
Abstract
Purpose:
The purpose of this article was to assess the clinical outcome of high tibial osteotomy (HTO) with articular cartilage surgery compared with unicompartmental knee arthroplasty (UKA) in unicompartmental osteoarthritis (OA).
Methods:
We designed retrospective study and evaluated 47 patients with unicompartmental OA (Kellgren–Laurence [K–L] grade ≥III OA). Two groups of patients underwent either HTO with articular cartilage surgery or UKA by the senior author between January 2010 and April 2013. The minimum follow-up period is 2 years. Clinical outcomes were assessed using Knee Injury and Osteoarthritis Outcome Scores, International Knee Documentation Committee (IKDC), and visual analog scale (VAS) score. And we evaluated the radiologic result of HTO and UKA by measuring mechanical axis at preoperative period and at last follow-up.
Results:
The IKDC score was significantly better in the UKA group than in the HTO group at 6 months but there was no significant difference in the two groups at 2 years. The VAS score was improved at the final follow-up compared to before surgery in both groups and did not show significant intergroup difference (p = 0.123). There was no significant difference in the preoperative mechanical axis in the two groups. But their mechanical axis at the final follow-up were significantly different (p = 0.0001).
Conclusion:
The clinical outcome was significantly better in the UKA group at 6 months. But in the two groups, there were no significant differences at 12 months and 2-year follow-up, and the mechanical axis correction effect is greater than the UKA group. Based on our research, HTO with articular cartilage surgery can be considered as the treatment of choice for more active and younger patients with unicompartmental OA.
Keywords
Introduction
The surgical treatment methods for unicompartmental osteoarthritis (OA) of the knee largely include high tibial osteotomy (HTO) and unicompartmental knee arthroplasty (UKA). 1 –3 The differences of indications and clinical prognoses of these two surgical approaches are still debated. Recently, HTO has become widely used to correct varus deformity by shifting the weight-bearing axis to the unaffected lateral compartment. 4,5 Several studies reveal good prognosis for HTO, for which malalignment of the medial compartment of knee OA had been corrected. However, it is technically difficult to achieve ideal valgus knee after surgery. Also, occurrence of complications after HTO is higher than that after UKA. However, reports of clinical prognosis–related study on HTO have been mainly the closing wedge type. 6 –9 Recently, opening wedge HTO has been popular and more widely used with good clinical outcomes. A concurrent repair of an injured cartilage also improved the prognosis. 10 –12 Lately, few studies were conducted to directly compare the clinical results of opening wedge HTO and UKA. Reports have shown excellent long-term results from these two groups. 13,14 In comparison with HTO, UKA is a reconstructive surgery that replaces the worn-out articular surface with an artificial structure. This process preserves the articular surface of the healthy side. Also, weight-bearing ambulation and early rehabilitation are possible within a short time, and therefore the advantage is less postoperative complications. 10,12,15,16
Nevertheless, UKA has a significant disadvantage. Owing to the fact that UKA demands high technical skill, it is difficult to precisely make the correction of malalignment and positioning of implants in cases with unicompartmental knee OA. Furthermore, complications may develop, such as implants loosening, failure, or infection. However, with improvement of surgical techniques and instruments, the demand for UKA has increased in the last several years, while a better long-term prognosis has been shown. 1,17,18 As shown earlier, advances in surgical methods and techniques for both UKA and HTO have led to the expansion of indications. Respectable results are shown in low-grade unilateral compartmental OA, despite some differences between these two methods. Nevertheless, there are nearly no studies on clinical results of its application and prognosis for patients with severe unicompartmental OA. In this retrospective study involving patients with severe unicompartmental knee OA, the clinical result of HTO concurrently with cartilage injury repair was compared and analyzed with that of UKA.
Methods
This retrospective study included 47 patients, who had been diagnosed as having unicompartmental OA of grade 3 or 4 under the Kellgren–Laurence (K–L) system and had undergone HTO with injured cartilage repair and UKA by the senior author in this hospital from April 2010 through May 2013. The minimum follow-up duration was 2 years with a mean follow-up period of 34.7 months. Of those 47 patients, 26 had undergone HTO, while 21 had undergone UKA. The protocol of this retrospective research was approved by the Institutional Review Board of this hospital. This study excluded cases with (1) lateral and patellofemoral compartmental OA of the K–L grade 2 or higher, (2) range of motion (ROM) is 120° or less, (3) flexion contracture is in excess of 20°, (4) ligament instability, or (5) inflammatory arthritis. The choice of surgical method of either HTO or UKA was decided by patients. With respect to surgical technique, medial opening wedge HTO was performed. The Miniaci method 19 was used to obtain the angle of correction. Osteotomy was performed under the control of the C-arm and the osteotomy gap was filled with the pieces of cancellous bone allograft. Then, the Synthes TomoFix Medial High Tibial Plate was used for fixation. The Zimmer Unicompartmental High Flex Knee system was used for UKA, and bone cement was used for fixation in all cases. The Knee Injury and Osteoarthritis Outcome Scores (KOOS), International Knee Documentation Committee (IKDC), and visual analog scale (VAS) scores were used for the clinical assessments of these two groups, before surgery, 6 months after surgery, 1 year after surgery, and 2 years after surgery. These values were utilized as measurement indices for clinical prognosis. Also, the postoperative complications of patients in these two groups were also evaluated and compared. All survey questionnaires and clinical data were recorded and evaluated by clinicians. A radiologic evaluation was performed by obtaining the mechanical tibiofemoral angle in the weight-bearing radiographs before surgery and at 2-year follow-up observation. And union at the osteotomy site in the HTO group was assessed on anterior–posterior and lateral radiographs at 6 and 12 weeks after surgery and then as required until bone union was evident. Delayed union was defined as lack of bridging callous and presence of radiolucent areas within the opening wedge defect more than 3 months after surgery, and nonunion as no evidence of healing within 6 months. Implant loosening in the UKA group was defined by a periprosthetic lucency of >3 mm, a progressive lucency with time, or obvious fracture-dislocation of a prosthesis.
Regarding postoperative physical rehabilitation in the HTO group, ROM exercise, patella mobilization, and quadriceps setting exercises were started a day after surgery, while partial weight-bearing was allowed 6 weeks after surgery. Patients who underwent UKA started ambulation immediately after the volume in the Hemovac reached 100 cc or less. These patients were allowed weight-bearing ambulation with a walker or a crutch up to 6 weeks after surgery. Then, they were allowed to ambulate freely. The IBM SPSS 19.0 version was used for statistical analyses of indices, while the repeated analysis of variance test was used for the comparison of measured value differences before and after surgery. A paired t-test was utilized for the comparisons of measured values between these two groups. A p-value less than 0.05 is considered statistically significant.
Results
Patient demographics
The mean age of patients who underwent HTO was 56.8 years (with a range of 43–58 years), while that of patients who underwent UKA was 60.7 years (with a range of 51–76 years), but this difference in age was not statistically significant (p = 0.052). Regarding gender, 4 males and 22 females underwent HTO, while 4 males and 17 females underwent UKA. The mean body mass index (BMI) of HTO patients was 26.6, while that of UKA was 26.1. The mean BMI of patients in both groups increased (Table 1).
Patient demographics.
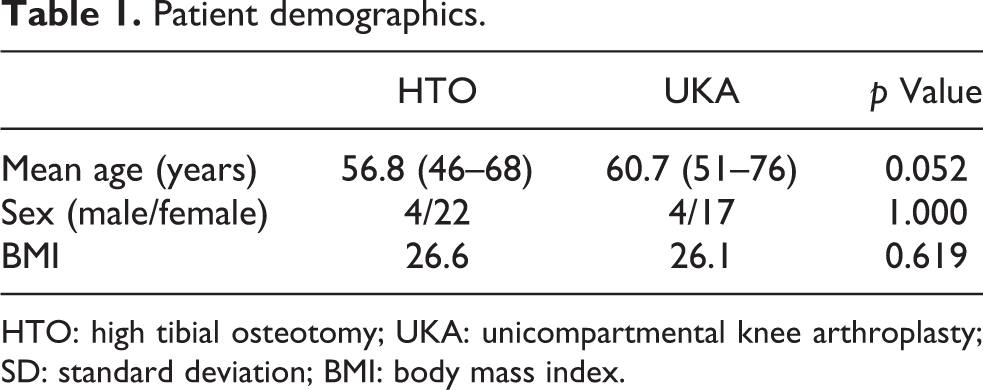
HTO: high tibial osteotomy; UKA: unicompartmental knee arthroplasty; SD: standard deviation; BMI: body mass index.
Functional outcome
The KOOS of patients in the HTO group before surgery, 6 months after surgery, and 12 months after surgery were 72.19, 94.15, and 105.61, respectively. The KOOS score decreased to 103.92 at the 2-year follow-up. The KOOS scores of patients in the UKA group before surgery, 6 months after surgery, and 12 months after surgery were 67.66, 100.95, and 104.52, respectively. The KOOS scoring decreased to 104.04 points at the 2-year follow-up. The IKDC scores for patients in the HTO group before surgery, 6 months after surgery, and 12 months after surgery were 26.87, 42.56, and 51.10, respectively, showing improvement. However, the IKDC score decreased to 50.17 at the 2-year follow-up observation. The IKDC scores for patients in the UKA group before surgery, 6 months after surgery, and 12 months after surgery were 33.65, 53.68, and 57.13, respectively, showing improvement. However, the IKDC score decreased to 56.86 at the 2-year follow-ups. The IKDC score of patients in the UKA group 6 months after surgery was statistically significantly increased. However, there was no statistically significant difference in the IKDA score of patients between these two groups 12 months after surgery and at the 2-year follow-up (Tables 2 and 3). The injured cartilage surgery performed concurrently with HTO were 9 cases of autologous chondrocyte implantation (ACI), 4 cases of chondroplasty, 10 cases of meniscectomy and microfracture, as well as 3 cases of meniscectomy and chondroplasty. Regarding complications, there were two cases of complications, such as leg length discrepancy and fibroarthrosis, in the HTO group, while there was one case of peroneal palsy complication in the UKA group. However, there was no statistically significant difference in the occurrence rate of complications between these two groups (p = 0.654).
IKDC score.

IKDC: International Knee Documentation Committee; HTO: high tibial osteotomy; UKA: unicompartmental knee arthroplasty; SD: standard deviation.
KOOS score.

KOOS: Knee Injury and Osteoarthritis Outcome Scores; HTO: high tibial osteotomy; UKA: unicompartmental knee arthroplasty; SD: standard deviation.
VAS score
The VAS score at the final follow-up improved as opposed that before surgery for both groups. However, data between these two groups showed no statistically significant difference (p = 0.123; Table 4).
VAS score.

VAS: visual analog scale; HTO: high tibial osteotomy; UKA: unicompartmental knee arthroplasty; SD: standard deviation.
Radiologic measurements
There was no statistically significant difference in the angle of mechanical axis between the two groups before surgery. Nevertheless, the mean angle of mechanical axis of the knee in the HTO group at the final follow-up showed a 1.06° valgus deviation, while that of the UKA group revealed a 2.71° varus deviation, showing a statistically significant difference (p = 0.0001; Table 5). Bony union at the osteotomy site occurred on radiographs on an average of 12 weeks postoperatively in 24 cases (92.3%) and delayed union occurred in 2 cases (7.7%). However, two patients with delayed union underwent complete unions in 6 months and had no clinical symptoms such as load-dependent pain at the osteotomy site and pain at the osteotomy site. And no loosening implant in the UKA group was seen in our study period.
Mechanical axis.

HTO: high tibial osteotomy; UKA: unicompartmental knee arthroplasty; SD: standard deviation.
Discussion
OA may affect various compartments of the knee joint. Many patients are inflicted with medial compartmental arthritis, and one-third of these patients have a single compartment involvement. 20 The original goal of HTO was to correct the angular deformity of the knee joint, or the malalignment of tibial metaphysis, which can induce weight overbearing and pain of the medial knee joint. Ideal patient selection is the single most important factor of successful outcome in HTO. Various papers reported several common conditions that reflect a poor prognosis. The risk factors that lead to poor prognoses include (1) old age, (2) extent of OA, (3) degenerative lesion of lateral and patellofemoral compartment, (4) remarkably reduced ROM, (5) joint instability, or (6) presence of a lateral tibial thrust. 21 –25 Among these risk factors, age is the most important one in the selection of a candidate for HTO procedure. As the age increases, the failure rate increases 7.6% every year. The relative risk of patients with an age of 65 years or older is 1.5 times greater. Thus, it was reported that HTO would not be recommended for elderly patients with an age of 65 years or older. 26 Nevertheless, the recent trend is that indications for HTO have been expanded to include posterolateral laxity, varus hyperextension thrust, anterior cruciate ligament deficit, varus thrust, or alignment. 27 The reasons are that understanding of the tibial slope and advances in correction technologies have improved stability of the knee joint. Thus, indications for HTO have expanded. Additional cartilage surgery techniques were currently added to improve prognosis further. 22,28,29 In our study, 9 cases of ACI, 4 cases of chondroplasty, 10 cases of meniscectomy and microfracture, as well as 3 cases of meniscectomy and chondroplasty were performed and showed good clinical outcome.
UKA is a partial replacement of the knee joint. It can replace a severely damaged compartment. Owing to fast recovery time with less invasiveness and preservation of the tibia compared to total knee replacement arthroplasty, clinicians seem to prefer this procedure in recent times. 30 Ideal indications for UKA include (1) unicompartmental OA with well-preserved lateral and patellofemoral joint compartment, (2) avascular necrosis of femoral condyle, (3) an age of 60 years or older, (4) less activities, (5) nonobese, (6) cases with no pain during resting phase, (7) flexion contracture of less than 5° and joint ROM of 90° or greater, and (8) malalignment of the axis of 10° deviation or less, which can be corrected with a nearly neutral posture. 18,31
Owing to the fact that UKA and HTO, each with unique features, have similar indications, the choice of a surgical treatment for unicompartmental knee OA is still in debate. Up to now, reports limited to comparative analysis between UKA and HTO are largely UKA and lateral closing wedge HTO. 22,30 Broughton et al. retrospectively investigated UKA and lateral closing wedge HTO in their follow-up observations for 5 years. They reported respectable results of 76% for UKA and 43% for HTO. Sukenborg-Colsman et al. prospectively compared prognoses of UKA and HTO for 7 to 10 years and reported better prognosis and less surgical-room complications for UKA. 10,12
The reported results of UKA generally showed better results in terms of clinical prognosis and survival rate. However, the improvements of surgical method and instruments after opening wedge HTO have also led to improved clinical results. Dettoni et al. compared UKA and opening wedge HTO for the first time and found that both these groups showed an excellent mid-to-long-term prognosis clinically and radiologically at the final follow-up observations. 30 Conclusively, either HTO or UKA is a rather outstanding surgical treatment as long as appropriate selection of a patient can be made.
Considering the results of the mechanical axis, patients in the HTO group showed a statistically significant tendency of postoperative valgus alignment, in comparison with those in the UKA group. Broughton et al. asserted that the main cause of unsatisfactory results from the HTO group came from insufficient correction. 10 Kozinn et al. reported that there would be a high possibility of showing good results at long-term follow-up when HTO could correct the mechanical alignment of the axis by 7° or greater. 18 However, it is technically not easy to obtain ideal valgus alignment. Furthermore, with respect to degenerative change of the knee joint, there is a report that a degenerative change of lateral tibiofemoral compartment has not shown significant difference between HTO and UKA groups, despite having achieved a greater valgus alignment by HTO. 32 Accordingly, it is necessary to clearly elucidate a correlation between correction of mechanical axis and clinical outcome through further prospective random studies.
UKA is known as a surgical method with advantages of fast return to activities of daily living and early recovery from pain, and thus the authors found similar results in this study. The early clinical result of UKA at 6-month follow-up was better, in comparison with that of HTO, showing a statistical significance. The clinical results of these two groups at 12-month follow-up and at 2-year follow-up were similar, showing no statistical significance. The early postoperative differences between the two groups might have been due to (1) weight-bearing taking place in the HTO group beginning 6 weeks after surgery and (2) the aspect that the osteotomy site would not be completely healed at 3 months after surgery. Furthermore, owing to a larger change in angular correction of the HTO group, it seemed that normal ambulation would take more time. The disadvantage of having a longer duration of physical rehabilitation after HTO is one factor, for which elderly patients prefer UKA. However, such a shortcoming can be remedied in the group of relatively younger patients less than 60 years old.
Clinicians may consider HTO as a sufficient treatment option since this procedure can largely preserve a patient’s own knee joint and has a large corrective effect of the mechanical axis. With respect to complications, both these groups showed overall low occurrence rates, which might be due to improvement in surgical technique. Several studies reported OA progression on the patellofemoral joint in both groups of HTO and UKA. 32 Such findings were not observed in this investigation. This issue may be due to a relatively short follow-up observation period, which necessitates further studies in the days ahead.
Conclusion
In this study, clinical and radiologic prognosis, including recovery to activities of daily living, were evaluated from at least 2-year follow-up after HTO and UKA, which had been performed for medial compartmental OA. The results of this study revealed achieving respectable functional prognosis in both groups of HTO and UKA postoperatively, and there was no statistically significant difference in the clinical outcome between these two groups. Early recovery of the HTO group was slower than that of the UKA group. Nevertheless, HTO has advantages of not having bone loss from joint replacement and preserving a patient’s own joint, as well as a large corrective effect of the mechanical axis, making it easy to perform future total knee replacement. Furthermore, there are recent reports of improved clinical prognosis as injured cartilage repair has been concurrently performed. In consideration of these clinical results, HTO seems to be the surgical option that could be preferentially selected in the group of young active patients with unicompartmental OA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Inha university hospital.