure carried out at our institution. Garcia et al. reported an average ASES score post-remplissage of 89.3 at an average follow-up time of 60.7 months. 10 Merolla et al. used the same procedure and reported a mean Constant–Murley score of an increase from 62.9 ± 7.1 preoperatively to 90 ± 5.2 at a median follow-up of 39.5 months. 11 Similarly, Wolf and Arianjam reported a postoperative mean Constant score of 92 ± 10 at an average follow-up of 58 months. 5 Our outcomes with both the remplissage and the reverse McLaughlin procedures are comparable to these previous works. The reverse McLaughlin procedure in our view is simpler to perform and easier to teach than the remplissage procedure, which has a steep learning curve. The time taken to perform this procedure is similar to that for the remplissage at our institution. Park et al. reported an estimated time of 2 h for the Bankart repair and the remplissage procedure. 8
The remplissage procedure involves a tenodesis of the infraspinatus and the underlying capsule into the bony defect on the humeral head. Such a tenodesis would naturally restrict internal rotation of the shoulder. This effect is likely to be more prominent if the procedure is carried out with the shoulder in external rotation to create a greater working space for the surgeon to carry out the remplissage. Restriction of external rotation is expected as the length of free infraspinatus tendon at play during the external rotation is severely limited by the tenodesis. Previous work on clinical and cadaveric have shown this restriction in rotation. 4,9 –11 Our study was, however, unable to show a significant difference in rotation, probably attributed to the small number of cases studied.
All the adverse effects of the remplissage procedure are eliminated with the reverse McLaughlin procedure. The excellent functional outcome with the standard McLaughlin procedure 17 for posterior shoulder dislocations is also reproduced in the reverse McLaughlin procedure that we have described.
Our technique moves the infraspinatus medially into the Hill–Sachs defect and hence is unlikely to affect ER and more importantly IR. The restriction in rotation with the remplissage had its main effects in those engaged in throwing sports. In a 5-year follow-up after the remplissage procedure, 65.5% of throwers reported problems throwing and 58.6% felt that they could not normally wind up throwing a ball. 10 Direct rates of return to overhead sports were 69% for basketball, 50% for baseball, and 50% for football. 10 The reverse McLaughlin procedure may be a suitable alternative for those engaged in throwing activity.
The strength of this study is that the clinical examination findings and postoperative outcome scores were studied by personnel who were not involved in the initial surgical management and were blinded to the surgical approach used in these patients, thus minimizing bias. Despite the small numbers, this is a novel technique that has not been reported previously.
There are recognized limitations of this study. The small sample size and the retrospective nature of this study limit the strength of the conclusions we can draw from our results. As mentioned earlier, the overall incidence of Hill–Sachs lesions requiring surgery is relatively low.
This novel technique we describe for engaging Hill–Sachs lesions is cheap and easily performed, without a significant learning curve. Compared to the remplissage, we feel our procedure is simpler to perform being no more than a miniopen cuff repair. The procedure can be performed using sutures anchors or transosseous sutures technique that will reduce the cost of the procedure. The learning curve compared to the remplissage is likely to be less steep. We have shown the good functional outcomes obtained via this technique to be at least equivalent to those obtained via the remplissage technique performed in our local center as well as in other centers. Future multicenter studies or comparative studies with a larger number of patients could potentially clarify some the issues raised in this study.
Conclusion
This novel surgical technique, the reverse McLaughlin procedure for engaging Hill–Sachs lesions, is simple to perform and is associated with functional outcomes and range of motion at least equivalent to those obtained via the remplissage technique. It may be a suitable alternative to the latter.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.