
Abstract
Background
Understanding the impact of situational variables on surgical recovery can improve outcomes in total hip arthroplasty (THA). Literature examining hospital outcomes by season remains inconclusive, with limited focus on patient experience. The aim of this study is to investigate if there are differences in hospital and patient-reported outcomes measures (PROMS) after THA depending on the season of the index procedure to improve surgeon preoperative counseling.
Methods
A retrospective chart review was performed on patients undergoing primary THA at a single large academic center between January 2013 and August 2020. Demographic, operative, hospital, and PROMs were gathered from the institutional electronic medical record and our institutional joint replacement outcomes database.
Results
6418 patients underwent primary THA and met inclusion criteria. Of this patient population, 1636 underwent surgery in winter, 1543 in spring, 1811 in summer, and 1428 in fall. PROMs were equivalent across seasons at nearly time points. The average age of patients was 65 (+/- 10) years, with an average BMI of 29.3 (+/- 6). Rates of complications including ED visits within 30 days, readmission within 90 days, unplanned readmission, dislocation, fracture, or wound infection were not significantly different by season (P > .05).
Conclusion
Our findings indicate no differences in complications and PROMs at 1 year in patients undergoing THA during 4 distinct seasons. Notably, patients had functional differences at the second follow-up visit, suggesting variation in short-term recovery. Patients could be counseled that they have similar rates of complications and postoperative recovery regardless of season.
Keywords
Introduction
A plethora of modifiable and nonmodifiable preoperative factors have been examined to optimize outcomes for patients undergoing total joint arthroplasty (TJA). 1 However, little attention has been paid to the role of situational variables in preoperative decision making prior to joint replacement. There is a growing body of orthopedic literature regarding the effect of season on postoperative outcomes. Several of these studies examine the “July effect” of new fellows and residents, with no significant differences reported.2-4 However, complications following total knee arthroplasty (TKA) have been found to be higher during the summer months 5 with increased risk for infections found during warmer weather.6-8 In a large database study, total hip arthroplasty (THA) and TKA procedures performed in December were shown to have lower rates of complications with decreased lengths of stay postoperatively. 9 Alternatively, another study noted increased rates of periprosthetic infection following THA occur during the winter, 10 although this was not demonstrated in a population of unicompartmental knee arthroplasty patients. 11 No effect of season has been noted on post-operative wound complications after trauma to the foot, ankle or lower leg. 12 Another study found no difference in seasonal variation of complications 30 days after THA. 13 Taken as a whole, the body TJA literature remains inconclusive on the role of season of index surgery on outcomes. The majority of work within this field has focused on whether season of surgery impacts complications; there to the best of our knowledge this is the first study to investigate whether season of surgery effects patient-reported outcome measures (PROMs) and satisfaction following TJA.
Preoperative and post-operative PROMs are a standard practice in TJA. 14 These measures evaluate patients’ perceptions of their health and experiences, and are essential to providing patient-centered care. 15 Additionally, as measures of patient satisfaction, PROMs are increasingly utilized as indicators of health care quality, with the ability to influence health care policy and decrease inequalities within care systems. 16 Understanding the factors that impact PROMs are important for maximizing patient satisfaction and identifying areas for quality improvement. We hypothesize that season of index surgery may impact PROMs following THA. This effect may be impacted by variation in complication rate by season, if seen, with higher complication rates associated with lower PROMs. Yet additional environmental and behavioral may also play a role. Winter months in northeastern regions of the United States (where our institution is located) encourage a sedentary lifestyle, which may adversely impact patient postoperative mobility and recovery.17,18 Furthermore, increased rates of depression and Seasonal Affective Disorder occur during winter months19,20; such psychological conditions increase complications and decrease satisfaction among TJA patients, 21 and may similarly limit postoperative mobility and therefore recovery. Conversely, the summer months in northeastern United States are notable for increased ambient temperatures, a factor which increases microbe survivorship, but which also allows for increased patient post-operative activity and ability to be outside. 22 Thus, the role of season and its impact on patient satisfaction in recovery is poorly understood, with an unclear expected relationship between season of surgery and PROMs following THA.
The aim of this study is to investigate if there are differences in hospital and patient-reported outcomes after THA depending on the season of the index procedure performed in the northeastern United States. Better understanding of how season may affect patient-reported outcomes following THA will allow improved surgeon preoperative counseling prior to undergoing arthroplasty as an elective procedure.
Material and Methods
Patient Selection and Data Collection
A retrospective chart review was performed on patients undergoing primary total hip arthroplasty at a single large academic center in northern New England with 4 distinct seasons between January 1, 2013 and August 31, 2020. Institutional review board approval (IRB NET ID 1981001-1) was obtained, and the project was deemed not to constitute human subjects’ research. Inclusion criteria was set for patients over the age of 18 who received an anterior-based muscle-sparing THA, 23 the approach commonly used at our hospital. Patients undergoing revision THA, patients who had a preoperative diagnosis of septic arthritis, and patients with a discharge disposition of psychiatric hospital or expired were excluded. All cases performed by the only 3 arthroplasty surgeons performing THA were included for analysis. The primary outcomes of interest were the demographics, surgical, and dispositional outcomes of patients undergoing THA in different calendar seasons. Seasons were defined using the standard meteorological definition of 4 3 month periods, winter (December 1—February 28), spring (March 1—May 31), summer (June 1—August 31), and fall (September 1—November 30). 24
Demographic, operative, and hospital outcome data were obtained from the institutional electronic medical record. Demographic information collected included sex, age, American Society of Anesthesiology (ASA) score, preoperative diagnosis (degenerative joint disease [DJD]/osteoarthritis [OA], avascular necrosis [AVN], and fracture), and public or private insurance type. Operative variables collected included arthroplasty fixation (press fit vs cemented), procedure type (primary vs conversion), anesthesia time in minutes, procedure duration in minutes, estimated blood loss (EBL) in milliliters, transfusion requirement, and presence of an intra-operative complication. Hospital-reported outcomes included discharge disposition (to home, home health care service, skilled nursing facility, or rehabilitation facility), emergency department (ED) visit (within 30 days), average days after surgery for ED visit, readmission (within 90 days), average days after surgery for readmission, planned or unplanned readmission, presence of any complication (as well as specifically surgical complications), myocardial infarction (within 7 days), pneumonia (within 7 days), surgical site complication (within 30 days), pulmonary embolism (within 30 days), death (within 30 days), fracture (within 90 days), dislocation (within 90 days), mechanical complication (within 90 days), and joint or wound infection (within 90 days). Initially, 6421 patients were included. Patient-reported outcomes collected included preoperative, 6 weeks, 6 months, and 1 year Single Assessment Numeric Evaluation (SANE), pain, Hip Disability and Osteoarthritis Outcome Score Joint Replacement (HOOS JR), University of California, Los Angeles (UCLA), and Patient- Reported Outcomes Measurement Information System (PROMIS) mental/physical and satisfaction scores, all collected from an institutional joint replacement outcomes database. After excluding patients who were undergoing revision THA, patients who had a pre-operative diagnosis of septic arthritis, and patients with a discharge disposition of expired or psychiatric hospital, the data included 6418 patients.
Data Analysis
To assess the relationship between seasonality and our outcomes of interest, all demographic, patient-reported, and hospital-reported variables were analyzed with respect to season. Pearson’s Chi-square test was used for all normally distributed categorical variables, and the Wilcoxon rank sum test or Fisher’s exact test were used for non-normally distributed categorical variables and all continuous variables. Q-values were reported in all outcomes tables to correctly adjust for the False Discovery Rate for multiple testing.
Univariate regression models were created to analyze the relationship between patient- and hospital-reported outcomes and all covariates (cemented status, both hips, sex, age, BMI category, insurance category, and anesthesia type). Linear and logistic regression approaches were used according to the respective outcome (linear for continuous outcomes, logistic for binary outcomes). Final linear and logistic multivariable regression models were created using a combination of clinical expertise and purposeful selection (P < .2) with respect to each individual outcome; adjustment was made for year of index surgery. Any patients with missing data were excluded from regression analyses.
Modeling of patient-reported outcomes measures (PROMs) was limited by missing data (>50% of patients were missing 1 or more outcome values) impacting the accuracy and generalizability of PROMs regression model results. Descriptive analysis showing differences across season was utilized to assess PROMs that were significantly different on initial analysis. All analysis was done on R version 4.2.1.
Results
Demographic Information.

an (%); Mean (SD).
Surgical Variables and Disposition.

an (%); Mean (SD).
Bivariate Analysis of Hospital Outcomes.

an (%); Mean (SD).
bPearson's Chi-squared test; Kruskal-Wallis rank sum test; Fisher's exact test.
cFalse discovery rate correction for multiple testing.
Multivariate Regression Analyses for ED Visit Within 30 days.

aOR = Odds Ratio, CI = Confidence Interval.
bFalse discovery rate correction for multiple testing.
Null deviance = 1198; Null df = 6353; Log-likelihood = -593; AIC = 1198; BIC = 1239; Deviance = 1186; Residual df = 6348; No. Obs. = 6354.
Multivariate Regression Analyses for Readmission Within 90 days.
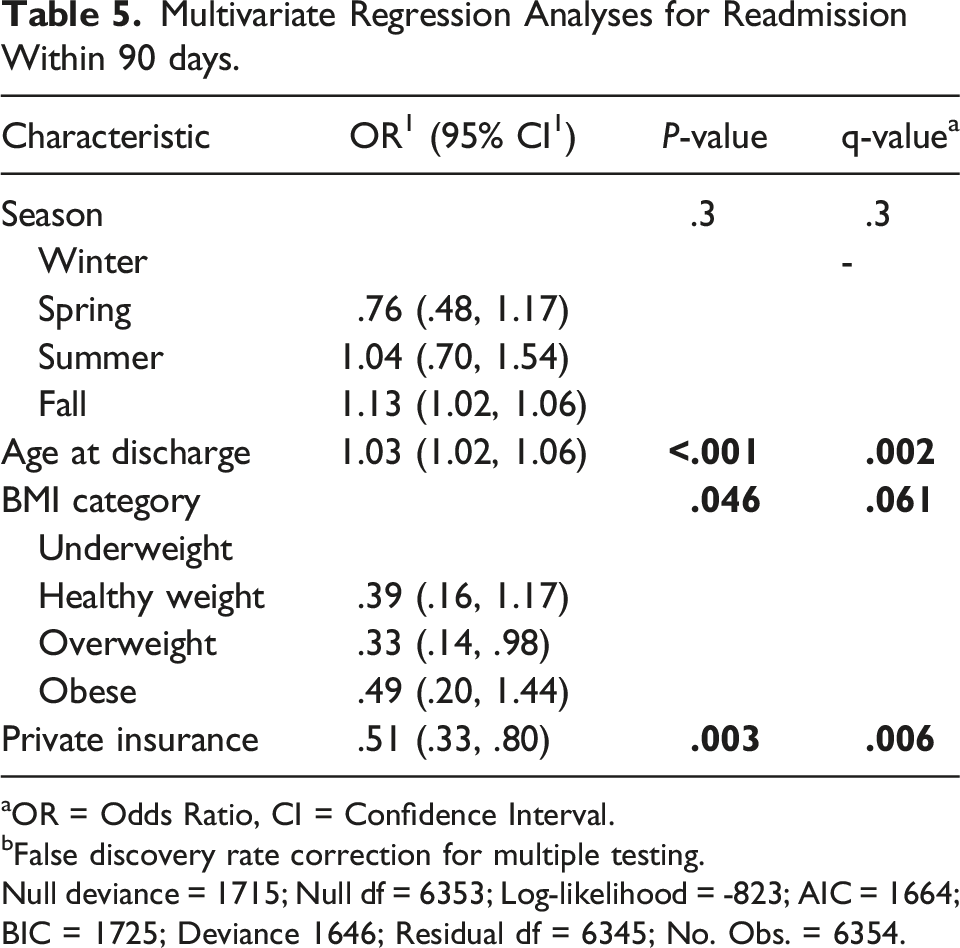
aOR = Odds Ratio, CI = Confidence Interval.
bFalse discovery rate correction for multiple testing.
Null deviance = 1715; Null df = 6353; Log-likelihood = -823; AIC = 1664; BIC = 1725; Deviance 1646; Residual df = 6345; No. Obs. = 6354.
PROMS are reported from preoperative to 1 year postoperatively (Table 4). With this analysis, there were no values identified that demonstrated a statistically significant difference across season, nor met minimal clinical significant difference. Only preoperative UCLA score varied (q < .001). Patient-reported outcome measures of function and satisfaction were equivalent across season of index surgery and time.
Discussion
Demographics and Outcomes
Overall, demographic characteristics, as well as surgical and hospital variables, remained remarkably consistent across season of index surgery. The homogeneity amongst the seasonal groups in most categories supports conclusions that findings by season are not due to otherwise unaccounted-for differences between the groups. There were few statistically significant differences in demographic data observed, including variation in rate of cementation and percentage of female patients by season. Some surgical and hospital variables showed statistically significant differences, including percentage undergoing surgery under general anesthesia, anesthesia time, procedure duration, and room duration, although these are likely not clinically significant. None of the postoperative variables measured were significantly different across season: differences in incidence of complication and readmission within 90 days (among other variables) were not statistically significant. Although it is possible that some patients may have sought care at facilities other than our institution, we feel that early readmission would be directed to the surgeon that performed the original surgery. Additionally, most hospitals within our geographic area are operated under the same health care system and utilize the same electronic medical record, and admissions are referred back to the providing surgeon at our institution, the largest hospital and only Level 1 trauma center in the region.
In contrast to prior work, which implicates both summer and winter as seasons with increased incidence of prosthetic joint infection and complications,25,26 we did not observe differences in incidence of surgical site complication within 30 days nor joint or wound infection within 90 days by season, Due to the rarity of these complications, our study may be underpowered to detect a statistical difference. It is possible that each season confers specific risks and protective factors. Several studies have identified increased temperature as a risk factor for infection following TJA, with hay fever and associated allergies higher during summer months. 27 Winter months in areas experiencing colder ambient air temperatures are associated with increased eczema flares 28 and upper respiratory infections. 29 While environmental factors may increase risk during winter. Aghdassi et al showed that patients undergoing surgery on days with temperature over 20°C had increased risks of surgical site infection compared to those less than 5°C. 30 Furthermore, Fortaleza et al showed an increased risk of 1.3% of SSI for every increase of 1° in average temperature on the day of surgery. 31 Increased temperature during the summer months improves microbe survivorship, which may underly an increased risk for infection. 22 Thus, patients with increased infection risk may consider undergoing THA at a cooler time of year. Conversely, during winter months, patients generally have less sun exposure. This may increase the risk of vitamin D deficiency, which is associated with complications following TJA and occurs at higher prevalence in people undergoing revision arthroplasty. 32 Thus, there is evidence that THA recovery may be impacted in the summer by warmer weather and elevated infection risk, and in the winter by increased in risk for complications. At our institution located in northern New England, with average January temperatures ranging from 13-31 F and average July temperatures ranging from 59-79 F, we did not observe an increased incidence of infection or any complication during the summer or winter months. 33
There has been concern that the increases in infection and complications observed during the summer months are due to the presence of inexperienced trainees—new residents and fellows joining the care team— however this has not been widely supported by the literature.2-4 At our tertiary care institution without an orthopedic training program, patients underwent THA by fellowship-trained attending surgeons without the involvement of trainees. Khanna et al 26 found an increased rate of complications in summer months in teaching and non-teaching hospitals alike. Thus, the trend in our data may support the finding that increased incidence of infections in the summer—when observed— are not driven by trainee involvement but may be the result of a seasonal or temperature effect.
Our data demonstrated no statistical differences in discharge disposition between seasons. In our institution’s northern geographic location, it would be reasonable to consider that it may be more difficult for patients to return home during the winter months, where it can be challenging to perform activities of daily living due to the cold temperatures, ice and snow. However, the finding that patients largely return home (92%–93% on average by season discharged to home/self-care or with home health services) provides evidence for the success of THA, as well as good patient selection of patients who are able to have a successful recovery. Zalikha et al 9 found shorter length of stay and a greater proportion of patients returning home when undergoing arthroplasty in December. They hypothesized that the cultural significance of December holidays may impact discharge disposition planning, and the presence of family support may allow for more rapid return home. Our data showed that patients undergoing THA during summer did have the lowest percentage going to skilled rehab, although by a very small percentage. From this data, patients could be counseled that they have a similar chance to return home postoperatively regardless of season of undergoing THA.
Patient Reported Outcome Measures
Patient reported outcome measures remained mostly equivalent amongst seasonal groups; postoperatively, there were no statistically significant differences in scores of function or satisfaction. Increased rates of depression and Seasonal Affective Disorder may occur during the winter,19,20 which increases complications and decreases satisfaction among TJA patients. 21 A sedentary lifestyle during the winter may adversely impact recovery.17,18 There is evidence that older patients have decreased activity in the winter34,35 which may impact patient recovery to higher levels of activity. Pervasive differences were not observed, but it still may be beneficial to counsel patients that their activity levels may be lower undergoing THA in the winter or spring compared to the summer or fall. With the importance of rehabilitation for TKA, 36 these differences may be increased within that population compared to THA patients. Furthermore, it may be appropriate to have patients who are at higher risk of poor short-term recovery elect to undergo surgery during the warmer months. This data indicates while there may be some differences in recovery, seasonality does not impact patient-reported outcomes measured up to 1 year.
Limitations
There are several notable limitations to this study. With patient-reported outcome surveys, there is potential for incomplete data and bias. Nevertheless, previous studies have found non-responders have similar responses in TJA PROMs. 37 The patients with missing data were excluded from regression analyses, resulting in loss of information due to incompleteness. Additionally, the population encapsulated in our study was racially and ethnically homogenous, limiting generalizability to areas where there is more diversity. While we have categorized based on meteorological seasons, weather patterns may be variable from year to year, altering conditions that patients may face. Reassuringly, average temperatures across years at our institution’s location remained stable with relatively little fluctuation, indicating consistency in the experience of winter, spring, summer, and fall seasons across the years observed; year of surgery was also accounted for in multivariable analysis. 33 Data from only 3 surgeons at 1 center was analyzed in this study, further limiting generalizability.
Conclusion
When evaluating demographics, surgical, and hospital variables, characteristics were similar regardless of season of index surgery. Statistically significant variation in complications were not observed. In evaluation of PROMs, no differences in PROMs measured up to 1 year were found between the 4 seasons in a patient population undergoing THA during 4 distinct seasons. From this data, patients could be counseled that they have similar rates of complications and postoperative recovery regardless of season.
Supplemental Material
Supplemental Material - The Association of Season of Surgery and Patient Reported Outcomes following Total Hip Arthroplasty
Supplemental Material for The Association of Season of Surgery and Patient Reported Outcomes following Total Hip Arthroplasty by Andrew D. Lachance, Catherine Call, Zachary Radford, Henry Stoddard, Callahan Sturgeon, George Babikian, Adam Rana, and Brian J. McGrory in Progress in Physical Geography
Footnotes
Author’s Note
All authors qualify for authorship as per ICMJE guidelines. All authors approve of this submission. We thank the reviewers for the consideration of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.