
Abstract
Purpose:
There has been no report to date on any biomechanical study regarding the strength of fixation at the osteotomy site in dome-shaped high tibial osteotomy (HTO). In this study, we evaluated the biomechanical strength of a spacer that we improved and determined the medial site of HTO.
Methods:
HTO correction angles of 15° and 20° were used in all experiments, which were performed on lower leg specimens from pigs (n = 12). The osteotomy site was fixed by a locking plate and screws with a spacer. Compression (600 N/min until 1100 N) and extended cyclic loading (200 cycles at 1000–2000 N) were performed to compare initial displacements in HTO specimens with and without spacers.
Results:
The reduction ratios of displacement with and without spacers at HTO correction angles of 15° and 20° were 37% and 27%, respectively. No effect of the spacer at the correction angle of 15° was observed in the cyclic loading; however, the maximum displacement and amplitude were reduced with the spacer at the correction angle of 20°.
Conclusions and clinical relevance:
When the HTO correction angle is small, the effect of the spacer is uncertain. However, the spacer is effective at an HTO correction angle of 20°.
Introduction
Osteoarthritis of the knee is a pathological condition in which the articular cartilage is damaged, frequently leading to pain in the knee in the elderly due to varus deformity of the knee. High tibial osteotomy (HTO) for osteoarthritis of the knee has the advantage of preserving the articular joint structure and achieving deep flexion of the knee, which is used in various Japanese sitting techniques. Several different fixation methods have been used to date, including plate fixation and external fixators. 1,2 Recently, medial opening-wedge osteotomy has been increasingly performed for moderate varus deformity of the knee, with good results when the appropriate technique has been used. 3 –5
However, few satisfactorily strong and secure methods for moderate-to-severe varus deformity of the knee have yet been developed, and fixation methods must be improved to resolve these issues for the affected patients. 6 Dome-shaped osteotomy 7 –9 is applicable even for patients of large varus deformity and provides a relatively good clinical result; however, to the best of our knowledge, there have been no biomechanical studies regarding the strength of the fixation at the osteotomy site. Therefore, in the present study, we evaluated the biomechanical strength of a spacer that we improved and determined the medial site of the HTO.
The purpose of this study was to evaluate the role of the spacer in dome-shaped HTO with a locking plate under repeated compression loads using pig tibia to establish desirable fixation methods.
Methods
Lower leg specimens from pigs were used for the experiments. The specimens were thawed at room temperature for 24 h before the experiments. The soft tissues were completely removed. The fibula and tibiofibular joints were also removed.
In preparation for the osteotomy, the hole guide was fixed using Kirschner wire at a position 30 mm from the upper end of the tibia on the loading axis. The guide for the osteotomy was made of acrylic plate (Figure 1(a)), with multiple holes of 2.4 mm in the curvature radius of 22.5 mm. The dome-shaped cutting line was achieved by piercing through the Kirschner wire through all holes. Separation of the bone was performed very slowly by soft hammer blows to avoid fracture of the lateral cortex.
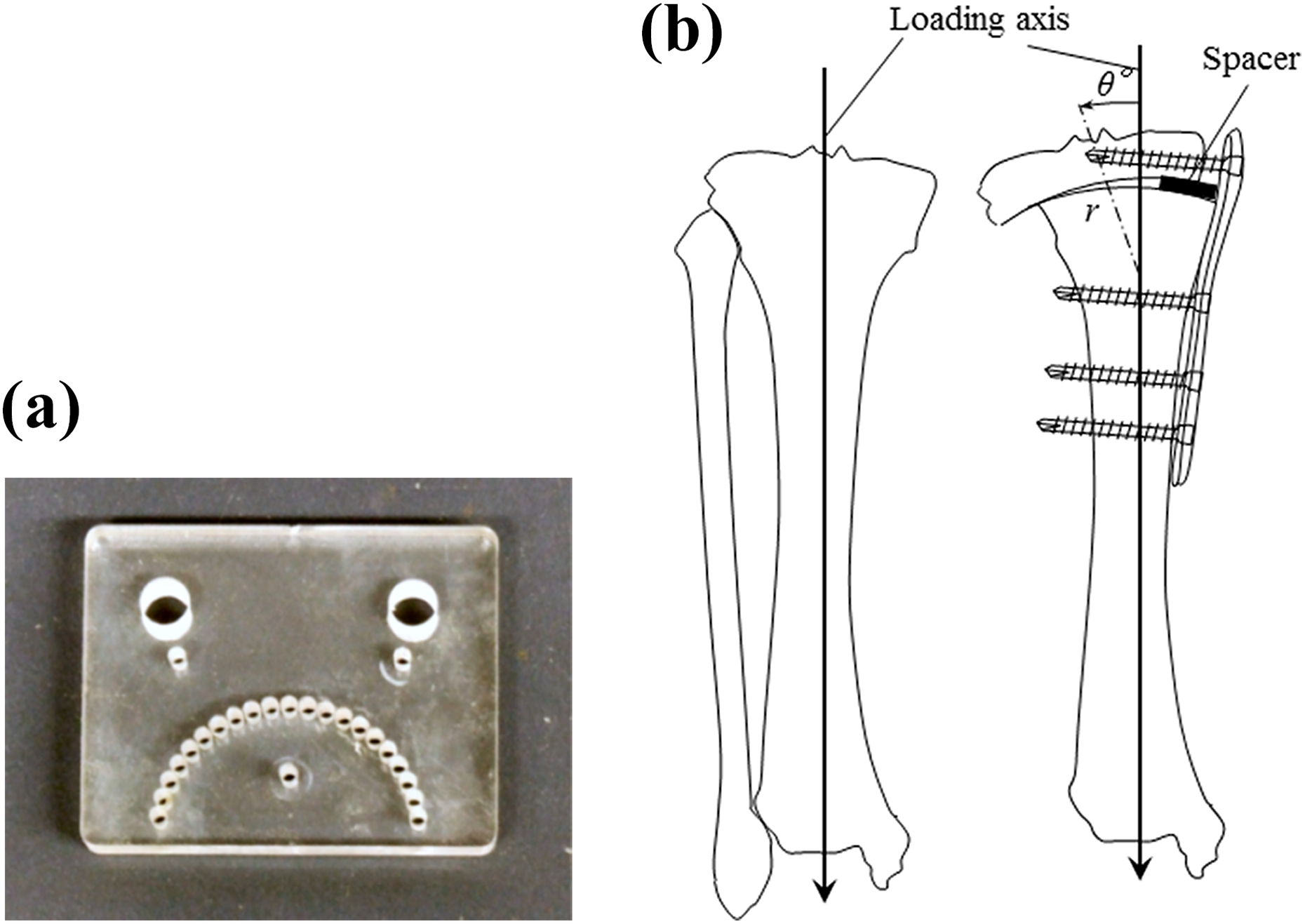
(a) Osteotomy plate; (b) HTO correction angle and loading axis. HTO: high tibial osteotomy.
HTO correction angles of 15° and 20° were used in all experiments, as shown in Figure 1(b). We measured the angle of θ using the loading axis line of tibial shaft and center of joint surface during the fixation of HTO site. The osteotomy site was fixed by PHILOS® plate (SYNTHES Co. Ltd, Tokyo, JAPAN) and locking screws with rectangular aluminum alloy (A5083) spacers measuring 15 mm wide, 20 mm long, and 5 mm thick. In experiments without spacers, the spacer was removed after mounting the plate. As shown in Figure 2, two-piece locking screws were used to fix the upper part of the plate, and three-piece screws fixed the lower part. Finally, to perform cyclic loading tests, steel grip bars were fixed onto the distal part of the loading axis of each HTO specimen.

Absolute locations of screws on the PHILOS® plate.
Experimental procedures
The cyclic loading tests were performed in a fatigue testing machine (INSTRON 8516, 98kN Servo Hydraulic Machine, INSTRON Japan, Co. LItd, Kawasaki, Japan). The HTO specimen was mounted on a hydraulic grip, as shown in Figure 3. Tibial loading axis was set perpendicular to the ground, and compression force was applied perpendicular to the tibial axis.

Fatigue testing machine and mounted HTO specimen. HTO: high tibial osteotomy.
To compare initial displacements in HTO specimens with and without spacers, quasi-static compression tests were carried out at a loading rate of 600 N/min until 1100 N. The displacement of the osteotomy space was measured by actuator displacement of the test machine.
Assuming that the maximum loads of walk rehabilitation and normal walking are 1000 and 2000 N, the cyclic loading test conditions were a stress ratio of R = 0.1 and a cyclic frequency of f = 0.5 Hz. After the test condition of 1000 N had completed 1000 cycles, a further 1000 cycles were performed at 2000 N.
Change of displacement range was recorded during each test. Twelve test specimens were used for each angle of the HTO cyclic loading test.
Displacement in cyclic loading tests
Change in displacement range
The displacement range Δδ is defined as the difference between maximum δ max and minimum displacement δ min

The normalized displacement range is defined as the displacement range change normalized by the initial displacement range Δδ ini at which the loading range steadied around 40 cycles:

The initial fixed state was 100%. That is, if the initial fixed state is maintained, it remains at 100% during cyclic loading.
Results
Effect of spacer on displacement in quasi-static compression
Load–displacement curves up to 1100 N are shown in Figure 4. It was observed that the displacement of the osteotomy space increased nonlinearly with increasing load in all specimens. A comparison of the displacements of the HTO correction angles showed that the displacement at 15° was smaller than that at 20°. In spite of the dome-shaped cutting line, the HTO correction angles’ dependence arose because of slips in directions other than the direction of the loading axis. Displacements with a spacer were smaller than those without a spacer at all HTO correction angles. The reduction ratios of displacement with and without spacers at HTO correction angles of 15° and 20° were 37% and 27%, respectively, as shown in Table 1.
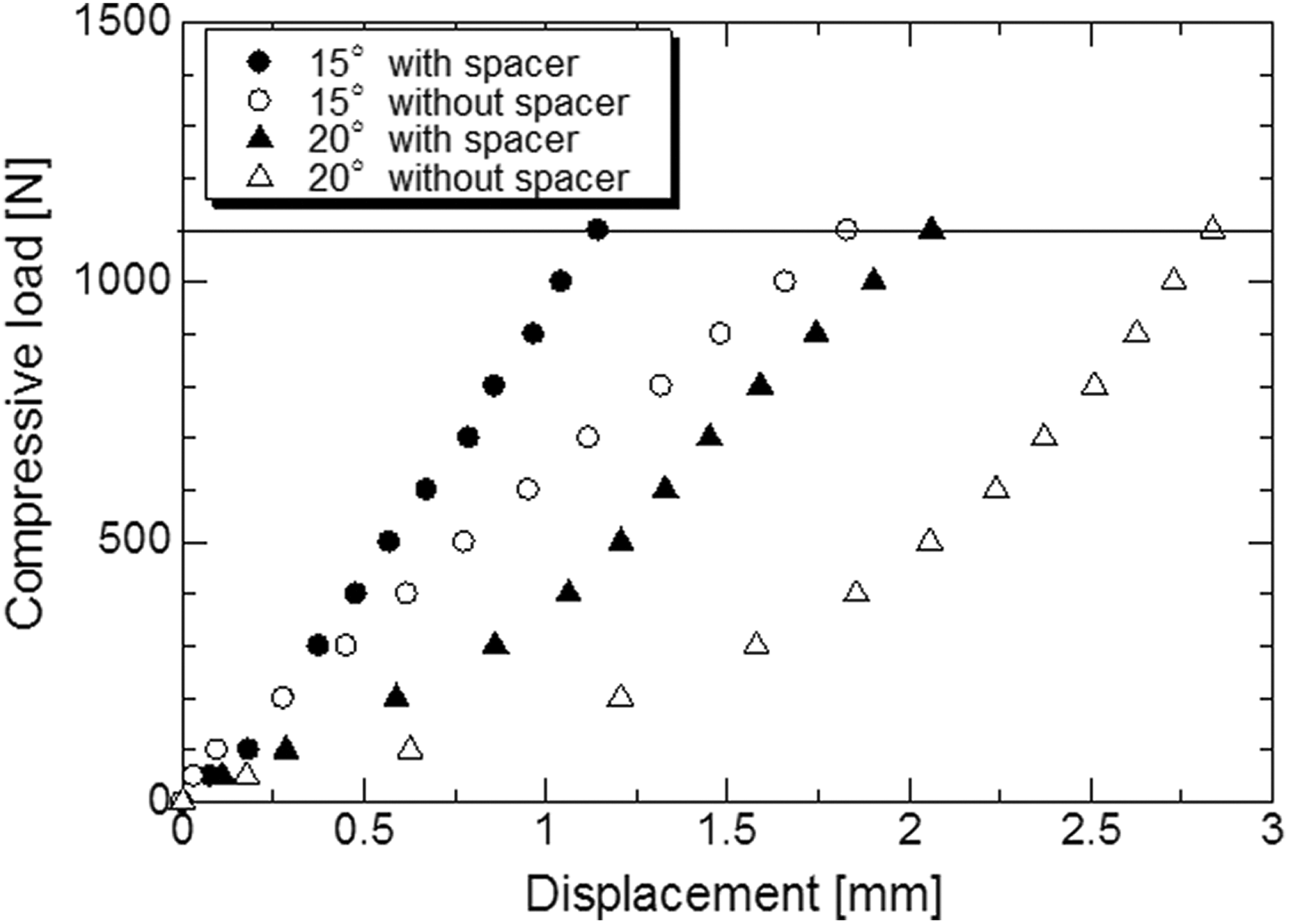
Relationship between compressive load and displacement up to a quasi-static compressive load of 1100 N.
Comparison of displacement with and without spacers in quasi-static compression tests.
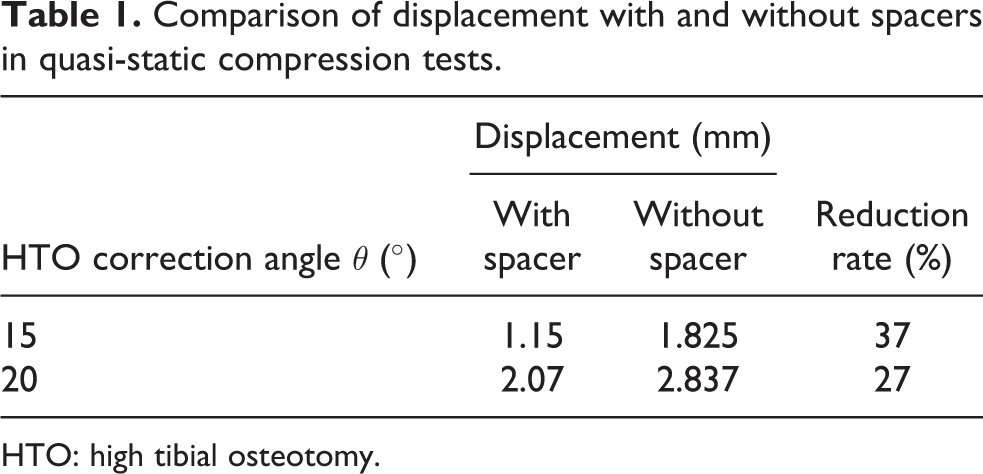
HTO: high tibial osteotomy.
Displacement in cyclic loading tests
The initial displacement ranges of the present experiments are shown in Table 2. The initial displacement ranges with and without spacers showed tendencies similar to those observed in the quasi-static tests.
Normalized displacement amplitude at 1000 cycles.

HTO: high tibial osteotomy.
Changes in the normalized displacement range at the correction angles of 15° and 20° are shown in Figure 5. The displacement ranges decreased with increasing number of cycles; that is, the osteotomy space becomes small. Comparing tests with and without spacers at 1000 N under a correction angle of 15°, the displacement range was almost identical at the initial stage, but the difference between samples with and without spacers then increased gradually (Figure 5(a)). After 1000 cycles, the normalized Δδ/Δδ ini with a spacer had decreased by nearly 10%. In the case of 2000 N, the spacer had little influence on the displacement range.

Relationship between normalized displacement range and number of cycles at HTO correction angles of 15° (a) and 20° (b). HTO: high tibial osteotomy.
On the other hand, in a comparison of samples with and without spacers under a correction angle of 20°, changes in the displacement ranges without a spacer at 1000 and 2000 N corresponded to 15° (Figure 5(b)). Furthermore, the spacer had little influence on the displacement range at either 1000 or 2000 N. The results of the displacement amplitudes at 1000 cycles are shown in Table 2.
Changes in maximum displacement
Changes in δ max at the correction angles of 15° and 20° are shown in Figure 6. Changes in δ max are represented by a difference from the initial value of maximum displacement and were found to increase with increasing number of cycles. The results of the maximum displacement at 1000 cycles are shown in Table 3. A comparison of the data with and without spacers at 1000 cycles shown in Table 3 reveals that δ max with a spacer at the correction angle of 15° increased more than that without a spacer of 0.13 mm at 1000 N. In the case of 2000 N, changes in δ max with a spacer corresponded to those without a spacer. In the case of the higher HTO angle (20°) as shown in Figure 6(b), changes in δ max with a spacer at the correction angle of 20° corresponded to those without a spacer at 1000 N. δ max with a spacer, however, decreased more than that without a spacer of 0.19 mm at 2000 N (Table 3).
Maximum displacement at 1000 cycles.

HTO: high tibial osteotomy.
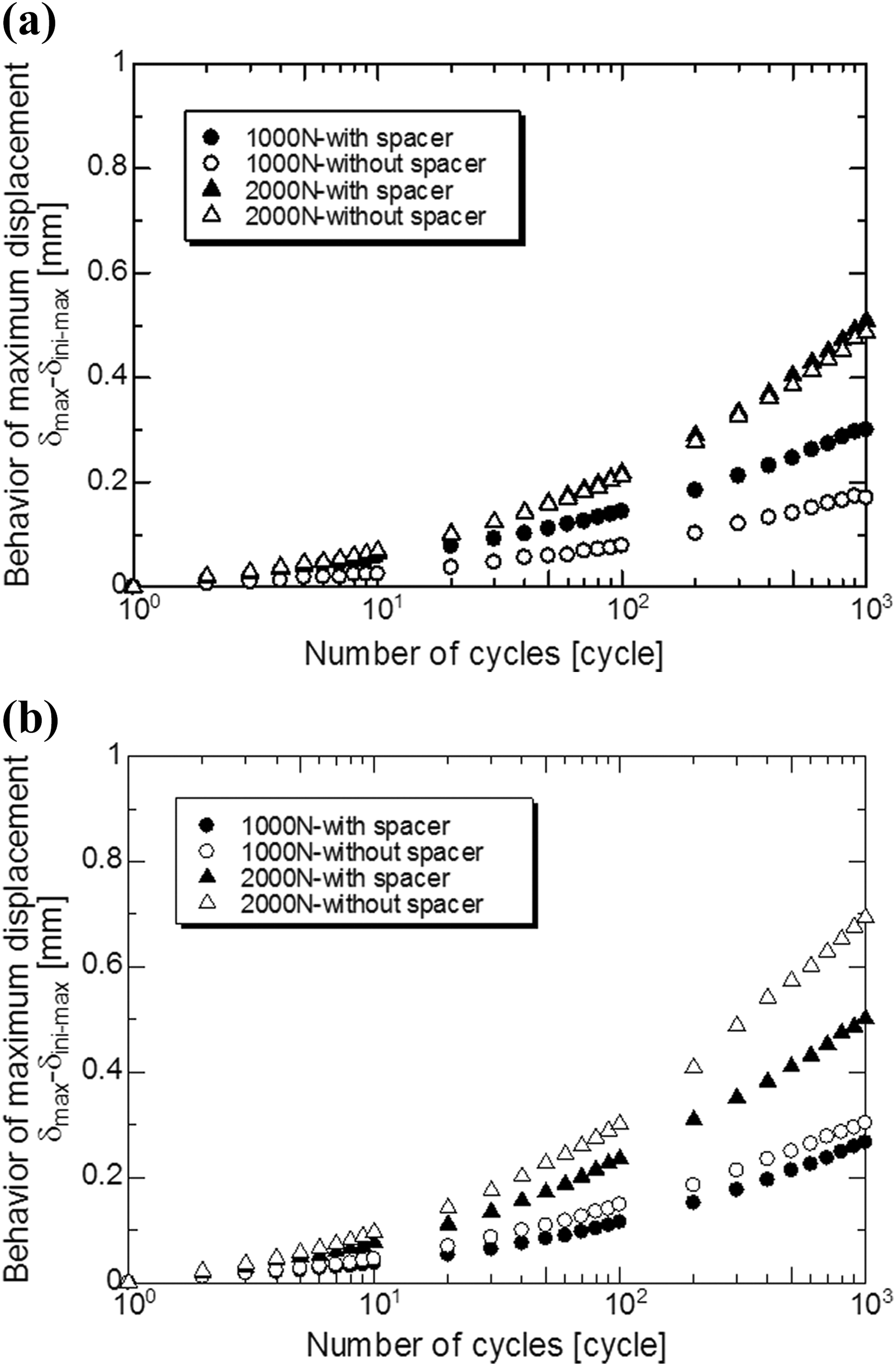
Relationship between maximum displacement and number of cycles at HTO correction angles of 15° (a) and 20° (b). HTO: high tibial osteotomy.
Discussion
Surgical HTO procedures include wedge osteotomy, 10 medial open wedge osteotomy, 3 and dome-shaped osteotomy. 9,11 Plate fixation has been shown to have a greater fatigue life than blade staples and tends toward less displacement in 15° closed-wedge osteotomies. 12 Recently, the use of medial open-wedge osteotomy has increased, 4 and there have been several reports on the mechanical strength of the fixation methods. 12 –16 Open-wedge osteotomy is able to facilitate early rehabilitation and achieves a good range of motion. It is not necessary to perform osteotomy of the fibula. In contrast, the HTO correction angle should be less than 15° because the gap at the osteotomy site increases due to the enlargement of the correction angles.
With respect to open-wedge osteotomy, Puddu et al. created a spacer plate which is able to support the osteotomy space during osseous consolidation 15 and which is reported to involve certain specific pitfalls, such as loss of correction, and fracture of lateral cortex, that are technically demanding. 17 The stability of the osteotomy site is particularly disrupted both axially and torsionally after the failure of the lateral cortex, and additional fixation is needed. 15 In contrast, the TomoFix plate®, which was developed by Staubli and De Simonni, makes use of the concept of the locking head screw, which provides rigid fixation of the osteotomy site. The TomoFix plate® provides greater stability and is superior to the Puddu plate® as well as to the short spacer plate. 15,18 –20 In the present study, we used a locking screw system in combination with a PHILOS®, which is smaller than a TomoFix plate, because the former is the appropriate size for the pig tibia.
Dome-shaped HTO is an acceptable way to correct a large deformity in comparison to other osteotomy methods, because it has a large contact area at the osteotomy site and shows good clinical results. However, there is a gap of several millimeters at the medial site of the osteotomy, which means that there needs to be a large correction angle. In such cases, it is generally believed that the stability of the osteotomy may be decreased; however, to the best of our knowledge, there has been no detailed report on the biomechanical stability of dome-shaped HTO, nor has there been any report on whether the stability of the osteotomy site would change by the insertion of a spacer.
In the present study, the reduction ratios of displacement with and without spacers at HTO correction angles of 15° and 20° were 37% and 27%, respectively. No effect of the spacer was observed at a correction angle of 15° in the cyclic loading test; however, the maximum displacement and amplitude were reduced with a spacer at the correction angle of 20°.
δ max with a spacer at a correction angle of 20°, however, decreased more than that without a spacer of 0.19 mm at 2000 N. Based on the results of these experiments, when the HTO correction angle is small, the effect of the spacer is uncertain. However, the spacer is effective at an HTO correction angle of 20°.
Further studies are needed to continue the present examination with larger numbers of samples and changing the loads, the number of more repeated frequency, and the shape of the spacer. It is also necessary to improve the fixation technique and materials for the medial opening wedge osteotomy in the future.
Conclusions
The reduction ratio of the displacement was approximately 30% at HTO correction angles of 15° and 20° with and without spacers. No effect of the spacer was observed at a correction angle of 15° in the cyclic loading test, however, the maximum displacement and amplitude were reduced with a spacer at the correction angle of 20°.
Supplemental material
Supplemental_material_792406 - Biomechanical study of optimum anchorage in dome-shaped high tibial osteotomy
Supplemental_material_792406 for Biomechanical study of optimum anchorage in dome-shaped high tibial osteotomy by Toshiaki Takahashi, Manabu Takahashi, Haruyasu Yamamoto, and Hiromasa Miura in Journal of Orthopaedic Surgery
Footnotes
Acknowledgment
We thank Yasuyuki Kimoto, MEng, for the assistance in study experiments.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.