
Abstract
Aims:
This study aims to determine whether giant cell tumor of bone of the foot (GCTB-F) is more aggressive than GCTB at other sites using data from a single institution.
Patients and Methods:
We reviewed all patients with GCTB seen by our Unit from 1993 to 2012. Patients with GCTB-F were compared with all other patients with GCTB in terms of demographics and presentation. This group of GCTB-F was then compared with patients with GCTB of the appendicular skeleton (GCTB-AS) in terms of treatment and oncologic outcome at follow-up of at least 2 years.
Results and conclusion:
There were seven patients with GCTB-F (2.6%), most consulted over 12 months after symptoms. Compared to other GCTB (n = 262), a bigger proportion of patients (28.5%) presented as recurrent lesions. All seven patients were classified as Campanacci III but none had lung metastasis at presentation or on follow-up. Compared to the group of 124 GCTB-AS, no GCTB-F patient received intralesional surgery. The 14% recurrence rate can be explained by contaminated non-intralesional surgery due to the advanced presentation and the technically challenging architecture of the foot. It would seem the aggressive tag of GCTB-F is not due to aggressive biologic behavior but to a combination of delayed presentation, delayed diagnosis, and difficult surgery.
Introduction
Giant cell tumor of bone (GCTB) is a benign aggressive lesion more commonly encountered in the epiphysis and metaphysis of long bones and less commonly seen in the small bones of the hands and feet. As a result, the number of reports describing GCTB of the foot (GCTB-F) is limited. Early studies indicated that GCTB-F behaved in a more aggressive manner when compared to GCTB at other sites. 1,2 Since then, multiple case series have been published, some of which include GCTB of the hand or distal tibia, almost all of which compared data and outcomes with literature or a set of historical controls. 3 –8 There have been no studies comparing GCTB-F with GCTB of the long bones or appendicular skeleton (GCTB-AS) from the same institution. A study done in this manner would have a smaller population but would have the advantage of evaluating patients from the same general community who are treated with similar oncologic principles.
We ask ourselves the question: is GCTB-F more aggressive in terms of presentation, natural course, and oncologic outcome when compared to GCTB of other sites?
In order to answer this question, we (1) reviewed the cases of all patients with GCTB-F treated by the (University of the Philippines - Philippine General Hospital Musculoskeletal Tumor Unit (UP-PGH MuST)) over the past two decades, (2) compared their demographic and presentation profile with all other GCTB treated by the Unit in the same time period, and (3) compared this group of GCTB-F patients with the population of GCTB-AS also from the UP-PGH MuST during the same time period in terms of treatment and the oncologic outcomes of local and systemic recurrence.
Patients and methods
We reviewed data from the UP-PGH MuST tumor registry between the years 1993 and 2012. Included in our study were all patients with histologically confirmed GCTB of the foot (GCTB-F) who completed treatment with the Unit and who were followed up for at least 2 years or until death. The histologic diagnosis was made or verified by a trained musculoskeletal tumor pathologist of the Unit.
We reviewed each patient’s radiographs, histologic slides, inpatient, outpatient, and surgical records, making sure to rule out non-neoplastic conditions such as hyperparathyroidism and infection. We first compared this subset of patients with GCTB-F with all other GCTB patients seen by the Unit over the same period in terms of demographics. We then compared this same group of GCTB-F patients with subgroups of GCTB-AS patients who presented with a similar Campanacci grade and similar treatment (en bloc excisions).
Results
Demographic data
The UP-PGH MuST maintains a database of patients with extremity tumors seen and treated at the UP-PGH MuST. During the period 1993–2012, there were 269 patients with GCTB of all bones, 7 of whom had GCTB-F, giving an incidence of GCTB-F of 2.6%.
Descriptive results of the 7 patients with GCTB-F were compared against the remaining large group of 262 patients with GCTB of all bones (269 minus the 7 GCTB-F; Table 2).
Of the seven cases of GCTB-F, there were four females and three males. Average age was 28.1 years with a range of 18–41 years. There were more patients (2/7 or 28.5%) less than 20 years of age compared to the bigger cohort of GCTB (26/262 or 10%). The most commonly involved bone was the talus (57%) (Figure 2) with one case each involving the cuboid (Figure 1), calcaneus (Figure 3), and the first metatarsal. Two patients presented as recurrent lesions (talus and metatarsal), having received inadequate intralesional treatment previously at other institutions while five patients had no history of previous treatment. Four of these five virgin cases consulted 12 months or more after experiencing their first symptoms (Table 1).

(a) Gross presentation of patient with GCTB-F of the right cuboid (patient 5). (b) Radiograph of right foot (lateral view) showing involvement of the cuboid (patient 5). GCTB-F: giant cell tumor of bone of the foot..

(a) Preoperative radiograph of the left foot (lateral view) showing talar involvement (patient 6). (b) Post-surgery radiograph showing tibiocalcaneal fusion (patient 6).

Radiograph of foot (lateral view) showing involvement of the calcaneus (patient 7).
Description of each of the GCTB-F patients.

GCTB-F: giant cell tumor of bone of the foot.
Comparison of demographic data between GCTB-F and all other GCTB during the same period.
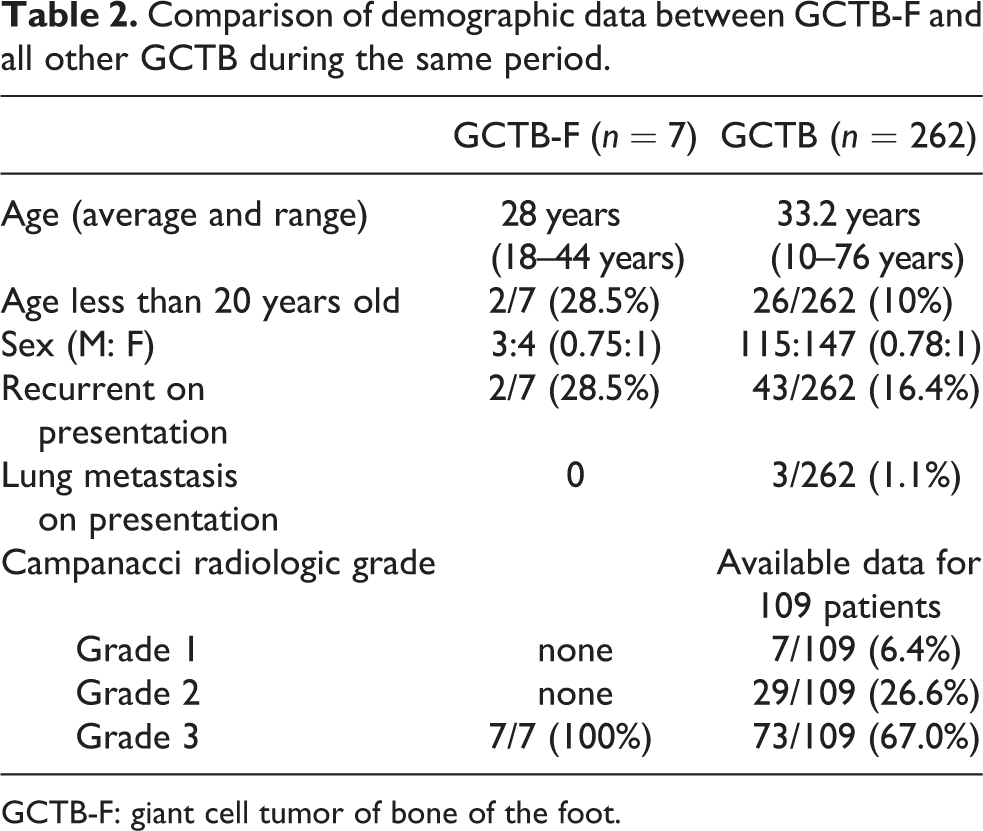
GCTB-F: giant cell tumor of bone of the foot.
In all seven cases, radiographs of the lesions were assessed as Campanacci grade III; having a combination of thinned out, markedly expanded, or destroyed cortices, with tumor bulging into the soft tissue and soft tissue masses neither following the contour of the bone nor limited by a shell of reactive bone. 9 There was involvement of at least 75% or more of the regular bony dimensions in each case. According to the Enneking staging system for benign musculoskeletal neoplasms, the seven cases were all classified as Enneking 3 aggressive lesions based on their clinical course, radiologic features, and histologic findings. 10 None of the patients had local or distant metastasis.
Treatment and outcomes
Of the patients with GCTB-F, all four patients with talar involvement underwent talectomy (marginal surgical margins) with tibiocalcaneal fusion using either autograft or allograft bone. The patient with involvement of the first metatarsal underwent en bloc excision of the metatarsal and reconstruction with metatarsophalangeal fusion using a metatarsal allograft augmented with iliac crest bone graft. 11 Similarly, the patient with cuboid GCTB underwent excision and arthrodesis to surrounding bone with iliac crest bone graft. The patient with a GCTB of the calcaneus underwent a calcanectomy without further reconstruction. None of the 7 GCTB-F patients received denosumab, as none had presented to our Unit before denosumab was included in our treatment protocol.
All surgical margins were classified as marginal; none of the lesions were judged to be appropriate for intralesional curettage. After surgery, all 7 patients were followed up for at least 2 years (range: 2.5–18 years). There was one local recurrence (1/7 or 14%) in a patient who had undergone a piecemeal (vs. en bloc) talectomy. She followed up approximately 11.5 years after her initial surgery with a large, unresectable, local recurrence in the affected foot. We believe this recurrence had occurred much earlier but had been neglected by the patient. She underwent a below knee amputation but eventually died of renal cell carcinoma less than a year afterwards. There were no systemic recurrences from their GCTB-F lesions in all seven patients (Table 3).
Summary of treatment and outcomes for all GCTB-F patients.

GCTB-F: giant cell tumor of bone of the foot; recon: reconstruction; interval to rec (mo.): interval to recurrence in months: systemic rec: systemic recurrence; MTP: metatarsophalangeal.
During the period 1993–2012, there were 124 patients with histologically proven GCTB-AS who fulfilled the same criteria as those of the group of GCTB-F, that is, complete treatment by the Unit and follow-up of at least 2 years or until death. GCTB of the axial skeleton (spine and pelvis), GCTB of the hand, and multicentric GCTB were excluded since they can have different oncologic outcomes compared to those of the AS.
Since all seven GCTB-F patients were classified as Campanacci III lesions and since all seven underwent attempted en bloc excisions, comparisons were also made against similar subsets of patients among the 124 GCTB-AS patients. Of the 124 GCTB-AS patients, 80 were Campanacci III lesions, 4 of whom developed a local recurrence (4.8%) after surgeries which included mostly en bloc excisions or extended curettage. A quarter of these GCTB-AS patients with Campanacci III lesions presented with huge masses requiring amputations. We therefore also compared the GCTB-F patients with those GCTB-AS patients who did not receive amputation (n = 60). On the other hand, 64 patients with GCTB-AS underwent en bloc excisions, 2 of whom developed a local recurrence (4.8%; Table 4).
Comparison of outcome data between the GCTB-F and similar subgroups in the GCTB-AS groups.

GCTB-F: giant cell tumor of bone of foot; GCTB-AS: GCTB of appendicular skeleton.
Discussion
Is there truth to the notion that GCTB of the foot behaves more aggressively than GCTB of the AS? We tried to answer this query by first describing a case series of all GCTB-F patients seen at our Unit over a period of 20 years (1993–2012) and comparing this series against all other patients with GCTB (n = 262) treated by the Unit in the same time period. We then compared clinical treatment and outcomes between our GCTB-F case series and a group of 124 patients with GCTB-AS treated at our institution who were also followed up for 2 years or until death.
Unlike other studies which have analyzed GCTB of the feet and hand (GCTB-H) together as GCTB of the small bones, we concentrated only on GCTB-F because of previous findings that GCTB-H may be a different and biologically more aggressive entity. 8 Surgical techniques may also vary between the two groups as GCTB-F usually occurs in the technically more challenging hindfoot, rarely in the metatarsals while GCTB-H occurs mainly in metacarpals. 1,4,8
Over a 20-year period, there were seven patients with GCTB-F, giving an incidence of 2.6%; well within the range reported in literature 1.2–4%. 5,12 Gender distribution was the same as that of the bigger cohort, 3:4 M: F ratio. In terms of age, the GCTB-F group had two patients just below 20 years of age (28.5%) compared to 10% in the general GCTB population. This finding of more GCTB-F patients in the younger age group has previously been reported although its prognostic significance remains unclear. 7,8
Two of the seven patients presented to our Unit as recurrent lesions after previous inadequate surgery for a 28.5% incidence compared to a 16.3% incidence for the larger cohort. At the same time, all of our GCTB-F patients presented with Campanacci III radiographic lesions. While the higher rate of recurrent lesions and the larger percentage of Campanacci III lesions on presentation might be interpreted as aggressive behavior, they can both be explained by delays in both consult and diagnosis combined likely with inadequacies of a health system in a middle income country such as ours. 13 Young et al., in a review of 57 bone tumors of the hindfoot (23 talus and 34 calcaneus), noted these tumors were often initially misdiagnosed and treated as sprains, arthritis, and various soft tissue injuries. 14 At the same time, the architecture of the bones and joints of the hindfoot provides little room for cortical expansion. Locked in by the surrounding bones, a growing tumor will more readily lyse and break through the cortex of the involved bone, giving a Campanacci III radiographic lesion.
Despite these delays and hindrances to appropriate treatment, however, none of the seven patients with GCTB-F presented with lung metastasis. This is unlike the bigger cohort of 263 patients which had a 1.1% incidence of lung metastasis on presentation.
This seemingly aggressive presentation of GCTB-F patients would preclude the intralesional surgery reserved generally for better contained bone tumors and in turn necessitate an excision of the entire involved bone. Compared to the cohort of GCTB-AS where a third of patients underwent intralesional surgery, none of the GCTB-F patients received intralesional surgery. Despite marginal surgical margins, however, there was one local recurrence. This is likely due to the piecemeal (in contrast to en bloc) excision of the entire talus, resulting in a contaminated marginal excision. This highlights the difficulty of surgery posed by the technically challenging architecture of the hindfoot 4,6 in comparison to the straightforward surgeries (both en bloc excisions and extended curettage) to which the comparison patients with GCTB of the long bones were subjected. Our recurrence rate of 14.3% (1/7) after non-intralesional resection of GCTB-F is approximately the same as the 12.5% reported by Wold et al. from the Mayo Clinic and the 17% reported by Oliveira et al. from a multicenter study led by the Leiden University Medical Center. 1,6
No patient in our series developed regional or systemic recurrence on follow-up; consistent with most studies and consistent also with the observation that lung metastasis is correlated with local recurrence or repeated recurrences rather than radiographic or clinical presentation. 3,4,6 –8,15
In summary, it would seem GCTB-F is not biologically more aggressive. Rather, the aggressive tag is probably due to (1) delayed presentation by patients and delayed recognition by physicians, (2) earlier disruption of cortical borders due to the unique architecture of the foot, (3) the resulting inappropriateness of intralesional surgery and therefore the choice to excise the entire involved bone by non-intralesional margins, usually marginal, (4) contaminated non-intralesional surgery, in this case, piecemeal removal, and (5) a higher incidence of local recurrence due to a higher rate of contamination during surgery.
Treating physicians must therefore remain aware of bone tumors involving the foot, including the entity of GCTB-F in order to provide appropriate and timely management. Principles of treatment remain no different from regular GCTB since it seems the aggressiveness of GCTB-F stems not from an aggressive biology but mainly from delays and difficulties in both recognition and treatment.
Our study has a relatively small sample size. However, this is an inherent limitation of studies about GCTB-F. We have chosen to limit our study to data only from our Institution in order to better compare our GCTB-F patients with the general GCTB and GCTB-AS population. This is the first study that evaluates GCTB-F in this manner.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.