
Abstract
Purpose:
Many musculoskeletal disorders are associated with over-pronated foot and decreased medial longitudinal arch (MLA) height. Foot intrinsic muscles and plantar fascia (PF) are the primary structures that support MLA. An important reason for the over-pronated foot and the reduction in the MLA height may be the morphological characteristics of the foot intrinsic muscles and PF as well as changes in their mechanical properties. The aim of the present study is to investigate the morphologic structure and mechanical properties of PF, flexor hallucis brevis (FHB), flexor digitorum brevis (FDB), and abductor hallucis (AbH) muscles in individuals with flat foot and to compare the results with those of healthy individuals.
Methods:
The study included 80 participants, 40 with flat foot and 40 with normal foot posture. The foot posture of the participants was assessed using the Foot Posture Index. PF, FHB, FDB, and AbH thickness and stiffness were measured with an ultrasonography device using a linear ultrasonography probe.
Results:
Individuals with flat foot had higher AbH thickness compared to individuals with normal foot posture (p < 0.001), whereas both groups were similar in terms of PF (p = 0.188), FHB (p = 0.627), and FDB (p = 0.212) thickness. Stiffness values of the assessed tissues were similar in both groups (p > 0.05).
Conclusion:
AbH thickness was higher in individuals with flat foot; however, PF, FHB, and FDB thickness were similar in both groups. In addition, our results suggest that foot posture is not related to the stiffness of the assessed tissues.
Introduction
The foot is rigid to support body weight, dynamic to provide gait function, and flexible to adapt to the environment. The foot is stable in foot-strike and push-off phases of gait. In the mid-support phase, the foot must become a mobile adapter to reduce loads. In the mid-support phase, the mobile adaptation of the foot is achieved by controlled foot pronation, which occurs with movements of the subtalar eversion, ankle dorsiflexion, and forefoot abduction. 1 Clinically, over-pronated foot is defined as reduced medial longitudinal arch (MLA) height, everted rearfoot, and dorsiflexed and abducted forefoot in static standing. 2 Over-pronated foot, decrease in MLA height, or flat foot are associated with many musculoskeletal disorders, such as Achilles tendinopathy, plantar fasciitis, tibial tendon dysfunction, patellofemoral disorders, and back pain. 3 –6
MLA is considered to be predominantly supported by passive structures such as plantar fascia (PF) and plantar ligament 7,8 ; however, local dynamic support is provided by contraction of the intrinsic foot muscles and indirectly the extrinsic foot muscles. 9,10 It is believed that the primary task of the intrinsic foot muscles with small moment arms and small cross-sectional areas is to stabilize the foot arches. 9 However, the relationship of changes in structure and function of the foot intrinsic muscles and PF with decrease in MLA height or flat foot is not completely known. These structures cannot be assessed dynamically because of their small size and limited accessibility, 11 but ultrasonography and magnetic resonance imaging can reliably assess their morphological structures (thickness and cross-sectional area). 12 –14 Magnetic resonance imaging is more reliable and valid in assessing muscle thickness compared to ultrasonography, but ultrasonography enables the measurement of the thickness of muscle to be done easily, economically, and quickly compared to magnetic resonance imaging. 13 –16 The morphological characteristics of these muscles can provide important information about muscle function such as muscle strength. 17 In addition, mechanical properties such as stiffness of these soft tissues can be assessed by shear wave elastography, which is reported to be valid and reliable as a new imaging method based on ultrasonography. 18,19 Changes in the stiffness of the foot soft tissue may be an important factor causing decreased MLA height, flat foot, and over-pronated feet, because soft tissue stiffness (muscle, tendon, or ligament) is an important parameter for the regulation of human motion and control as well as for joint stability. 20 –22
In theory, decrease in thickness and stiffness of foot muscle could decrease resisting capacity against external loading and this could cause flat foot or a decrease MLA height. In the literature, there exist a few studies on the morphological features of foot muscles and PF in individuals with flat foot. The results of these studies vary widely. One of these studies 23 reported an increase in foot intrinsic muscle thickness; however, the other 24 reported a decrease in foot intrinsic muscles and PF thickness. Even though a few studies in the literature investigate the intrinsic foot muscles and PF thickness in individuals with flat foot, to the best of our knowledge, there exists no study investigating the stiffness of intrinsic foot muscles and PF in individuals with flat foot. Identifying possible changes in intrinsic foot muscles and PF stiffness and thickness in individuals with flat foot may help to better understand the factors causing or resulting flat foot. In addition, determining possible changes in intrinsic foot muscles and PF stiffness and thickness in individuals with flat foot may provide important contributions to the development of new treatment modalities and/or the development of protective/preventive strategies by providing a better understanding of the factors causing or resulting in flat foot. Therefore, the purpose of the present study was to examine the thickness and stiffness of the PF as well as abductor hallucis (AbH), flexor hallucis brevis (FHB), and flexor digitorum brevis (FDB) muscles in individuals with flat foot. We hypothesized that the stiffness and thickness of the PF and AbH, FDB, and FHB muscles would be lower in individuals with flat foot compared with individuals with normal foot posture.
Metarials and methods
Sample size calculation
Because of the lack of reference data about the stiffness of the foot muscles for this type of comparison, sample size and power calculations were determined using the thickness values of the foot muscles reported in previous study. 23 It was estimated that at least 28 individuals for each group had to be included in this study for 80% power with 5% type-I error level to detect a minimum clinically significant difference of 1.0 mm for muscle thickness, when the average value in the control group is 12.0 mm, with a standard deviation of 1.2 mm.
Participants
The present study was carried out in 80 physically sedentary participants (60 females and 20 males) between the ages of 19 and 49. The participants were not interested in any sports and had not performed regular exercises for at least 6 months prior to the study. The foot posture of the participants was assessed using the Foot Posture Index (FPI), which is reported to be a reliable tool for the detection of different foot types. 25 Based on the FPI scores, 40 individuals (30 females and 10 males) were detected as having a normal foot posture, with an FPI score of 0 to +5, and 40 individuals (30 females and 10 males) as having flat foot, with a score larger than +6. Individuals were excluded from the study if they met any of the following exclusion criteria: (1) ankle or foot orthopedic injuries, such as plantar fasciitis, ligament injuries tendinopathy, bursitis, or ligament injuries; (2) a history of lower extremities surgery or major trauma; (3) rheumatic diseases, such as gout, rheumatoid arthritis, or osteoarthritis involving joints in the lower extremities; and (4) a systemic disease, such as diabetes and/or connective tissue disorders. Ethics approval was obtained from the Non-Invasive Clinical Research Ethics Board of the Faculty of Medicine and written consent was obtained from each participant.
Ultrasonic examinations
Ultrasonic examinations in the selected soft tissues of the foot were performed using an ultrasonography device (ACUSON S3000 Ultrasound System; Siemens Medical Solution, Mountain View, California, USA) equipped with a linear (9L4, 4–9 MHz) probe. Stiffness and thickness measurements of the PF, FHB, and FDB were performed as the participants in the prone position with neutral ankle position and 90° of knee flexion. The AbH stiffness and thickness measurements were performed when the subjects were in the side-lying position and the ankle was in the neutral position, so that the ultrasound probe had the best contact with the skin and with minimal pressure on the tissue. Stiffness measurements of the PF were performed at the region between the calcaneal insertion of the plantar aponeurosis and 10 mm distal to the calcaneal insertion of the plantar aponeurosis. The origin of the PF on the medial tubercle of the calcaneus was used for PF thickness measurements. For the stiffness and thickness measurements of AbH, FHB, and FDB, the probe placed along the direction of the muscle fiber (Figure 1). To avoid deformation on the assessed soft tissue that may increase the stiffness measurements and decrease thickness measurements, minimum pressure was applied on the probe to obtain a sufficient image quality and shear wave signals. For stiffness measurements, shear wave velocity of the assessed soft tissues was calculated using a customized software program (Virtual Touch Imaging and Quantification; Siemens Medical Solution). The thickness and stiffness of the selected tissues were calculated by taking the average of three successive measurements performed.
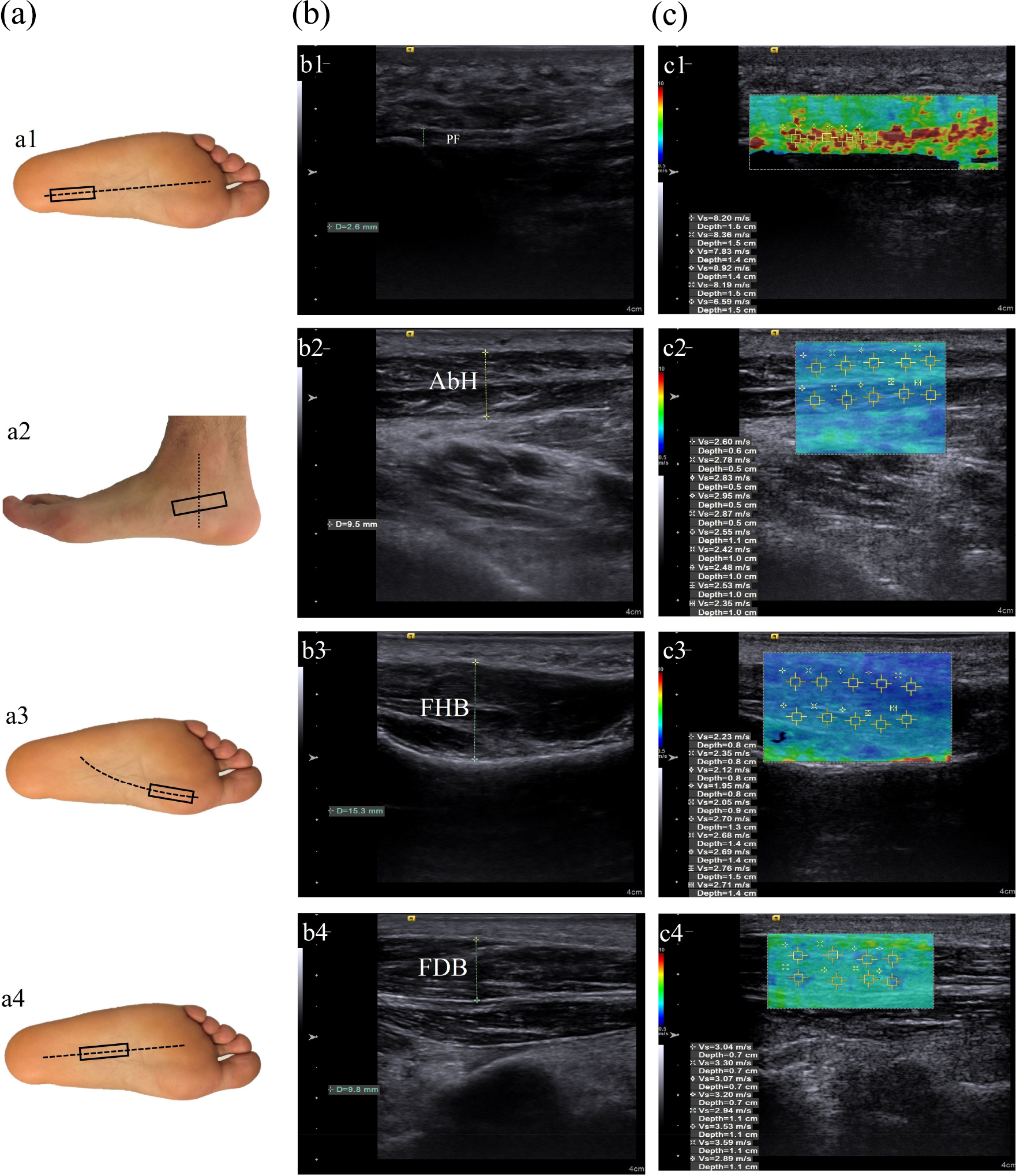
Probe location and ultrasound imaging measurements. (a) Probe position of the PF (a1), AbH (a2), FHB (a3), and FDB (a4) at ultrasonic measurements; (b) two-dimensional ultrasound image of the PF (b1), AbH (b2), FHB (b3), and FDB (b4) at thickness measurements; and (c) color map images of the PF (c1), AbH (c2), FHB (c3), and FDB (c4) at stiffness measurements. Regions of interest were placed, and corresponding shear wave velocity (m/s) was recorded. Red-coded areas represent the highest stiffness, blue-coded areas represent the lowest stiffness, and green-coded areas represent intermediate stiffness. PF: plantar fascia; AbH: abductor hallucis; FHB: flexor hallucis brevis; FDB: flexor digitorum brevis.
Statistical analysis
Statistical analyses were performed using a statistics software program (SPSS, Inc, an IBM Company, Chicago, Illinois, USA). The variables were investigated using visual (histograms, probability plots) and analytical methods (Kolmogorov–Smirnov/Shapiro–Wilk’s test) to determine whether they were normally distributed. Demographic data and the assessed parameters were presented using medians and interquartile range for nonnormally distributed variables. Since the stiffness and thickness of the selected soft tissues were nonnormally distributed, the Mann–Whitney U test was used to compare these parameters between the groups. A p-value of less than 0.05 was considered to show a statistically significant result.
Results
Both groups were similar in age (p = 0.427), body mass (p = 0.244), body mass index (p = 0.346), and height (p = 0.276). Individuals with flat foot had higher AbH thickness compared to individuals with normal foot posture (p < 0.001), whereas both groups had similar PF (p = 0.188), FHB (p = 0.627), and FDB (p = 0.212) thickness. The stiffness of PF (p = 0.310), AbH (p = 0.327), FHB (p = 0.377), and FDB (p = 0.857) was similar in both groups (Table 1).
Median (interquartile range) value for each parameter measured.
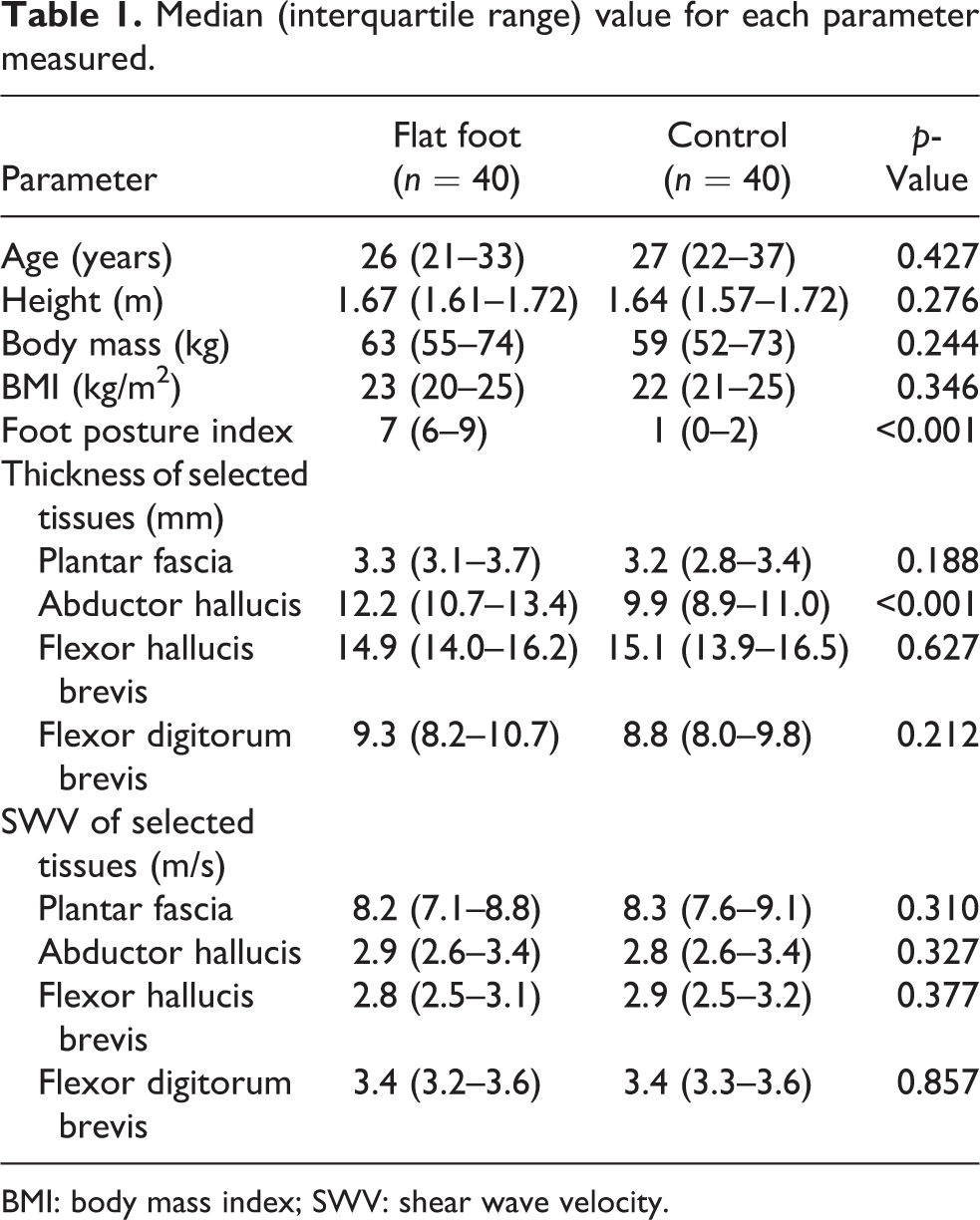
BMI: body mass index; SWV: shear wave velocity.
Discussion
The purpose of the present study was to investigate the changes in morphologic features and mechanical properties of intrinsic foot muscles and PF in individuals with flat foot. We hypothesized that the thickness of PF and intrinsic foot muscles would be lower in individuals with flat foot. Contrary to our hypothesis, we found that the AbH thickness was higher in individuals with flat foot. In addition, the thickness of PF, FDB, and FHB were similar in individuals with and without flat foot. Similar to our results, Zhang et al. 23 reported that individuals with flat foot had higher AbH thickness; however, the thickness of the FHB and FDB muscles was similar in individuals with and without flat foot. Contrary to our results, Angin et al. 24 found that the thickness of AbH and FHB was lower in individuals with flat foot compared to individuals with normal foot posture; however, similar to our results, both groups had similar calcaneal portion of the PF and FDB thickness. The increase in the thickness of AbH in individuals with flat foot may relate to its anatomical and functional features different from the other intrinsic foot muscles. AbH is the most medial muscle in the first layer of the intrinsic muscles, and the primary function of AbH is to elevate the MLA of the foot when the hallux is fixed on the ground. 26 In individuals with flat foot, the decrease in MLA height and over-pronated foot may cause an increase in loading on the AbH muscle, which may cause hypertrophy in the AbH muscle. Different from the AbH muscle, PF, FDB, and FHB is located on the plantar surface of the foot and it resists loading with the other soft tissues of the foot (abductor digiti minimi, quadratus plantae, lumbricals, extensor digitorum brevis, plantar interossei, etc.) against external loading. 9 On the other hand, flat foot may be related to failure in sensory–motor interaction of the foot intrinsic muscle, but not to muscle morphology or strength. Intrinsic foot muscles have small cross-sectional areas and moment arms. Therefore, intrinsic foot muscles do not produce large rotation moments and a considerable force. Alignment and anatomic position of these muscles were thought that they produce immediate sensory information about changes in foot posture via the stretch response. 9 Changes in sensory information, which are assured by foot intrinsic muscles, may be associated with over-pronated foot and decreased MLA height.
Another hypothesis of the present study was that the stiffness of PF, AbH, FHB, and FDB would decrease in individuals with flat foot compared to individuals with normal foot posture. This hypothesis was established based on the idea that soft tissue stiffness is an important parameter for joint stability. 20,21 We expect that a decrease in selected soft tissue stiffness of individuals with flat foot would cause a decrease in MLA height because the decrease in soft tissue stiffness could cause a decrease in resisting capacity against external loading. 27,28 Contrary to our hypothesis, our results suggest that stiffness of PF, AbH, FHB, and FDB do not affect the foot posture. In different orthopedic conditions such as plantar fasciitis, plantar heel pain, or Achilles tendinopathy, changes in soft tissues stiffness were reported by some studies. 29 –31 In these studies, changes of soft tissue stiffness were considered to be related to inflammatory processes and local tissue damages. Contrary to these pathological conditions, flat foot is a long-term and continuous process. Maintaining the soft tissue stiffness might be the best strategy to protect this tissue because changes in the stiffness of the soft tissue can cause an increase in loading and local tissue damage. 32 –34
This study has a few limitations. Firstly, thickness and stiffness measurements were not performed by a researcher blinded to the groups. However, standardized instructions used in thickness and stiffness measurements to minimize the bias. Secondly, stiffness and thickness measurements were performed only on the longitudinal plane. Involving the transverse plane cross-sectional area and stiffness measurements could have been useful in having insight into the pathomechanic of the flat foot. Secondly, the study included only young or middle-age sedentary individuals. In different populations (geriatric, athletes, etc.), effects of flat foot might be different on selected tissues stiffness and thickness. In the present study, foot muscles and PF stiffness and thickness measurements were carried out in resting condition. Investigation of changes in foot intrinsic muscles and PF stiffness and thickness in standing posture or during various functional activities such as walking may provide further insight into flat feet and the factors causing flat feet. Finally, in the present study, changes in morphological and mechanical properties of foot intrinsic muscles and PF in individuals with flat feet were evaluated in comparison with healthy individuals. Further studies are necessary to improve knowledge about changes in intrinsic foot muscles and PF in patients with different various severity levels of flat foot that may have more clinical implications to the management of flat foot.
Conclusion
In conclusion, we found that in individuals with flat foot, the AbH thickness was higher compared to that of individuals with normal foot posture; however, PF, FHB, and FDB thickness were similar in individuals with and without flat foot. In addition, our results suggest that foot posture is not related to the stiffness of the assessed tissues.
Footnotes
Authors’ note
The manuscript or portions thereof are not under consideration by another journal or electronic publication and have not been previously published. Each author participated sufficiently on this manuscript and publication is approved by all authors. The authors and authors’ institutions have no conflict of interest.
Author contribution
All authors have made a substantial and equal contribution to the material submitted for publication and have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.