
Abstract
The majority of children with obstetric brachial plexus injury show some degree of spontaneous recovery. This review explores the available evidence for the use surgical brachial plexus repair to improve outcome. So far, no randomized trial has been performed to evaluate the usefulness of nerve repair. The evidence level of studies comparing surgical treatment with non-surgical treatment is Level IV at best. The studies on natural history that are used for comparison with surgical series are also, unfortunately, of too low quality. Among experts, however, the general agreement is that nerve reconstruction is indicated when spontaneous recovery is absent or severely delayed at specific time points. A major obstacle in comparing or pooling obstetric brachial plexus injury patient series, either surgical or non-surgical, is the use of many different outcome measures. A requirement for multicentre studies is consensus on how to assess and report outcome, both concerning motor performance and functional evaluation.
Introduction
Around 20–30% of infants with obstetric brachial plexus injury (OBPI) do not show complete spontaneous recovery (Annika et al., 2019; Lagerkvist et al., 2010; Pondaag et al., 2004). Depending on the extent of the neurological deficit 2 weeks after birth, four different lesion groups were described by Narakas: Group 1; C5-C6; Group 2: C5-C6-C7; Group 3: C5-T1 without Horner syndrome; and Group 4: C5-T1 with Horner syndrome (Narakas, 1987). An increasing extent of the nerve lesion, namely a higher Narakas group, correlates negatively with the amount of spontaneous recovery (Al-Qattan et al., 2009). It is widely accepted that if elbow flexion occurs after 2 months of age then recovery will be incomplete, with outcome progressively worsening with later biceps recovery (Gilbert and Tassin, 1984; Lagerkvist et al., 2010; Smith et al., 2004; Strömbeck et al., 2000; Waters, 1999).
In cases of incomplete recovery the shoulder is always impaired, with poorer function in more extensive lesions and with later biceps recovery (Lagerkvist et al., 2010; Smith et al., 2004; Waters, 1999). It is rare for active elbow flexion not to recover spontaneously (Bisinella and Birch, 2003; Chin et al., 2013; Hems et al., 2017). In Narakas Group 3 and 4 cases, wrist and finger extension may fail to recover. Finger flexion is only rarely completely deficient in some Narakas Group 4 cases, but functional grip is usually absent. Longer term deformities include flexion contracture of the elbow and limitation of forearm rotation.
The prognosis for useful hand function recovery in infants with a Group 4 lesion is poor (Al-Qattan et al., 2009; DiTaranto et al., 2004; Narakas, 1987; Sever, 1916). It is generally agreed that the indication for nerve surgery in these children is strong. In children with a Narakas Group 1–3 lesion type the indication for surgical intervention is less clear, but is often considered when spontaneous recovery does not occur or is limited at the age of 3–6 months. There is no consensus among surgeons regarding the selection criteria and timing of surgery, although neurotmetic lesions and root avulsions precluding useful regeneration have been identified during OBPI surgery (Boome and Kaye, 1988; Boyer, 1912; Gilbert and Tassin, 1984). Nerve reconstruction is performed in these instances aiming at a significant improvement of function as compared with what would have recurred spontaneously.
So far, a strong scientific validation of the value of nerve reconstructive surgery, such as might be provided by a randomized trial, is lacking (Malessy et al., 2009). To address the issue, two different approaches can be used: (1) the results of nerve reconstruction can be compared directly with those of non-surgical treatment in the same series and (2) the results of non-surgical series from the literature can be used for comparison with series describing results after nerve reconstruction.
In order to outline the current way of thinking regarding nerve surgery for OBPI, we updated our previous analyses of the literature (Pondaag and Malessy, 2014; Pondaag et al., 2004) and reflect on the difficulties encountered with the comparisons published so far.
Results
Comparing results of nerve reconstruction with those of non-surgical treatment
Summary of papers included.
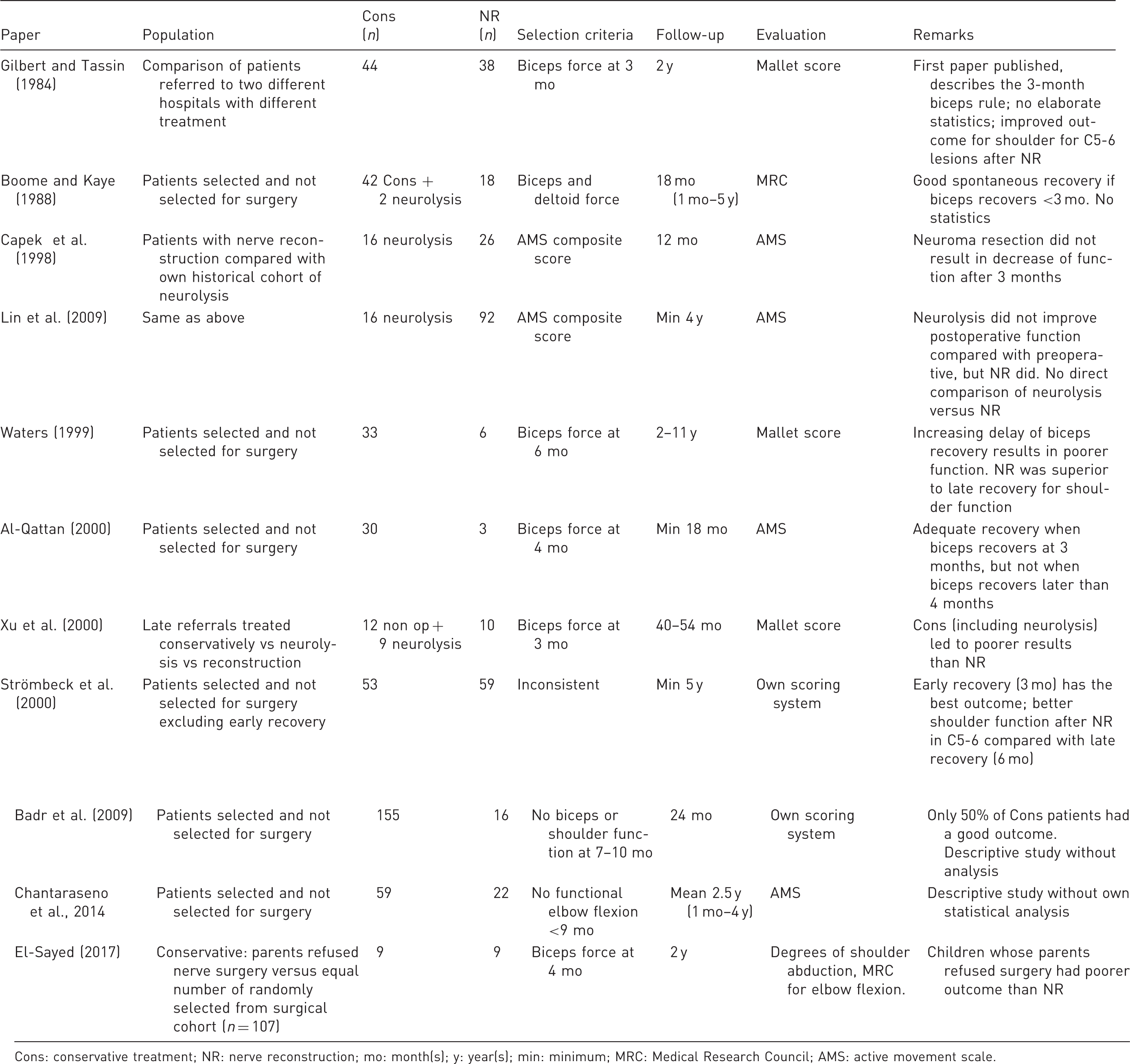
Cons: conservative treatment; NR: nerve reconstruction; mo: month(s); y: year(s); min: minimum; MRC: Medical Research Council; AMS: active movement scale.
The first comparison performed by Gilbert and Tassin (1984) was between a conservatively treated cohort (n = 44) from Hôpital Saint Vincent and a surgically treated cohort (n = 38) from Hôpital Trousseau, in Paris, France. In a subgroup analysis of C5-C6 lesions, 22 surgically treated and 18 conservatively treated patients were compared. In the surgical group, 14/22 patients (63%) reached a Mallet IV shoulder, while recovery in the conservatively treated group occurred to a maximum of Grade III (Mallet, 1972). In the non-surgical group, recovery was incomplete if biceps recovered after age 3 months. This observation led to the conclusion that surgical treatment is indicated if the biceps muscle has not recovered at the age of 3 months.
Clarke et al. (1996) performed a stepwise analysis of the patients of the Toronto Hospital for Sick Children, looking at natural history (Michelow et al., 1994), benefits of neurolysis (Clarke et al., 1996), and outcome of graft repair of conducting neuromas in 26 children (Capek et al., 1998). In 2009, results from a larger patient series with a longer follow-up (>4 years) led the authors to conclude that the eventual recovery after graft repair was better than after neurolysis (Lin et al., 2009). Recovery to Active Movement Scale (AMS) Grade 6 or 7 was statistically more robust in the surgical repair group than in the neurolysis group for shoulder abduction and external rotation, elbow flexion, supination and wrist/thumb extension. The interpretation of the findings of this study is hampered by the fact that a comparison was made between preoperative and postoperative AMS grading within the neurolysis and grafting group. A direct comparison between the end result of neurolysis and grafting was not provided.
Waters (1999) described 39 children who were evaluated before the age of 6 months. In six patients nerve surgery was performed because there was no recovery of the biceps muscle at the age of 6 months. The conservatively treated children were divided into five groups, depending on the month in which the biceps muscle recovered. Four of the five movements of the Mallet score for shoulder function were analysed separately: (1) abduction; (2) external rotation; (3) ability to bring the hand to the mouth; and (4) to the neck. It was concluded that these shoulder functions were better in the group that received nerve surgery at 6 months of age, as compared with non-surgically treated infants in whom the biceps recovered at 5 months. Unfortunately, the statistical method used for comparison of groups was not mentioned. We constructed figures from the patient data in the original paper, to illustrate the authors’ findings and to make the results easier to understand (Figure 1). The authors concluded that when recovery was delayed to 4 or 6 months, the end-stage recovery was incomplete. Nerve surgery after 6 months yielded superior results for the shoulder in children in whom biceps recovery was delayed until the sixth month.
End stage of three components of the Mallet score related to timing of first biceps muscle recovery or after nerve surgery (Waters, 1999). (a) Abduction, (b) external rotation, (c) hand to mouth.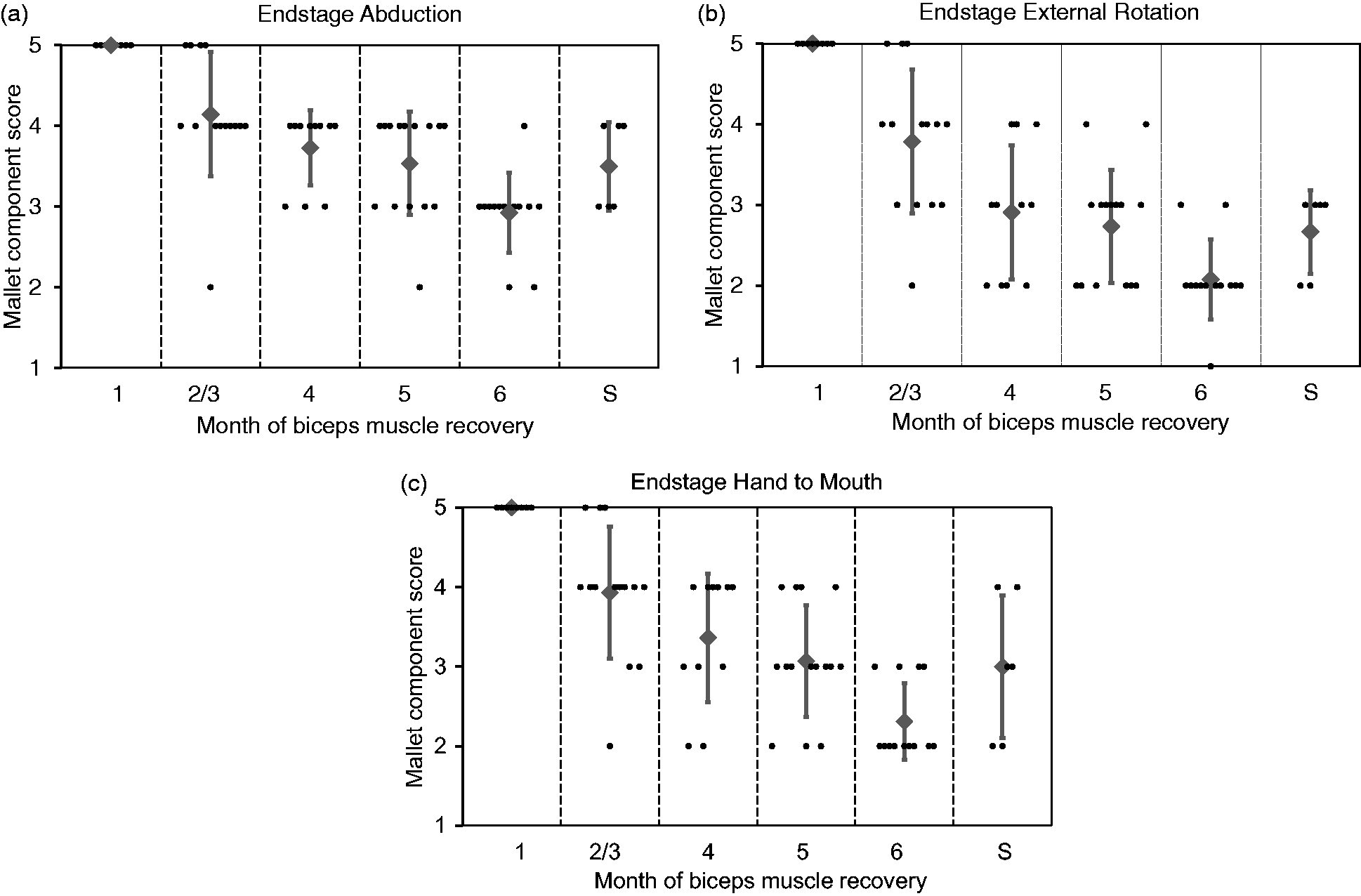
Strömbeck et al. (2000) described infants referred to a national OBPI clinic in Stockholm, Sweden. From a cohort of 470 children, only those with a follow-up of more than 5 years were selected, which left 247 children for analysis (only about half of their cohort). Seven years later a follow-up study was published (Strömbeck et al., 2007). Movements in these 247 children were assessed using a locally designed scoring system resulting in a sum score, which is difficult to interpret. In addition, the tactile sensibility, grip, bimanual activity and hand preference were scored and the pick-up and grip-tests were performed. The children who ‘exhibited some muscle activity in their biceps or deltoid muscles at the first visit at 3 months of age’ were considered as early recovery. Outcome after early recovery was compared with late recovery, and to recovery after nerve reconstruction. In the C5-C6 group, children who were surgically treated had better shoulder function than the non-surgically treated children with a delayed recovery, but not better elbow flexion. In children with a C5-C7 lesion, there was no difference in shoulder or elbow recovery between the late recovery and operated group. Both groups had worse function than the early recovery group. The major limitation in this paper was the inconsistent selection criterion for surgery (or cross-over in the treatment groups), which makes extrapolation to a generalizable rule for the indications for nerve reconstruction impossible.
Our search strategy did not identify one relevant paper, which has come to our attention (El-Sayed, 2017). The outcome of two patient groups with an upper plexus (C5-C6) lesions without biceps recovery at 4 months of age were compared. In one group surgery was proposed, but refused by the parents (n = 9). As a consequence, these patients were treated non-surgically. The other group consisted of nine patients who were randomly selected from the authors cohort of surgically treated children (n = 109). The authors concluded that nerve reconstruction provided superior results compared with conservative management. We feel, however, that the base for this conclusion is insufficient in view of the small numbers and lack of proof that both groups were really comparable in the absence of MRI diagnostics and surgical findings. In the non-surgical group, the authors reported that there was no useful recovery of elbow flexion in any patients, which is substantially different from other studies of the natural history for spontaneous recovery after C5-C6 OBPI.
Comparing outcome of non-surgical series from the literature with those following nerve reconstruction
Another option to investigate the benefits of nerve reconstruction is to compare the outcome in surgical series with the outcome of spontaneous recovery in other series. The main difficulty in this comparison is that there are few natural history series for OBPI that assess and report outcome in a qualitatively good manner. We systematically reviewed the quality of natural history series by applying four quality criteria to 76 papers: prospective study design (not retrospective), population-based series (not selected populations from specific clinics or hospitals), proper follow-up and a well-defined system of outcome. None of the publications met three or four quality criteria (Pondaag et al., 2004). Only seven papers met two quality criteria.
Since 2004, two papers have appeared that described the outcome of a prospective, population-based cohort using a well-documented outcome after sufficient and complete follow-up. Both series originate in Sweden, and have a follow-up of 18 months (Lagerkvist et al., 2010) and 10–12 years (Annika et al., 2019). In these series, however, a small number of children were included who had been surgically treated, thereby confounding the natural history data. The proportion of children with residual impairment was around 20%.
Natural history descriptions could ideally be used as a standard to which results of surgical series could be compared. One approach is to identify those children who were eligible for nerve repair, but were treated non-surgically, and use these non-surgical results as a reference point to surgical outcome. Smith et al. (2004) reported long-term outcome in 28 children who had absent biceps function at 3 months of age (Gilbert’s rule of thumb), 22 of whom did not have nerve repair. All except one with a C5-T1 lesion regained elbow flexion. Although some of these children had good shoulder outcome, many had deficits in shoulder function and had undergone secondary operations.
A difficulty with comparing natural history and surgical series is that the latter harbour referral and inclusion bias. As OBPI is a rare disease, the number of patients in surgical series is generally small and studies may be insufficiently powered.
Surgical series differ in selection criteria, surgical technique and outcome assessment, which hampers summarizing the results. Regardless, it is our experience for shoulder function (n = 86) that true glenohumeral external rotation does not recover after surgery in 40% of children, and only 20% of children can externally rotate beyond 20° (Pondaag et al., 2005). This roughly corresponds with the findings of Clarke’s group (n = 177) (Tse et al., 2011). ‘Good’ shoulder function was achieved in 33% of children in Birch’s series (Birch et al., 2005). Poor recovery of elbow flexion after nerve surgery was occasionally seen in large groups: 5% of 51 children (Terzis and Kokkalis, 2009), 8% of 86 children (Pondaag et al., 2005) and 18% of 100 children (Birch et al., 2005). The main goal of surgery in the most severe lesions, namely useful hand function, was, depending on definition, achieved in 93% (Birch et al., 2005), 75% (Haerle and Gilbert, 2004), 69% (Pondaag and Malessy, 2006), 57% (Maillet and Romana, 2009) and 48% (Kirjavainen et al., 2008).
Discussion
The benefits of nerve repair in OBPI have not been investigated in a randomized fashion, thus the highest level of evidence cannot be reached. To date, the evidence that supports the value of surgical treatment is of low methodological quality. It would, however, be erroneous to conclude that there is no place for surgical treatment: ‘Absence of evidence is not evidence of absence’.
Since the neurological prognosis without treatment is poor in cases of root avulsions and neurotmesis, brachial plexus surgery to improve outcome is justified, provided that it indeed does so. After nerve surgery recovery of shoulder function, elbow flexion and hand function has been obtained (Birch et al., 2005; Haerle and Gilbert, 2004; Lin et al., 2009; Pondaag and Malessy, 2006). For most physicians treating infants with OBPI, a severe lesion (Narakas Groups 3 and 4) with diminished hand function without speedy recovery is a strong indication for nerve reconstruction. This subgroup of patients, however, is only about 15% of patients in hospital-based series.
The most difficult decision making is in Narakas Group 1 and 2 injuries (C5-C6 or C5-C6-C7 lesion) that persists for at least 3 months (Bain et al., 2009). The specific lesion encountered is a neuroma-in-continuity of the superior trunk in which impaired, disorganized axonal regeneration may take place (Chen et al., 2008; van Vliet et al., 2015). Unfortunately, related clinical recovery is variable and unpredictable. Published results of conservatively treated children in various cohorts have frequently not been investigated with imaging to detect the presence of avulsions. Without surgical exploration, the exact type and extent of nerve lesion is not known, making comparison difficult. Cases where exploration and neurolysis only had been carried out have been regarded as the non-repair control group in at least one study (Lin et al., 2009). However, it is not known whether neurolysis has an effect on nerve recovery either beneficial or harmful.
The exact time point to select patients with an upper type lesion for nerve reconstruction cannot be determined with certainty, but is probable somewhere between the third and sixth month (Smith et al., 2004; Waters, 1999). It is important to realize that the start of recovery of the biceps muscle is employed as a proxy for prognostication of the shoulder in upper trunk lesions and not per se a predictor for the end stage of recovery of the biceps muscle itself: ‘The biceps rule is not about the biceps’. With increasing delay of initial recovery, the prospect of a good eventual outcome for the shoulder decreases. The available comparative series (Gilbert and Tassin, 1984; Lin et al., 2009; Strömbeck et al., 2000; Waters, 1999) provide some evidence that shoulder function can be improved by nerve repair.
Especially external rotation of the shoulder recovers poorly, both after conservative treatment as well as after nerve repair (Manske et al., 2019; Waters, 1999). In those infants with otherwise good spontaneous recovery of elbow flexion, it is suggested to improve external rotation by using an accessory to suprascapular nerve transfer in a late stage (van Ouwerkerk et al., 2006). In the recent years, there has been a tendency to perform nerve transfers instead of brachial plexus reconstruction by grafting (O’Grady et al., 2017). Strong advantages of this shift of approach have not been shown (Tse et al., 2015).
An alternative to early nerve repair for OBPI is to await the end stage of natural neurological recovery, and to treat residual deficits with muscle/tendon transfers, rotation osteotomy or joint fusion (Socolovsky et al., 2016).
One of the major obstacles for improvement of treatment of OBPI is that many different outcome measures are used (Chang et al., 2013; Sarac et al., 2015), which disables comparison. Pooling of data to obtain statistical differences in larger series is therefore not possible. Recently, a first step was made to define an internationally accepted set of outcome measures (Pondaag and Malessy, 2018). The most commonly employed outcome measures used so far concern motor function of the shoulder and arm (Chang et al., 2013; Sarac et al., 2015). Only rarely, has the functional outcome, for example, performance of daily activities, been assessed between treatment groups, even though this intuitively seems the most valuable way to measure outcome. In addition, one has to keep in mind that in many OBPI children the affected hand is, or has become, non-dominant (Yang et al., 2005).
In order to be able to push the field forwards, it is imperative that a set of functional outcome measures is agreed upon to assess functional outcome of children with OBPI, as well as consensus on how to measure motor outcome of these children (Pondaag and Malessy, 2018; Squitieri et al., 2013). Such a set of outcome measures should be applied to cohorts of patients that have been treated with different strategies, which could be either conservative versus early nerve surgery, or focus on nerve surgery versus secondary surgery. At first, retrospective analysis of different strategies could be undertaken, as proper functional evaluation can only be performed at a certain age. Depending on the results of such an analysis of prior treatment strategies, patients should be prospectively treated according to the best strategy or treated in a randomized fashion if optimal treatment strategies are still uncertain in given situations.
The support for brachial plexus surgery in OBPI infants is based on low-quality observational studies of patient series in which surgical to conservative therapy are compared. None of the individual studies provides enough scientific proof that nerve reconstruction is superior to conservative treatment. Additionally, pooling of the results is not possible due to different methodology and outcome measurement.
Based on the literature and our own experiences, it is our opinion that for a well-selected group of patients’ nerve surgery is beneficial. Our own clinical paradigm is to advise early surgical exploration in children with Narakas Group 3 and 4 lesions. These children are investigated with MRI to look for nerve root avulsions at the age of 2–3 months, to enable surgery at 3–4 months. Children with Narakas Group 1 and 2 are followed for at least 3 months. The absence of anti-gravity elbow flexion using the biceps muscle at that age remains the main indicator to decide for MRI-analysis and afterwards surgery at the age of 4–6 months, unless late recovery commences and MRI does not show root avulsions.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.