
Abstract
Background:
Evaluating the effectiveness of total hip arthroplasty (THA) and total knee arthroplasty (TKA) often relies on accurate patient reporting of postoperative complications. Despite this, there is little research regarding the accuracy of patient reports. We aimed to determine the accuracy of patient-reported significant complications after THA and TKA.
Methods:
Patients were recruited prior to undergoing primary hip or knee arthroplasty at 19 high-volume hospitals. After surgery, follow-up of patients via telephone interviews at 35, 90 and 365 days recorded surgical outcomes including readmission, reoperation and venous thromboembolism (VTE). Patient-reported complications were verified via medical record audits and liaison with surgeons, general practitioners or other health professionals. Surgical and demographic information and patient-reported and verified complications were entered into a database. Patient-reported and verified complications were compared for readmission, reoperation and VTE.
Results:
The sample included 150 of 1811 patients who reported a total of 242 significant complications. Of the 242 patient-reported complications, 224 (92.6%) were correct (true positive). The type of complication had variable levels of accuracy in patient reports. Readmission to hospital was accurately reported by 90.2% (129/143) of patients. Reoperation (including any manipulations under anaesthesia, joint washouts, reductions of dislocated joints and revisions) was accurately reported by 98.7% (75/76) of patients. VTE was accurately reported by 86.7% (20/23) of patients.
Conclusion:
A high level of accuracy in patient-reported experience of complications was demonstrated following THA and TKA. Patient-reported complications may be reliably used for post-operative surveillance of joint replacement surgery.
Introduction
There is a growing demand for total hip arthroplasty (THA) and total knee arthroplasty (TKA) in Australia and elsewhere. 1 –4 Many studies have shown that most patients with end-stage arthritis achieve improved mobility and quality of life, reduced pain and disability and high levels of patient satisfaction after THA and TKA. 1,3 –13 However, THA and TKA are not without risk and are associated with complications such as venous thromboembolism (VTE) and infection.
Patient-reported complications are important in the context of clinical practice, and the incidence of these events is frequently used as an indicator of surgical quality for health services and in research. Patient-reported complications offer a convenient and meaningful method of measuring quality. This assumes that patients are accurate in the complications they report, yet the level of accuracy of patient reported complications after joint replacement surgery has not been extensively studied. 14,15
This study aims to measure the accuracy (true positive rate) of patient reporting of significant complications occurring after hospital discharge following THA and TKA.
Method
This study was conducted within the context of a large observational cohort study including 19 private and public hospitals in 5 states of Australia. Ethics approval was obtained through nine Human Research Ethics Committees. All participating patients gave informed consent prior to undergoing surgery. Patients were eligible if they were undergoing primary TKA or THA for osteoarthritis, able to speak English and available to participate in follow-up interviews.
Data were collected prospectively from patients and sites prior to and following surgery. At the time of consent, patients provided demographic information, general health information and provided baseline measures of pain, function and quality of life. Telephone follow-up interviews were conducted by investigators at 35, 90 and 365 days post-operatively to monitor progress, rehabilitation, complications and to repeat the patient-reported outcome measures (PROMs). The type of complications included in this study are shown in Table 1.
Type of complications and time frames for inclusion in study.
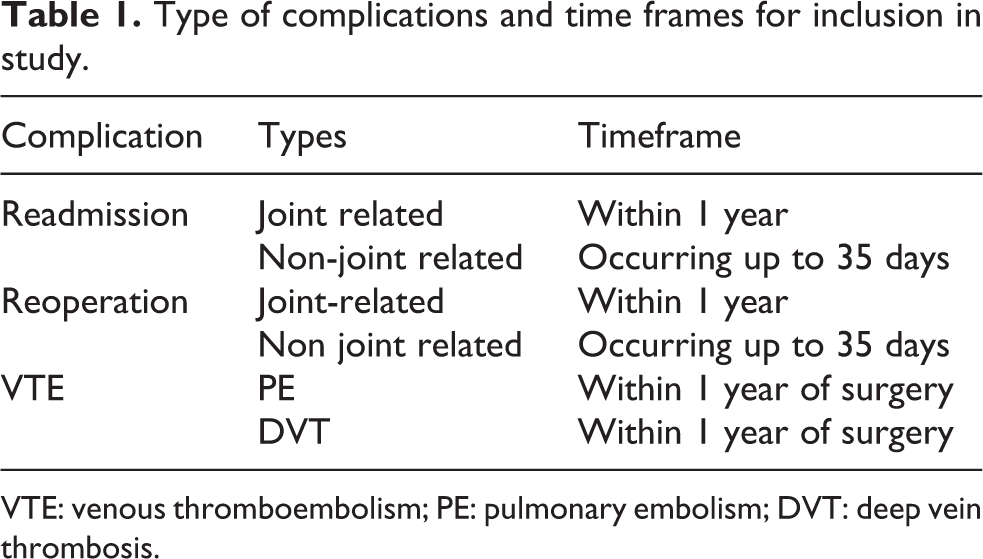
VTE: venous thromboembolism; PE: pulmonary embolism; DVT: deep vein thrombosis.
The accuracy of the nature, type and number of occurrences of each reported complication was verified through several methods: audit of medical records and communication with sites, general practitioners, treating surgeons and other hospitals. Data regarding the significant complications reported by patients and through verification and the level of agreement between them were reported for each type of complication. Occurrences of post-operative death were verified but not considered in this study, as death was not patient reported. We compared the type, time frame and management for each separate complication. Complications occurring beyond 1 year following surgery were beyond the scope of this study.
Patient reports and verified reports of each type of complication were coded as a series of dichotomous variables (yes or no). Accurate reporting for individual patients was defined as true positively reported complications. As the aim of the study was to investigate patient-reported complications, any complications discovered by audit that were not reported by a patient were not included.
The characteristics of the sample and surgical complications were described for all patients. Differences in co-morbid and demographic characteristics were compared for those patients whose values were accurate (true positive) compared to those whose values were inaccurate (false positive) in reporting complications using Pearson’s χ 2 test and the Mann–Whitney U test as appropriate. The level of accuracy for each type of patient-reported complication was reported as the proportion of reported complications that were correct.
Results
Demographics
The mean age was 68.5 years, and 48.7% of the sample were male. The proportion of patients who had their surgery in public hospitals was 48.7%. The proportion of TKA and THA were 68.7% and 31.3%, respectively. Just over a quarter of the sample completed high school. Only 23.7% of patients had no known co-morbid condition (see Table 2).
Sample characteristics of patients who reported complications.

Accuracy
Complications were reported by 12.4% of the sample (150/1822) and 88.7% of patients (133/150) were accurate. Many patients experienced multiple complications and 242 separate complications were reported. The most common type of complication reported by patients was readmission to hospital (95.3%), with 86.7% of these readmissions associated with joint-related complications.
The accuracy of all complications reported by patients was high (92.6%), with the degree of accuracy ranging from 77.3% for non-joint–related readmissions to 100% for pulmonary embolism. Only one person was not accurate in reporting a joint-related reoperation (98.7% accuracy). Three patients reported experiencing both joint- and non–joint-related admissions (see Table 3).
Patient report and accuracy of complications.
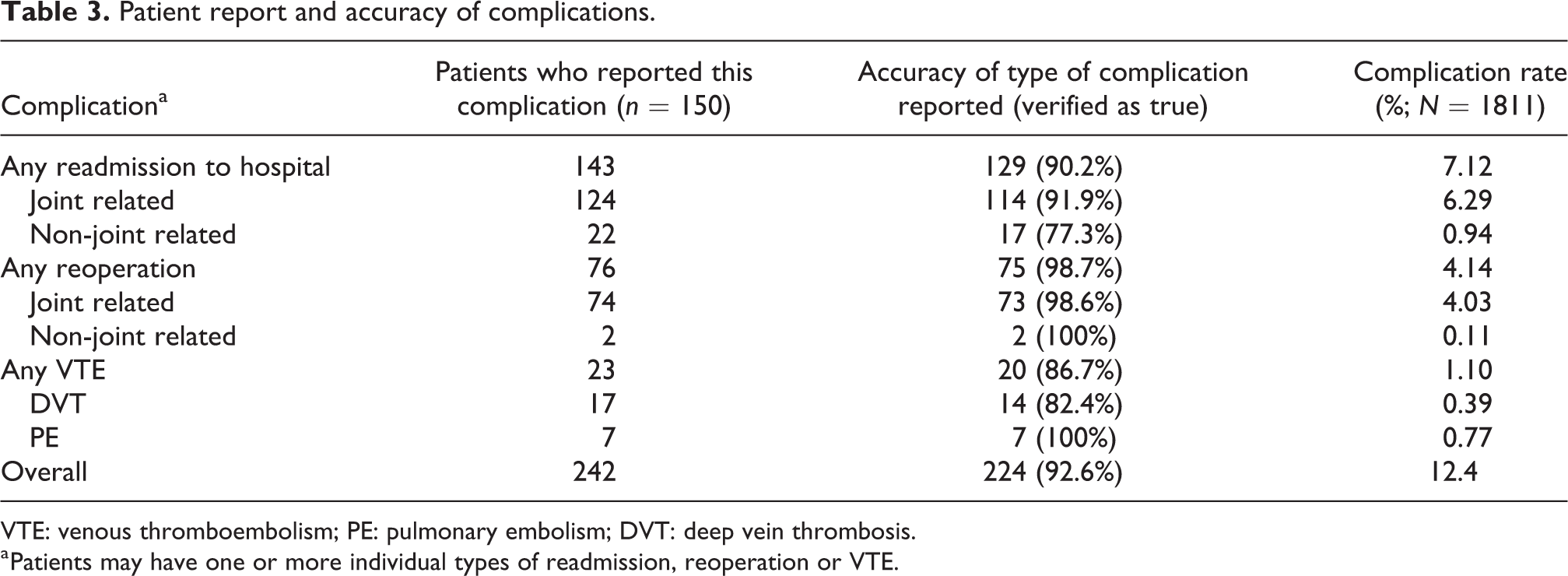
VTE: venous thromboembolism; PE: pulmonary embolism; DVT: deep vein thrombosis.
a Patients may have one or more individual types of readmission, reoperation or VTE.
Association between patient characteristics and accuracy
Differences in co-morbid and demographic characteristics were compared for those patients who were accurate compared to those who were inaccurate in reporting complications. There were no significant associations between accuracy and patient age, gender, public or private status, type of surgery, education or comorbidity.
Discussion
The overall accuracy of patients who reported complications after acute discharge was high (88.7%), consistent with other literature which demonstrated agreement between patients and clinicians ranging from 80% to 90%. 14,16 –18 We found that approximately 12% of patients experienced a significant complication within the first year of THA and TKA after acute hospital discharge. This rate was similar to other published studies. 14,19
While the accuracy and incidence of specific types of complications reported in this study was consistent with the literature, 14 –17,20 –22 there were varying degrees of accuracy for the different types of complications. While most patients who reported hospital readmissions were accurate, errors were mostly related to patients reporting presentations to outpatients or emergency departments (without overnight admission) as a hospital admission. This could be related to both the way questions were asked and different perceptions about the definition of hospital admission between patients and health professionals. The level of accuracy of patient-reported reoperations was high, consistent with a previous study. 17 All patients who reported a pulmonary embolism (PE) were correct, while only 82.4% of patients correctly reported deep vein thrombosis (DVT). Our accuracy rate for PE was higher than previous studies which reported 75–86.2%, but our DVT accuracy rate was within the range of previous reports (77.4–84.2%). 14,15 Incorrect reports of DVT may be attributable to patients’ lack of understanding between a complication and a normal physiological reaction of recovery to surgery such as swelling. 16 In this study, some patients considered haematoma, pain in their leg or ultrasound testing as a diagnosis of DVT.
Overall accuracy rates may also have been affected by the time frame of the reporting dates. Details of complications reported at the 1-year survey may not be accurately described, especially if these patients experienced complications that occurred early after the 90-day follow-up period.
The literature reports that accuracy of patient-reported outcomes may be influenced by type of surgery, number and nature of complications experienced, education and severity of co-morbidity. 6,14,16 –18,23 One study found that patients with more co-morbidities experienced higher complication rates and reduced accuracy of patient report. 16 However, our study did not demonstrate any association between accuracy and patient or surgical characteristics.
Contributions of study
This study has shown that patients can be a reliable source for post-discharge surveillance of complications after TKA and THA, allowing timely detection of complications. 24 This is important because patients experiencing complications are often admitted to different hospitals from their primary site. Furthermore, accurate patient reporting supports the use of PROMS, which can reduce surgeon bias and help drive service improvements. 14,17,18,23 The high reporting accuracy found in this study overall emphasizes the efficacy of incorporating patient reports into multidimensional methods of assessment to diagnose complications.
Limitations of study
This study only examined the accuracy of complications that patients reported. This excluded possible complications experienced by patients who reported no complication. Therefore, we were unable to report the true rate of complications and the rate of false-negative reports by patients. Reporting patient accuracy from the post-operative to discharge period was also not possible as we did not address acute complications which occurred during hospitalization from the primary surgery.
Furthermore, our study produced a small sample size of inaccurate patients which limited the analysis of associations between accuracy and patient characteristics. Categorization of data also may have influenced the sensitivity of these analyses.
Summary
A high level of accuracy in patient-reported complications was demonstrated, and the complication rate after THA and TKA was consistent with previous studies. Patient-reported complications can be reliably used for post-operative surveillance of joint replacement surgery to monitor patient outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.