
Abstract
Purpose:
Cup setting with only an alignment guide has been reported to be inaccurate in the lateral decubitus position in total hip arthroplasty (THA). We assessed the accuracy of cup positioning using only the alignment guide technique via a modified Watson Jones approach in the lateral decubitus position.
Methods:
Two hundred hips of 189 patients underwent THA from October 2014 to September 2016 via a modified Watson Jones approach. In the final sample, 181 hips of 171 patients (35 males, 136 females) were included in this investigation. The alignment of the cup was evaluated by an anteroposterior radiograph of the pelvis 1 week after surgery. Measurements were divided into safe zone determined by Callanan and Lewinnek.
Results:
There were 168 (92.8%) acetabular cups that were placed within the safe zone for both inclination and anteversion based on the safe zones defined by Lewinnek, and 134 (74%) acetabular cups that were placed within the safe zone defined by Callanan. Multiple logistic analysis showed that the laterality and the addition of the confirmation method were indicators for malpositioning of combined inclination and anteversion.
Conclusion:
Our data suggested that even if special tools were not used in the lateral decubitus position, using only the alignment guide enabled cup positioning to be achieved with 92.8% accuracy in the Lewinnek safe zone and 74% accuracy in the Callanan safe zone. Multiple logistic analysis showed that the laterality and the addition of a confirmation alignment guide influenced the accuracy of cup positioning.
Keywords
Introduction
The orientation of the acetabular cup has been shown to be correlated with the risk of dislocation, 1 –3 range of motion, 4 functional outcome, 5 and implant survival. 6 While several studies suggest optimal orientation ranges, most indicate acceptable anteversion from 0° to 30° and acceptable inclination from 30° to 50°. 7 –10 Lewinnek et al. 7 reported a safe orientation which was 5°–25° anteversion and 30°–50° inclination. The Callanan safe zone is defined as an anteversion from 5° to 25° and an inclination from 30° to 45°. 10 Most surgeons place the cup manually or using an alignment guide, although these methods have been reported to be inaccurate. 10 –12 computed tomography-based navigation systems and other tools have been reported to improve cup alignment accuracy. 13,14 However, navigation systems are costly, so they are used only in some institutions. Therefore, freehand cup positioning and positioning with an alignment guide are popular methods for cup placement. The improvement of cup accuracy with freehand techniques was reported using the direct anterior approach in the supine position. 15 Conversely, acetabular component accuracy from the lateral decubitus position has generally been inferior, with safe zone landing rates ranging from 59% to 72%. 10,15,16 This difference is due in part to loss of the surgeon’s “pelvic proprioception” in the lateral decubitus position, as compared with the supine position. 15 However, the lateral decubitus position has advantages over the supine position in terms of intraoperative impingement assessment. In 2004, Bertin and Rottinger published a description of the anterior muscle sparing approach to the hip in the lateral decubitus position (modified Watson Jones approach). 17 The modified Watson Jones approach has the advantage of utilizing an inexpensive attachment to a standard table, with the extremity prepped free allowing range of motion and stability assessment. 18 We believe that in the lateral decubitus position, accurate cup placement is possible as long as great care is taken. The purpose of this investigation is to determine whether a popular cup placement technique that uses only an alignment guide is sufficient for accurate cup alignment using the modified Watson Jones approach in the lateral decubitus position.
Materials and methods
This investigative protocol was conducted with the approval of our institutional ethics committee. In accordance with the requirements of this review, all patients provided informed consent. Two hundred hips from 189 patients underwent total hip arthroplasty (THA) from October 2014 to September 2016 via the anterolateral approach in the lateral position (modified Watson Jones approach). The alignment guides of all models were specially made to set operative anteversion and inclination to 20° and 40°, respectively. Patients whose cup alignment was not planned for 20° anteversion and 40° inclination by preoperative assessment were excluded (19 hips, whose cup anteversion was not planned for 20°). In the final sample, 181 hips of 171 patients (35 males, 136 females) were included in this investigation. Cementless acetabular and femoral components were used for all patients. The medical records database was used to obtain demographic information for each patient, including gender, body mass index (BMI mean = 23.1 ± 3.6 kg/m2; standard deviation), age (mean = 64.9 ± 9.9 years), and laterality of the operated hip. The average surgical duration was 83.2 ± 19.7 min. Various cementless acetabular components were used including Continuum (n = 36; Zimmer Biomet, Warsaw, Indiana, USA), G7 (n = 45; Zimmer Biomet), SQRUM TT (n = 99; KYOCERA, Kyoto, Japan), and Trident HA (n = 1; Stryker Orthopaedics, Mahwah, NJ, USA). A preoperative diagnosis of secondary osteoarthritis (OA) due to developmental dysplasia was made in 126 hips (Crowe I, 110 hips; Crowe II, 10 hips; Crowe III, 3 hips; Crowe IV, 3 hips), primary OA in 18 hips, trauma in 13 hips, osteonecrosis in 8 hips, OA after pelvic or femoral osteotomy in 5 hips, rheumatoid arthritis in 3 hips, subchondral insufficiency fracture in 3 hips, rapidly destructive coxopathy in 3 hips, and OA after Perthes disease in 2 hips. Preoperative CT scans for preoperative planning were conducted on all patients using the CT-based templating software ZedHip (Lexi Co, Tokyo, Japan).
Surgical procedure
All surgeries were performed on an operating table, the lower half of which could be split for the operative leg to be extended, adducted, and externally rotated. Surgery was performed by a single surgeon (TN) using the modified Watson Jones approach. Preoperatively, the three-dimensional CT template was carefully checked for bony spurs, pelvic alignment, and cup coverage. The patients’ trunks were positioned along the longitudinal axis of the table. Preoperatively, the fixation devices of the pelvis were positioned on the bilateral anterior superior iliac spine and sacral bone with three points to immobilize the patients’ trunks. Pelvic tilt was confirmed by palpating the pubic symphysis and anterior superior iliac spine, and pelvic obliquity was altered by inclining the operating table preoperatively. We marked the wall of the operating room toward the patient’s head with a line extending from the body axis of the patient and referred to it for cup positioning. The skin incision was minimally invasive, and incision length was measured in all surgeries. The muscular plane between the gluteus medius laterally and tensor fasciae latae medially was developed bluntly, and the femoral neck was cut. The acetabulum was reamed, and the final acetabular component was placed using a press fit technique with an offset handle. The cup positioning angle was set in an operative inclination of 40° and 20° anteversion (radiographic inclination 41.8° and radiographic anteversion 15.2°). To prevent pelvic tilt due to cup hammering, an assistant suppressed the buttocks from the rear to prevent pelvic swaying backward. When the cup was fixed, the surgeon held a cup holder and confirmed the axis of the cup holder and the abduction angle while an assistant confirmed the anteversion angle of the guide from the operative field. From September 2015, the alignment guide confirmation from the remote position on the leg side of the patient was performed by both a surgeon and an assistant. An intraoperative radiograph was not taken in any of the surgeries.
Measurements
The alignment of the cup was evaluated by an AP radiograph of the pelvis 1 week after surgery. An AP radiograph of the pelvis was centered over the superior margin of the pubic symphysis. A single examiner (JY) measured the cup alignment by Lewinnek’s method 7 (Figure 1). A cross-table lateral radiograph was used to determine whether the cup was anteverted or retroverted. The measurements of cup alignment were divided into two different safe zones including that of Lewinnek et al., 7 which was 5°–25° anteversion and 30°–50° inclination, and Callanan’s safe zone, which was an anteversion from 5° to 25° and an inclination from 30° to 45°. 10
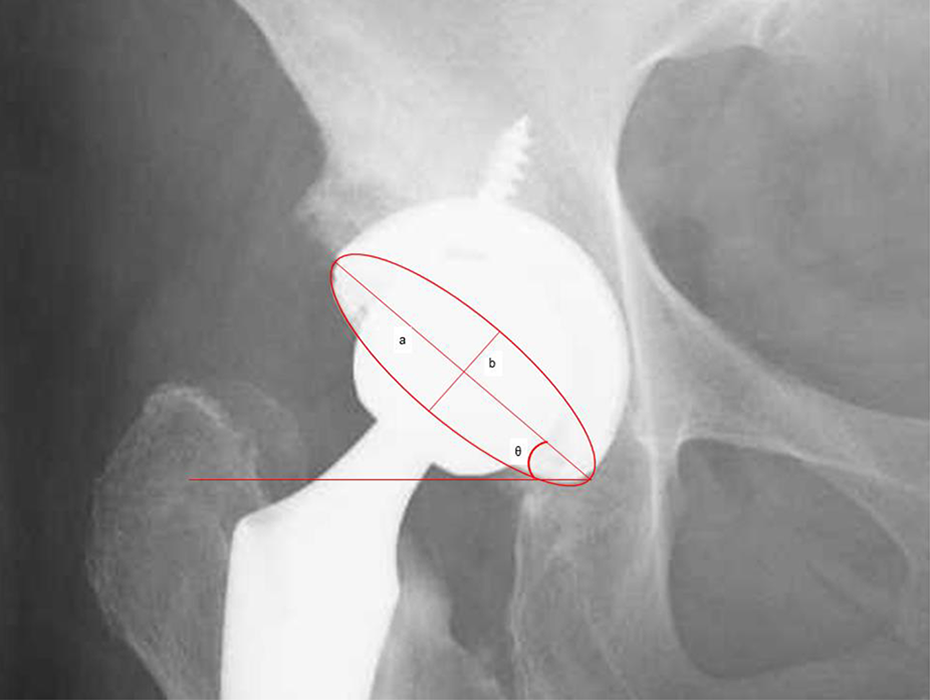
The geometry of the hip outlined using the circle theorem, which can be used to calculate acetabular version. The inclination angle, θ, was calculated from the angle between teardrop line and the major axis of the ellipse (line a). The anteversion angle was calculated from the ratio between the lengths of the major (line a) and minor axes (line b) of the ellipse referred to Lewinnek et al. 7
Statistical analysis
Patient and surgeon factors that were independent predictors of malpositioned cups based on both abduction and version angles in the Callanan safe zone and the Lewinnek safe zone were determined using binomial logistic regression, and adjusted odds ratios (ORs) and their 95% confidence intervals were calculated. The variables included the patient’s age, BMI, sex, the operated side, the length of the skin incisions, cup size, cup type, and the addition of the confirmation methods. Variables with p values < 0.2 by univariate analysis were considered for the multivariate model. We made a scatter diagram and confirmed no multicollinearity, which showed linear relations existed. An OR for the increased chance of malpositioning was calculated for all factors identified from the multivariate analyses. These ratios indicate the increased risk of malpositioning based on Callanan and Lewinnek. Statistical analyses were performed using SPSS Statistics version 19 (IBM SPSS Statistics 23.0; IBM, Armonk, New York). Correlations were considered significant when p < 0.05.
Results
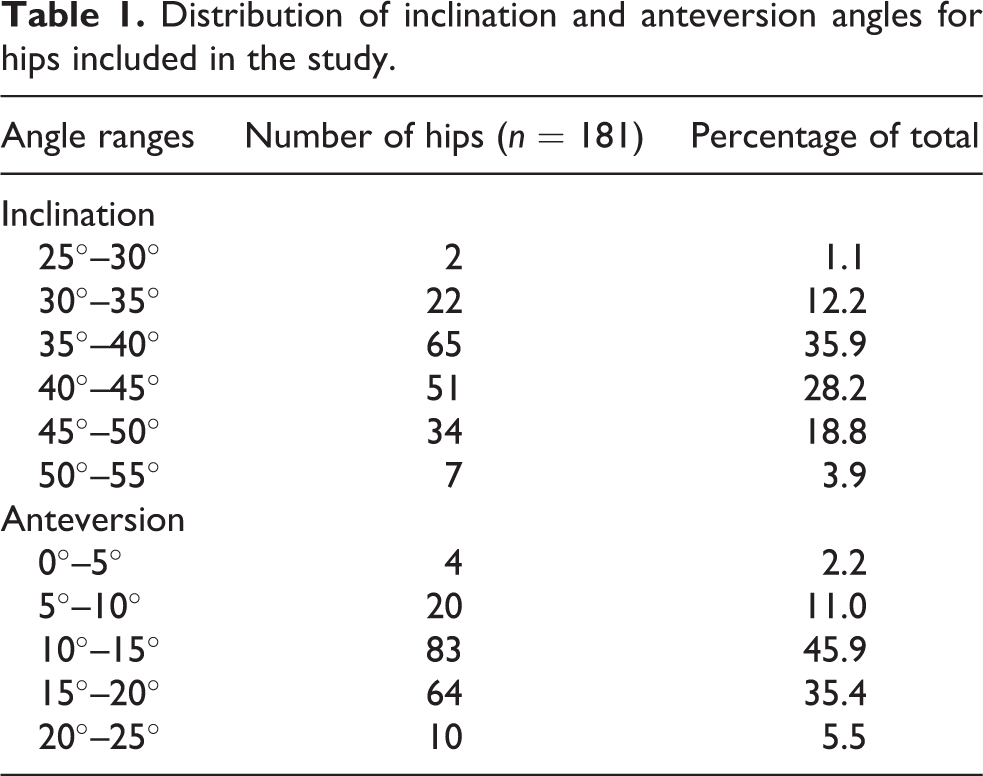
There were no postoperative hip dislocations in our investigation. Dislocations were determined based on follow-up appointments with patients seen postoperatively at 2 weeks, 3 months, and 1 year. The average radiographic anteversion was 14.1 ± 3.96° (range, 0.35°–24.22°). The average radiographic inclination was 40.7 ± 5.15°(range, 25.68°–53.72°). The frequency distribution for all angles in the study is shown in Table 1. There were 168 (92.8%) acetabular cups placed within the safe zone for both inclination and anteversion based on the safe zones defined by Lewinnek et al. 7 and 134 (74%) acetabular cups that were placed within the safe zone defined by Callanan et al. 10 A scatterplot shows the inclination and anteversion angles with a window indicating the boundary of the optimal cup angles (Figure 2). The results of the univariate analysis correlating the malposition of the cup defined by Callanan and Lewinnek were shown in Table 2. Univariate analysis of the risk factors was shown in Table 2. The laterality (OR: 0.878, p = 0.028) and the addition of confirmation method had significant associations in univariate analysis (p < 0.2), which were included in a multivariate logistic regression analysis.
Distribution of inclination and anteversion angles for hips included in the study.

Scatter diagram of cup orientation. A scatterplot showing acetabular cup positioning in the two groups. The y-axis shows radiographic inclination and the x-axis shows radiographic anteversion. The red box shows the Callanan safe zone and the blue box shows Lewinnek’s safe zone.
Results of the univariate analysis correlating the malposition of the cup defined by Callanan and Lewinnek.a

CI: confidence interval; BMI: body mass index; LSI: length of skin incision
a Confirmation method, the addition of the confirmation by an assistant from outside operative field.
The laterality was the indicator for malpositioning of combined inclination and anteversion defined by Callanan’s safe zone. The addition of the confirmation was the indicator for malpositioning of combined inclination and anteversion defined by Lewinnek’s safe zone in the multivariate analyses, respectively (Table 3).
Results of the multivariate logistic regression analysis correlating the malposition of the cup defined by Callanan and Lewinnek.a

CI: confidence interval.
a Confirmation method, the addition of the confirmation by an assistant from outside operative field.
Discussion
In our investigation, the acetabular cup was placed 92.8% of the time in the safe zone by Lewinnek and 74% of the time in the safe zone by Callanan when using a modified Watson Jones approach with only the alignment guide technique. This investigation showed that the accuracy of cup positioning with the modified Watson Jones approach without special tools was comparable or better compared to previous reports using the freehand technique: Bosker et al. 11 reported 70.5% accuracy (30°–50° inclination and 5°–25° anteversion), Callanan et al. 10 reported 47% accuracy, and Soderquist et al. 15 reported 61% accuracy (30°–45° inclination and 5°–25° anteversion). Hananouchi et al. 19 reviewed past literature that compared the rate at which outliers of cup orientation occurred. According to the report, between 19.7% and 83.8% of the cases with conventional THAs did not achieve a range within 10° from the planned alignment of the cup, whereas using a navigation system reduced this range to 0–25.3%. 11,12,14,19 –21 These previous reports showed that cup positioning using an alignment guide could possibly be inaccurate. However, we believe that accurate cup positioning using the modified Watson Jones approach, even if the special tools are not used, is achieved if surgeons take great awareness for pelvic position and the alignment of cup positioning.
For accurate cup settings, surgeons should carefully control multiple factors: preoperative and intraoperative pelvis setting, 22 accuracy of the alignment guide, 23 and direction of the alignment guide. Previous studies reported the greatest variability in pelvic orientation was in rotation around the transverse axis, and preoperative assessment of pelvic tilt identifying the position of the pubic symphysis and anterior superior iliac spine was recommended for an accurate pelvic setting. 22
We preoperatively assessed the pelvic tilt and rotation for the neutral pelvic setting and adjusted the pelvic obliquity by tilting the operative table. Hassan et al. 24 reported 58% of cups positioned within the Lewinnek safe zone in the lateral decubitus position and detected the inaccuracy of the component due to the movement of the pelvis in the sagittal plane during surgery. During the hammering of the cup, the pelvis was pushed backward by hammering and a retractor. Therefore, suppressing the buttocks from the rear to prevent pelvic swaying posteriorly is important. The alignment guides we used in this study were all special models which set operative anteversion and inclination to 20° and 40° accurately. Furthermore, the direction of the alignment guide was confirmed carefully outside of the operative field. Multivariate logistic analysis suggests that the addition of the confirmation method, by which an assistant and a surgeon checked the alignment guide from outside the operative field, reduced the number of cups that was outside the safe zone of Lewinnek (Table 3). Of course, the improvement might be due to the improvement of the surgeon’s technique because the confirmation method was added after the study was begun. However, we believe that it is important that cup alignment is confirmed repeatedly and carefully by multiple persons.
Multiple logistic analysis showed that the laterality impacted cup accuracy, with right-sided surgery having a higher incidence of safe zone landings. Left-sided surgery significantly increased only inclination angle, while the anteversion angle was not influenced by the laterality (Table 4). The surgeon in this study is right-handed and placement within the safe zone defined by Lewinnek et al. for the right hip was 96.2% and the left hip was 88%. Placement within the safe zone defined by Callanan et al. 10 for the right hip was 92.5% and was 48% for the left hip. Interestingly, the difference of cup accuracy in the laterality was reported by Soderquist et al., 15 although their surgery was done by the direct anterior approach in the supine position. They reported that the difference could be explained by the position of the surgeon when placing the acetabulum; performing the procedure on the side of the dominant hand may allow for better maneuverability. Despite the patient’s position, surgeons must be concerned that laterality will influence cup positioning.
Hips inside the safe zone for right-sided and left-sided THA by a right-handed surgeon.

THA: total hip arthroplasty.
There were limitations to this study. First, THA in this study was done by a single surgeon. Therefore, the risk factor for cup malpositioning might be influenced by the surgeon’s technique. Second, the data were collected by an independent observer, which introduces uncertainty because measurements were made manually and not calculated using a computer algorithm. Furthermore, the measurement of cup positioning was based on an AP radiograph of the pelvis centered over the superior margin of the pubic symphysis. The measurement of radiographic anteversion of the cup may not be accurate when measured by CT or an AP radiograph of the hip. The anteversion angle may be underestimated because the center of the radiograph was not directly over the cups. Third, the sample size was small, and the study was retrospective. However, as far as we are aware there are no reports that evaluate the accuracy of cup positioning using the modified Watson Jones approach with only the alignment guide technique.
Conclusion
Our data suggest that even in the lateral decubitus position, using only the alignment guide without other tools enabled cup positioning to be achieved with 97.9% accuracy in the Lewinnek safe zone and 74% accuracy in the Callanan safe zone. Multiple logistic analysis showed that the laterality and the addition of confirmation of the alignment guide influenced the accuracy of cup positioning.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.