
Abstract
Purpose:
We compared preoperative and postoperative measures among workers’ compensation board (WCB) recipients and non-recipients and determined the impact of WCB receipt on the 1- and 2-year outcomes of rotator cuff repair.
Methods:
We retrospectively reviewed patients with full-thickness rotator cuff tears who underwent arthroscopic repair between September 2011 and September 2014. Patients were divided into two groups based on WCB status: WCB recipients and non-recipients. All patients returned for follow-up functional evaluations at 1 and 2 years after the operation. Four outcome measures were evaluated: visual analog scale (VAS) pain score, American Shoulder and Elbow Surgeons (ASES) score, the Shoulder Rating Scale of the University of California at Los Angeles (UCLA), and range of motion (ROM).
Results:
Seventy patients (38 males, 32 females) were evaluated, 20 of whom were WCB recipients. At 1 year after the operation, ASES, UCLA, and VAS scores as well as abduction ROM (Abd-ROM) had improved significantly in both groups. However, non-recipients showed significantly greater improvement than did WCB recipients in ASES, UCLA, and VAS scores and in forward flexion ROM and Abd-ROM (p = 0.000, 0.009, 0.002, 0.046, and 0.020, respectively). However, at 2 years after the operation (after the end of WCB), there were no significant differences in any clinical outcome between WCB recipients and non-recipients (p = 0.057, 0.106, 0.075, 0.724, and 0.787, respectively).
Conclusion:
Although workers’ compensation recipients who underwent arthroscopic rotator cuff repair had worse outcomes while receiving WCB benefits, the outcomes were similar after WCB benefits ended.
Introduction
Surgical repair of rotator cuff injuries effectively reduces pain and improves shoulder function and range of motion (ROM). However, several studies have reported that workers’ compensation board (WCB) benefit recipients with rotator cuff tears experience lower recovery rates and report lower patient satisfaction than do non-recipients. 1 –4 It has also been suggested that WCB recipients report worse pain and lower function before surgery compared to those with nonwork-related injuries. 2,4 –7 However, the factors most commonly believed to affect postoperative outcomes are fatty degeneration, diabetes mellitus, age, gender, smoking status, and tear size. 8 Therefore, recent studies have used regression or multivariate analyses to control for baseline differences between WCB recipients and non-recipients. 8,9 A multicenter study also demonstrated marked variability in patient populations treated by different shoulder surgeons. 10
Several factors affecting postoperative outcomes such as age, gender, and smoking status cannot be controlled by investigators, but other factors such as the number of surgeons, tear size, operation method, and surgical technique can be controlled. Although recent studies have controlled for some baseline differences using statistical methods, to our knowledge no study has explored the treatment of rotator cuff tears of limited size by a single surgeon using the same operative technique. Furthermore, no study has compared the occurrence of re-tear after rotator cuff repair between WCB recipients and non-recipients while considering baseline differences between the groups.
The purpose of the present study was to examine preoperative differences between WCB recipients and non-recipients and to determine the impact of WCB status on 1-year (before the end of WCB benefits) and 2-year (after the end of WCB benefits) postoperative outcomes. We hypothesized that patients with workers’ compensation claims would have worse outcomes while receiving WCB benefits and similar outcomes after WCB benefits ended, even after controlling for baseline differences.
Materials and methods
Patient selection
We retrospectively reviewed records of patients with full-thickness rotator cuff tears who underwent arthroscopic repair between September 2011 and September 2014 at our hospital. Patients were divided into two groups based on WCB status: WCB recipients and non-recipients. The following were used as inclusion criteria: (1) full-thickness supra- and/or infraspinatus tear of 1.0–3.0 cm in anteroposterior length, (2) repair of the rotator cuff tear using an arthroscopic suture bridge technique, (3) return for follow-up functional evaluations at 1 and 2 years after the operation, (4) postoperative confirmation of the integrity of the rotator cuff repair by magnetic resonance imaging (MRI) or ultrasonography (US), and (5) WCB duration greater than 1 year and less than 2 years after the operation in the WCB recipient group to investigate the impact of WCB receipt on 1-year (before the end of WCB benefits) and 2-year (after the end of WCB benefits) postoperative outcomes. The following were used as exclusion criteria: (1) age >70 years, (2) full-thickness rotator cuff tear of anteroposterior length <1.0 cm or >3.0 cm, (3) duration of WCB less than 1 year or more than 2 years after the operation in the WCB recipient group, (4) repair of the rotator cuff tear using a mini-open or open repair method, (5) combined full-thickness subscapularis tear requiring concomitant repair, (6) combined acromioclavicular joint arthritis requiring concomitant distal clavicle resection, (7) neurological involvement, (8) revision operation, (9) operation using the suture bridge technique after the conversion of a partial-thickness rotator cuff tear to a full-thickness lesion, (10) arthritic changes of the glenohumeral joint, and (11) postoperative identification of rotator cuff re-tear by MRI or US. One specialized musculoskeletal radiologist performed all follow-up US examinations using an IU-22 system (Philips Healthcare, Bothell, Washington, USA). MRI and US images were evaluated by an experienced radiologist. A recurrent tendon defect was diagnosed when a distinct hypoechoic or mixed hyper- and hypoechoic defect was visualized by US in both the transverse and longitudinal planes. A full-thickness re-tear was diagnosed when a focal defect was present in the rotator cuff into which the deltoid muscle could be compressed with a probe to separate the torn tendon ends or when the cuff retracted to such an extent that the torn ends could be distinctly visualized. MRI was used to classify the integrity of the tendon into one of two categories: (1) intact (sufficient thickness, Sugaya types I and II) or (2) insufficient/not healed/re-torn (ranging from insufficient thickness (<50% normal cuff thickness) to discontinuity, Sugaya types III–V). 11
The study was approved by our institutional review board (IRB) and the need for informed consent from all patients was waived (IRB No. 2011-08-009).
Surgical technique and evaluation
All operations were performed by a single shoulder surgeon with the patient under general anesthesia and in the beach chair position. The conventional suture bridge repair method was developed by Park et al. 12 Under arthroscopy, the rotator cuff footprint was debrided. Depending on the tear size, one or two suture anchors (4.5 or 5.5 mm; Bio-Corkscrew, Arthrex, Naples, Florida, USA) were placed in the medial row. Both limbs of each of the two sutures perforated the tendon medially to establish parallel horizontal mattress stitches for each medial anchor. Knot tying was performed for each mattress stitch. To establish the lateral row, a suture bridge lateral-row repair technique was used to fully insert two knotless anchors (3.5 or 4.5 mm; Bio-PushLock, Arthrex) at an angle perpendicular to the cortical surface of the humerus.
The maximum anteroposterior length of each rotator cuff tear was measured using a calibrated probe introduced through the anterior or posterior portal under arthroscopic observation from the posterolateral or lateral portal. The maximum mediolateral length of each tear was estimated on preoperative oblique coronal T2-weighted MRI. MRI was used instead of arthroscopy to measure the mediolateral length of each tear due to considerable changes in this dimension according to shoulder position, especially abduction (Abd; Table 1). All measurements were performed by a single shoulder surgeon.
Demographic and surgical data.

WCB: workers’ compensation board.
a Based on separate paired t test; p < 0.05 denotes statistical significance.
No intra- or perioperative complication occurred, and no patient experienced neural injury, wound infection, or suture anchor problems.
Clinical evaluation
All patients returned for a follow-up functional evaluation at 1 year and 2 years after the operation. Four outcome measures were evaluated: visual analog scale (VAS) pain score, American Shoulder and Elbow Surgeons (ASES) score, the Shoulder Rating Scale of the University of California at Los Angeles (UCLA) score, and ROM. Active ROM was measured using a goniometer; passive ROM was not measured. Active ROM, including forward flexion (FF) and Abd, was measured with the patient in a standing position, and external rotation was assessed while the patient was standing with the arm in an adducted position.
Statistical analyses
The level of significance was set at p < 0.05. Comparisons between WCB recipients and non-recipients were performed using the χ 2 test for patient characteristics and independent t test for preoperative tear size. An independent t test was used to compare pre- and postoperative 1-year ROM and ASES, UCLA, and VAS scores. A paired t test was used to compare ROM and ASES, UCLA, and VAS scores between the two groups at 1 year and 2 years after the operation. All statistical analyses were performed using SPSS software (version 19.0 for Windows; SPSS Inc., Chicago, Illinois, USA). SAS software (version 9.1; SAS Inc., Cary, North Carolina, USA) was used to perform a power analysis with α = 0.05 for a sample size of 20 to evaluate pre- and postoperative ROM and ASES, UCLA, and VAS scores. The power of our study was estimated to be at least 0.97 for postoperative VAS scores, which was statistically significant.
Postoperative management
All patients received standardized pre- and perioperative care at our institution. The same regimen was prescribed to all patients, regardless of rehabilitation location or WCB status. Postoperatively, we prescribed the use of a shoulder immobilizing sling with an Abd pillow and provided instructions to maintain the shoulder at 30–40° internal rotation and 20° Abd. Patients began gentle passive FF of the affected arm using the unaffected arm in the second postoperative week. The sling with the Abd pillow was removed 6 weeks postoperatively, and active ROM mobilization was started. Active resistance muscle strengthening exercises were started after 12 weeks using Thera-Band (HCM-Hygenic Corporation, Batu Gajah, Malaysia). At 3–4 months after surgery, patients were permitted to perform light activities. Sports and heavy labor were allowed after 6 months.
Results
Overall, 70 consecutive patients (38 males, 32 females) who met the inclusion criteria (and no exclusion criteria) were identified, for a total of 54 affected right and 16 affected left shoulders. Among these, 20 patients (28.5%) were WCB recipients. Important demographic differences between WCB recipients and non-recipients are listed in Table 1.
Integrity of the repaired cuff of all patients was confirmed by follow-up MRI (n = 34) or US (n = 36). The average follow-up period for radiological evaluation was 8.7 months (range, 4–24 months) after the operation.
Preoperative evaluation revealed no significant differences between WCB recipients and non-recipients in ASES, UCLA, or VAS scores or forward flexion ROM (FF-ROM) (p = 0.332, 1.181, 0.921, and 0.109, respectively), except for abduction ROM (Abd-ROM; p = 0.008; Table 2). At 1 year after the operation, the ASES, UCLA, and VAS scores and Abd-ROM had improved significantly in both groups (all p < 0.05; Table 3). However, non-recipients showed significantly greater improvement than did WCB recipients in ASES, UCLA, and VAS scores, as well as FF-ROM and Abd-ROM (p < 0.001, p = 0.009, 0.002, 0.046, and 0.020, respectively; Table 4).
Comparison of preoperative functional scores between the two groups (mean ± SD).

SD: standard deviation; WCB: workers’ compensation board; ASES: American Shoulder and Elbow Surgeons score; UCLA: Shoulder Rating Scale of the University of California at Los Angeles score; VAS: visual analog scale pain score; FF-ROM: forward flexion-range of motion; Abd-ROM: abduction-range of motion.
a Based on separate paired t test; p < 0.05 denotes statistical significance.
Comparison of preoperative and postoperative 1-year functional scores (mean ± SD).

SD: standard deviation; WCB: workers’ compensation board; ASES: American Shoulder and Elbow Surgeons score; UCLA: Shoulder Rating Scale of the University of California at Los Angeles score; VAS: visual analog scale pain score; FF-ROM: forward flexion-range of motion; Abd-ROM: abduction-range of motion.
a Based on separate paired t test; p < 0.05 denotes statistical significance.
Comparison of postoperative 1-year functional scores between the two groups (mean ± SD).
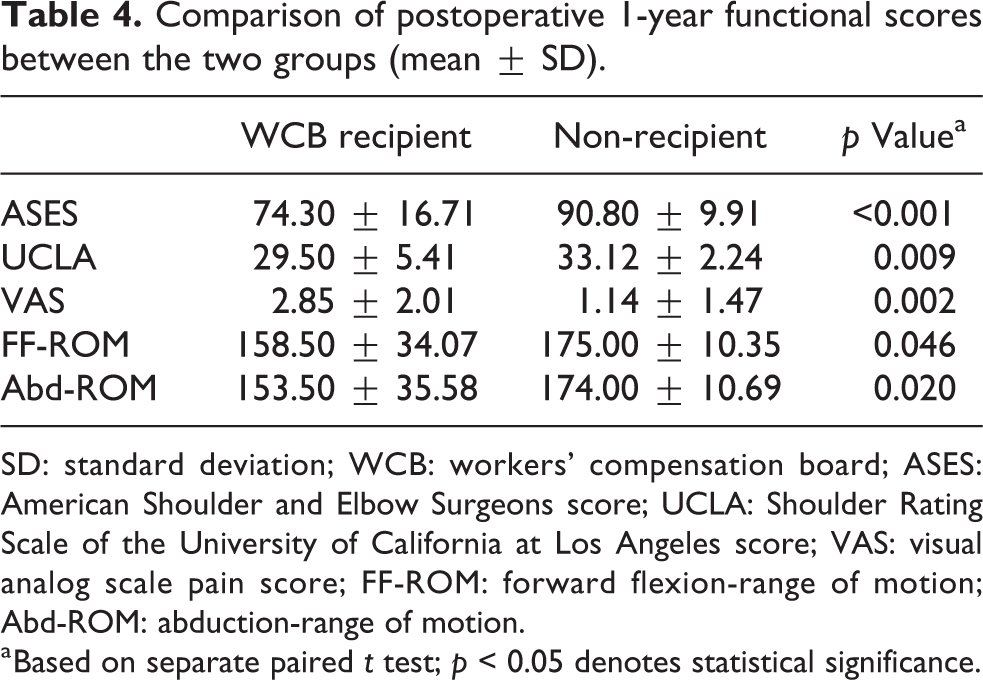
SD: standard deviation; WCB: workers’ compensation board; ASES: American Shoulder and Elbow Surgeons score; UCLA: Shoulder Rating Scale of the University of California at Los Angeles score; VAS: visual analog scale pain score; FF-ROM: forward flexion-range of motion; Abd-ROM: abduction-range of motion.
a Based on separate paired t test; p < 0.05 denotes statistical significance.
However, at 2 years after the operation (after WCB benefits had ended), there was no significant difference in any of the clinical outcomes between WCB recipients and non-recipients (p = 0.057, 0.106, 0.075, 0.724, and 0.787, respectively; Table 5).
Comparison of postoperative 2-year functional scores between the two groups (mean ± SD).

SD: standard deviation; WCB: workers’ compensation board; ASES: American Shoulder and Elbow Surgeons score; UCLA: Shoulder Rating Scale of the University of California at Los Angeles score; VAS: visual analog scale pain score; FF-ROM: forward flexion-range of motion; Abd-ROM: abduction-range of motion.
a Based on separate paired t-test; p <0.05 denotes statistical significance
Discussion
The purpose of the present study was to examine preoperative differences between WCB recipients and non-recipients and to determine the impact of WCB status on 1-year (before the end of WCB benefits) and 2-year (after the end of WCB benefits) postoperative outcomes. The main finding of this study was that workers’ compensation recipients who undergo arthroscopic rotator cuff repair had worse outcomes before the end of WCB benefits; however, the outcomes became similar after WCB benefits ended.
Balyk et al. 8 performed regression analyses to control for baseline differences between WCB recipients and non-recipients. Preoperatively, WCB recipients reported worse pain and function (Western Ontario Rotator Cuff (WORC) index and ASES scores) than did non-recipients, but ROM did not differ between the groups. WCB recipients showed poorer postoperative recovery outcomes according to all measures when baseline differences were not considered; however, only 6-month WORC scores were lower in WCB recipients when these differences were accounted for. The authors stated that clinicians should consider preoperative characteristics before concluding that WCB recipients experience poorer recovery after surgical repair. Henn et al. 9 performed multivariate analyses of Disabilities of the Arm, Shoulder, and Hand (DASH) and Short-Form 36 (SF-36) general health subscale scores using linear multivariate regression to control for confounding variables. 2,13,14 Preoperatively, WCB recipients had significantly lower scores on the Simple Shoulder Test (SST) and the SF-36 Physical Function and Social Function scales. At 1 year postoperatively, those patients also had lower SST, DASH, VAS, and SF-36 scores and showed less improvement in DASH and VAS measures of shoulder pain and function and in the SF-36 Bodily Pain and Role Emotional scales. A multivariate analysis controlling for confounding factors confirmed that workers’ compensation status was an independent predictor of lower DASH scores. The authors concluded that patients with workers’ compensation claims reported worse outcomes, even after controlling for confounding factors. In the present study, WCB recipients and non-recipients showed no preoperative differences in pain (VAS), function (UCLA, ASES), or FF-ROM. Moreover, there were no significant differences between the two groups in postoperative 2-year outcomes after WCB had ended. Interestingly, patients with workers’ compensation claims showed poorer 1-year postoperative outcomes, that is, before WCB benefits ended, in pain (VAS), function (UCLA, ASES), and Abd-ROM.
Multiple factors are associated with less favorable outcomes following rotator cuff repair, including age, 4,15 –17 sex, 15 –17 smoking status, 18 larger tear size, 15,19,20 poor tendon quality, 20 fatty degeneration of the cuff muscle, 21 and poor repair integrity. 22,23 Although surgical repair of rotator cuff tears can improve pain and shoulder function, previous studies have found that WCB recipients reported lower recovery rates than did non-recipients. 2 –4,6,7,13,24 Previous research has also suggested that WCB recipients exhibited poorer preoperative condition. 4,6,7,13,24 However, these studies have not controlled for differences in patient and injury characteristics and have not considered the potential effects of preoperative dissimilarities on postoperative recovery. Although several recent studies have performed regression or multivariate analyses to control for confounding factors and baseline differences between WCB recipients and non-recipients, these studies did not control for preoperative dissimilarities. 8,9 Although some factors affecting postoperative outcomes such as age, gender, and smoking status cannot be controlled by investigators, other factors can be controlled. In the present study, there was a significant difference in gender between the two groups; however, there was no significant difference in age, affected side, or smoking status. We also tried to reduce baseline differences that might affect postoperative outcomes, such as the involved rotator cuff, tear size, number of surgeons, surgical approach, surgical technique, and postoperative integrity of the rotator cuff.
The present study has some limitations. First, relatively few WCB recipients were included in the study, which limited the ability to generate significant results. Second, although all US evaluations were performed by an experienced musculoskeletal radiologist, this technique is examiner dependent. 25 However, we did not perform the US examination ourselves to avoid surgeon bias. 26 Third, although repair integrity was confirmed postoperatively, we did not analyze the effects of anatomical factors, such as fatty degeneration of the muscle or tendon quality, on the outcomes of rotator cuff repair. We were unable to assess preoperative muscle atrophy grades due to incomplete MRI scans, which lacked an appropriate Y-shaped view. Fourth, the effect of workers’ compensation status on the outcome may change over time, which may limit the generalizability of our results to patients after claim settlement. 9 We chose to perform the follow-up outcome evaluations at 1 year and 2 years after surgery. Finally, the characteristics of patients in different geographic areas vary, and workers’ compensation laws differ among states. These differences may also affect outcomes. 9 Moreover, secondary gain is very difficult to separate from the workers’ compensation claim process and is not directly assessed. 9
Despite these limitations, the present study has several strengths. First, all operations were performed by a single shoulder surgeon in the same hospital setting, thereby reducing variability in postoperative outcomes due to differences in the technical expertise of different surgeons. Second, we restricted the size of full-thickness rotator cuff tears included in the study to an anteroposterior length of 1.0–3.0 cm, thereby reducing variability in postoperative outcomes due to differences in tear size. Third, although controversy has surrounded long-term clinical outcomes following different rotator cuff repair methods or techniques, only the arthroscopic suture bridge technique was used. We believe that most small tears (<1 cm in anteroposterior length) do not require suture bridge or double-row repair. A recent systemic review has found no significant difference in re-tear rates between single- and double-row repairs of tears <1 cm in length. 27 Fourth, we performed postoperative MRI or US to evaluate the integrity of the repaired rotator cuff, thereby reducing variability in postoperative outcomes due to differences in cuff integrity.
Conclusion
Although workers’ compensation recipients who undergo arthroscopic rotator cuff repair had worse outcomes before the end of WCB benefits, the outcomes became similar after WCB benefits ended. Therefore, the hypothesis that patients with workers’ compensation claims would have worse outcomes following rotator cuff repair during WCB and similar outcomes after the end of WCB, even after controlling for baseline differences between WCB recipients and non-recipients, was supported.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.