
Abstract
Even though one of the surgical techniques most frequently used to correct external rotation deformity of the shoulder in brachial plexus patients is a humeral derotational osteotomy, few intraoperative parameters has yet been identified to determine the appropriate degree of rotation. We present in this technical note our initial experience using the main elbow flexion skin crease to quantify the correct rotation of the humerus in four young, male patients with upper-type brachial plexus injuries. All patients had a functional elbow and a stable shoulder, but also an external rotation deficit. Via a deltopectoral approach, we used the main elbow flexion crease as an intraoperative surgical parameter to determine the degree of external rotation of the humerus required to achieve a better positioning of the hand in space. After surgery, increased elbow flexion range and enhanced hand-to-face movement was observed, while internal rotation was preserved for performing midline activities. Moreover, all patients exhibited increased active elbow flexion and osteotomy consolidation, with mean elbow flexion increasing from 66.3° to 97.5° pre to postoperatively, and a mean 56.3° of internal rotation correction ultimately achieved. We propose that the main elbow flexion crease is a useful intraoperative parameter to determine the degree of intraoperative external rotation necessary to restore the plane of hand–face movements in upper-type palsies.
Keywords
Introduction
Upper brachial plexus palsies (both C5–C6 and C5–C7 injuries) are characterized by palsy involving shoulder abduction and external rotation, and elbow flexion (which variably influence extension of the elbow, wrist, and fingers when C7 is injured). Such palsies can be caused by birth trauma (obstetric brachial plexus palsy (OBPP)) or by direct brachial plexus injury (BPI), the latter often associated with motorcycle accidents. These palsies are associated with concomitant internal rotation of the upper limb. Although the general results of primary surgery on the brachial plexus (with either grafts or nerve transfers) are very good, recovery of external rotation of the shoulder is poor in some cases, especially where a lack of donor nerves is present. 1 Therefore, in such cases, the recovery of elbow flexion, although acceptable in terms of strength, often is associated with limited functionality of the upper limb. This is largely because forearm motion is obstructed by the abdomen, thereby impeding full flexion of the elbow. Many tasks of daily living in the hand–face plane are limited in this scenario.
For many surgeons, a derotational osteotomy of the humerus is the procedure of choice after a primary nerve reconstruction, as they seek to restore external rotation and improve use of a previously paralyzed upper limb. 2
Since the intraoperative parameters needed to determine the degrees of rotation that must be corrected in upper-type palsies have not yet been clearly defined, 3 –6 we propose using a readily identified and anatomically consistent landmark to determine, during any humeral osteotomy procedure, the degrees of external rotation necessary to ensure the restoration of upper-limb function otherwise limited by the internal rotation palsy.
Objectives
The purpose of this article is to summarize our initial experience with humeral osteotomies fixed with a limited contact-dynamic compression plate (LC-DCP), using the main elbow flexion crease to determine the degree of external rotation required to ensure adequate placement of the hand in space, in patients with an upper-type BPI, recovered elbow flexion, and a stable shoulder.
Patients and methods
Ours was a retrospective evaluation of a series of four patients with brachial plexus injuries who, whether after microsurgical reconstruction or not, exhibited a persistent external rotation defect. All underwent a derotational osteotomy of the humeral bone in the affected limb.
Two patients had sustained their BPI during a motorcycle accident, while the other two had neonatal BPI. The same surgical team performed all procedures, and the minimum follow-up period was 1 year. The degree of humeral external rotation necessary was estimated intraoperatively by pointing the main elbow flexion crease of the elbow directly toward the ceiling.
The postoperative clinical assessment consisted of measuring the range of elbow flexion, and range of rotation, using a goniometer, 4 weeks after surgery, and thereafter every 3 months until the minimum follow-up period of 1 year had passed. Prior to data collection, written informed consent was obtained for each patient, and the study was performed in full accordance with the Declaration of Helsinki II.
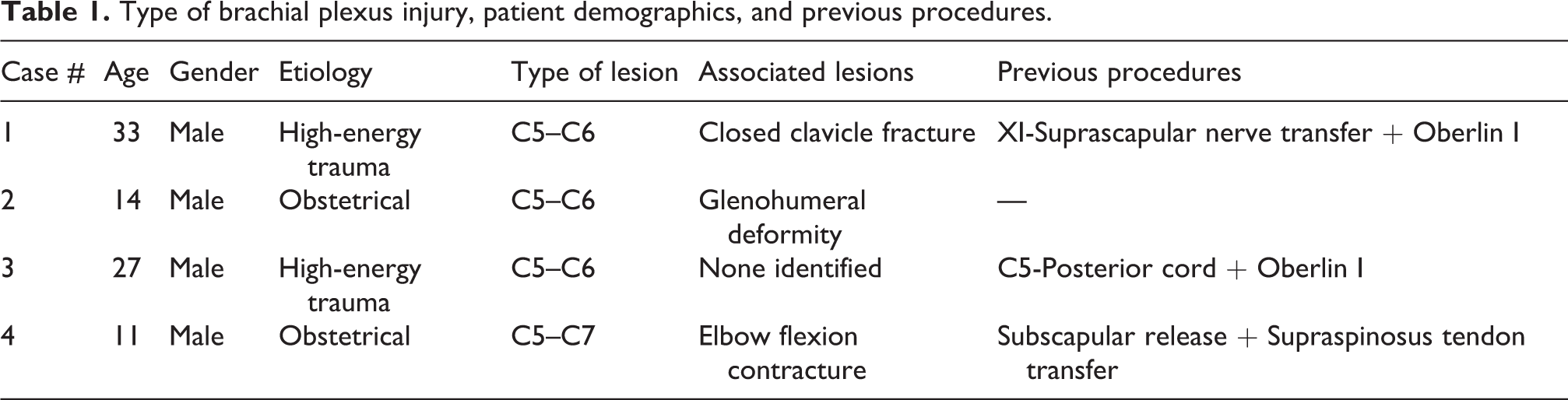
Table 1 summarizes the type of BPI, patient demographic data, and previous procedures performed.
Type of brachial plexus injury, patient demographics, and previous procedures.
Surgical technique
Under general anesthesia with the patient in flat position, the affected limb was positioned on an auxiliary table keeping the shoulder abducted 25°. A classical deltopectoral approach was utilized, creating a 7–10 cm incision that allowed us to separate the deltoid from the major pectoral muscles and identify the greater tuberosity. The deltoid insertion at the humerus was partially tenotomized, and the humeral shaft exposed without desinserting either the medial (latissimus dorsi and coracobrachialis) or lateral (brachialis) muscles.
The LC-DCP (6–12 holes, 3.5 or 4.5 mm in width, depending on humeral circumference) was affixed with screws to the anterolateral surface of the bone, but only at the plate’s proximal end (thereby temporarily leaving the distal end unsecured). Next, a plane and transverse osteotomy was performed with an oscillating micro-saw under water irrigation to avoid thermal necrosis of the bone (Figure 1). Once the osteotomy was completed, the distal humeral shaft was externally rotated in a controlled fashion, employing the elbow flexion crease as the landmark with the elbow flexed at 45° to obtain correct alignment; for this, the crease was pointed directly toward the ceiling to achieve proper alignment of the humerus in all three planes (Figure 2). This new position of external rotation was tested and considered satisfactory if the hand was capable of reaching the mouth (Figure 3). The final step consisted of fixing the three distal screws (Figure 4), and examining the alignment radiologically, after which the wound was closed in layers, with no drainage tubes left in place.
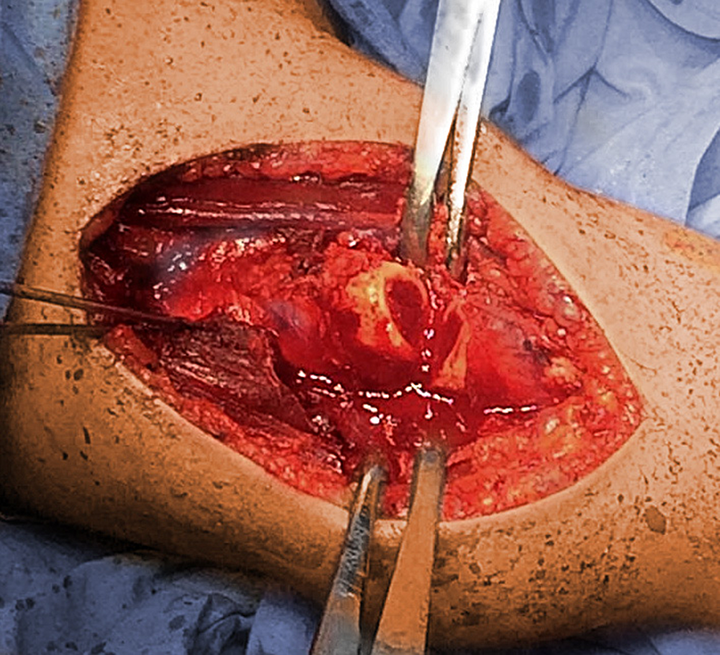
A classical deltopectoral approach was utilized, creating a 7–10 cm incision that allowed us to separate the deltoid from the major pectoral muscles and identify the greater tubercle. Deltoid insertion at the humeral bone was partially tenotomized, and the humeral shaft exposed without disinserting either the medial (latissimus dorsi and coracobrachialis) or lateral (brachialis) muscles. Next, a plane and transverse osteotomy was performed with an oscillating micro-saw under water irrigation to avoid thermal necrosis of the bone. Note the slight incongruence between both the proximal and the distal bone shafts.

Once the osteotomy was completed, the distal humeral shaft was externally rotated in a controlled fashion, employing the elbow fold as the landmark to obtain correct alignment; for this, the fold was pointed directly toward the ceiling to achieve proper alignment of the humeral bone in all three planes. The assistant’s left thumb is placed at the main elbow flexion skin crease.

This new position was maintained manually by assistants, during which the hand was moved passively to the mouth (hand-to-mouth maneuver) to evaluate the newly achieved alignment, which was considered satisfactory if the hand was capable of reaching the mouth.

The final step consisted of fixing the three distal screws, and examining the alignment radiologically.
After surgery, the limb was placed at forced rest for 48 h, after what passive elbow mobility and intermittent sling use were initiated and continued for 4 weeks. After these first four postoperative weeks, X-rays again were obtained; and, if no problems were noted at the plate or the humeral bone, physical therapy was initiated.
Statistical analysis
The main outcomes of interest were (1) pre to postoperative (final follow-up) change in the degrees of internal rotation at rest; and (2) pre to postoperative change in the degrees of active elbow flexion. These data were analyzed using both paired t-tests and the more conservative, nonparametric Mann–Whitney U test. All inferential analyses were two-tailed, and p ≤ 0.05 was set as the criterion indicating a statistically significant difference.
Results
All four patients were male, and they ranged in age from 11 years to 33 years (Table 2), being the mean age 21.3. All four exhibited consolidation of their osteotomy by 4 weeks after surgery.
Final outcomes for internal rotation and elbow flexion.a

a All values are expressed in degrees.
The degrees of internal rotation decreased in all four patients (Table 2), from a mean 73.8° to a mean 17.5°, a difference that (despite the very small sample size) was statistically significant both on parametric (t = 9.00, df = 3, p = 0.003) and nonparametric (p = 0.029) analysis.
Active elbow flexion also increased in all four patients (range of increase = 20°–40°), and overall from a mean 66.3° prior to surgery, to 97.5° postoperatively, a difference that was significant using the parametric paired t (t = 7.32, df = 3, p = 0.05), but not the more conservative nonparametric, Mann–Whitney U (p = 0.20) test (Figures 5 –8 show tow examples of the aforementioned results).

Patient #1. A 33-year-old male with right traumatic brachial plexus palsy remained after reconstructive nerve surgery with an internal rotation deviation of the limb.

Patient #1, 6 months after a derotational osteotomy. Note the complete correction of the internal deviation.

Patient #2. A 14-year-old male with a right residual brachial plexus birth palsy, showing a severe internal rotation contracture. This patient did not receive a nerve reconstructive surgery earlier in his life.

Patient #2 after a derotational osteotomy. Note the symmetry between both elbows and the adequate correction of the internal deviation.
The mean extent of internal rotation correction achieved during the procedure itself was 71.3° (range: 65°–80°), while the mean extent of actual correction (versus baseline) at final follow-up was 56.3°, a difference of 15.0°; this difference approached statistical significance (p = 0.06). Despite this 15.0° difference, in all four patients, a completely appropriate degree of internal rotation was evident, at final follow-up, for them to perform routine midline functional tasks with their affected hand.
The maximum degrees of abduction and glenohumeral flexion remained unchanged (data not shown). Table 2 summarizes pertinent outcomes for each of the four cases.
With respect to complications, two of the four patients experienced transient paresis of the biceps, from grade 4 to grade 3 on the British Medical Council Motor System Scale. However, by the time of the 4-week evaluation, strength had returned to at least its baseline level in both these patients. No other perioperative or long-term complications were noted.
Discussion
One of the most difficult movements to restore after a BPI is external rotation of the shoulder. This contrasts with shoulder abduction and elbow flexion, which are more easily reconstructed. An imbalance between the internal rotators (mainly the subscapular muscle) and the external rotators (mainly the infraspinatus muscle) has been theorized to cause this. 3
Many secondary procedures have been described to correct this imbalance, among which are tendon transfers, glenohumeral arthrodesis, and humeral derotational osteotomies. The first of these is the first choice at some centers, primarily utilizing the lower trapezius as the donor tendon. 7
Shoulder arthrodesis should be reserved for those adult patients who sustain a traumatic BPI and (1) either undergo no attempts to reinnervate their shoulder abductor muscles or (2) have any such attempt fail. 8,9 Shoulder arthrodesis not only stabilizes the shoulder, it also corrects the imbalance between internal and external rotators, eliminating the need of a humeral osteotomy.
A derotational osteotomy is the preferred choice in patients in whom reinnervation has been achieved to the suprascapular muscle, the deltoid muscle (achieving shoulder stability) or both, and elbow flexion restored, but in whom the lower part of the trapezius has been denervated because the spinal accessory nerve has been used as a donor to restore suprascapular nerve-related functions.
One of the most controversial aspects of this osteotomy procedure is the extent of external rotation to apply. Although the skin is naturally mobile, Itamura et al. 10 described a very stable relation between the main flexion elbow crease and different osseous structures as the medial epicondyle, the lateral epicondyle, the olecranon, and the radial head. This pattern was independent from gender and hand dominancy and is represented in Figure 9.

Graphic representation of the constant relation presents at the main flexion elbow skin crease and the underlying osseous structures. Left: Normal elbow, with the medial epicondyle, lateral epicondyle and olecranon in relation to the elbow crease. Right: In a pathologically internal rotated shoulder, this relation remains constant.
Al-Qattan et al. have used the hand–ear plane as a correction parameter, while performing a distal osteotomy. 11 In a series of 43 pediatric patients with an upper brachial plexus lesion, Waters and Bae 12 performed osteotomies with rotations of the humerus between 35° and 90°, averaging 64°. The results of rotation and flexion that we obtained in our small series are comparable to those results and some others. 4,5
As each brachial plexus palsy patient can present different grades of external rotator paresis, soft tissue retraction, and contraction of the subscapular muscle, the extent of correction needed to recover an acceptable plane for hand-to-face movements will tend to vary between cases. Furthermore, in upper-type brachial plexus palsies, the forearm could present either a supination or a pronation contraction, making the forearm position variable. In adult OBPP patients, the presence of a dysplastic humeral head greatly limits shoulder movements and can also limit the use of the forearm as an intraoperative parameter to determine the grade of external rotation that should be achieved. By contrast, the main elbow flexion crease was in our short experience a constant parameter that can be easily used, because it has constant relations to the underlying bone structures. 10,13 Figure 10 graphically represents the independence of the osseous elbow structures from the humeral head when performing this technique.

A: Humeral head and biceps tendon (the latter in yellow) viewed from above. B: Elbow osseous structures viewed from below. (c) Schematic representation of the structures observed in A and B in relation to the whole humeral bone. D: Schematic drawing of both the humeral head and the distal osseous elbow structures observed in A and B, but this time superimposed, in a normal patient on both sides. Note the biceps tendon in yellow. E: Normal limb on the left, and internally rotated limb on the right. F: After a surgical external rotation correction of the humeral bone by a proximal osteotomy, the humeral head keeps pointing internally, while the elbow osseous structures now point normally.
It is for this reason that we propose adopting an anatomically consistent intraoperative landmark to determine the exact degrees of external rotation each patient needs.
One important condition essential to any derotational osteotomy of the humeral bone is that the patient has a stable shoulder, thereby anchoring the upper limb. Such shoulder stability can be restored either via nerve repair or shoulder arthrodesis, both approaches capable of yielding satisfactory shoulder stability. 9
One advantage of the deltopectoral approach to derotational osteotomies is that it avoids the risk of damaging the nerve transferred (e.g. the Oberlin transfer) that exists if the more cosmetically pleasing internal arm approach is used. On the other hand, a disadvantage of the deltopectoral approach is that it leaves a more visible scar. Abzug et al. 14 also employ the deltopectoral approach, but does not perform a partial deltoid tenotomy. In our hands, we have found this technique useful, because it more readily exposes the humeral shaft and allows us to clinically evaluate the limb’s new alignment, while directly viewing the various humeral structures, and to thereby adjust that alignment to best meet each individual patient’s needs.
With respect to the location at which to perform the osteotomy, we select a point between the pectoralis major and deltoid muscle insertions, unlike the location described by Rühmann et al., 6 who has elected to perform mid-shaft osteotomies, albeit with a greater risk of both nonunion—between 15% and 25% 15,16 —and radial nerve injury. Meanwhile, in children, Al-Zahrani 17 achieved slight improvement in shoulder abduction if the osteotomy was performed proximal versus distal to the deltoid insertion. We performed our osteotomy, as described herein, more distally, so we did not identify any altered range of abduction in our patients.
We admit, however, that one of the major drawbacks of the technique described in this article is that the number of published cases remains very small; as such, numerous further cases are required to draw any confident conclusions.
Conclusions
Based upon this short series of cases, we propose that the main elbow flexion crease can be used as a reliable and readily identified intraoperative parameter with which to determine the degree of external rotation necessary to restore a satisfactory plane of hand-to-face movement. This approach preserves the midline functions needed to accomplish certain daily tasks, like dressing and feeding oneself. Neither previous nerve reconstructions nor glenohumeral deformities create difficulties for this procedure. Longer series employing this simple intraoperative technique are needed to determine its true clinical utility.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.