
Abstract
Purpose:
Objective and reliable force measurement is necessary to monitor the rehabilitation after triceps brachii pathology, injuries, and posterior approach–based surgery. It is unclear at which amount of extension the triceps is best tested and if comparison to the uninjured sided is reliable. This study aims to identify the most reliable elbow position at which elbow extension force is measured using a dynamometer. Furthermore, it aims to compare the extension strength of the dominant arm with that of the nondominant arm.
Methods:
Isometric elbow extension force of the dominant and nondominant arms of healthy subjects was measured. The measurements were taken in three sequences per arm in 0, 30, 60, 90, and 120 degrees of flexion. A subgroup repeated the measurements to analyze test–retest reliability using intraclass correlation.
Results:
We included a total of 176 volunteers. The repeated measures analysis of variance for within-subject effect showed the lowest variation coefficient at 30 degrees of flexion. Extension forces showed a mean difference of 3.2–6.9 N in advantage of the dominant arm, resulting in ratios from 1.05 to 1.09. Learning curve analysis showed that during the first session in dominant and nondominant arms, less forces were exerted.
Conclusion:
The most reliable isometric triceps brachii muscle strength measurement was at 30 degrees of flexion of the elbow. Considering the learning curve, a first tryout session for both arms is indicated. Then, a second measurement suffices as no further learning curve is observed.
Introduction
As the elbow provides flexion, extension, and rotation of the forearm, several muscle groups are involved. Contraction of the triceps brachii muscle and, when almost in full extension, the anconeus muscle, leads to elbow extension. In case of insufficiency, if the triceps brachii tendon rupture, active extension of the forearm is not possible, resulting in impairment of the upper limb. 1
Traumatic rupture of the triceps tendon is not frequently encountered and is often missed in the emergency department. 2 –4 It is unclear in which amount of flexion the triceps is tested, nor is clear if comparison to the uninjured site is reliable.
Insufficiency of the triceps can also be seen after posterior approach–based surgery as reconstruction of a ruptured triceps, after fixation of fractures of the proximal ulna, or after exposure for distal humeral fractures or total elbow arthroplasty. 5 –8 For surgical repair of a ruptured triceps tendon, several methods have been described for fixation. 9 –11 Complete ruptures are commonly treated by surgical repair, while partial ruptures can be treated conservatively by splinting. 4,11,12
During follow-up after triceps rupture or other pathology, detailed, objective, and repeatable information on muscle force is essential. To monitor rehabilitation and guide return to activity, extension force can be measured during the follow-up. The five-point Medical Research Council muscle strength scale can be used but lacks detail as it describes muscle force against subjectively described criteria as “slight,” “moderate,” and “strong resistance.” 13 More objective elbow extension force testing is needed. Moreover, it is not clear of comparison to the uninjured side is reliable.
Simple muscle force testing can be a solution to objectify muscle strength. Muscle strength testing may consist of dynamic isokinetic testing or static isometric testing. Isokinetic testing usually involves a large apparatus, while isometric testing can be performed with a portable, small dynamometer and also has an acceptable test–retest reliability for elbow flexion and extension. 14 However, multiple sources of error are likely to be introduced by the procedure or the examiner. 14 Standardized positioning of the patient is of importance, as during movement of a joint, the contracting muscle shortens and leverage forces change. Moreover, the triceps brachii exerts different forces at different angles of the elbow. 15
Therefore, this study investigates the reliability of elbow extension force in healthy volunteers using a dynamometer in different angles of elbow extension. Reliability is defined by a low coefficient of variation and a high test–retest reliability. In addition, we explored that the uninjured side can be used reliably to assess the recovery after posterior approach–based surgery, with the uninjured arm as the reference.
Materials and methods
Subjects
One hundred and seventy-six healthy volunteers, above 18 years without any pathology of the elbow, were enrolled.
The volunteers were recruited from the orthopedic staff (nurses, secretaries, and staff) and interested visitors of the outpatient clinic. Exclusion criteria were current or previous elbow surgery or elbow complaints and inability to follow instructions and filling in questionnaires. The Institutional Review Board of our hospital waived approval for the study. All subjects provided informed consent before participation in the study.
Experimental setup
All measurements were performed using the MicroFET 2 dynamometer (Hoggan Health Industries, Salt Lake City, UT, USA). The dynamometer was programmed to measure the forces in Newton (N). The session consisted of sequences of tasks in which extension was performed in full extension (0 degrees of elbow flexion) and in 30, 60, 90, and 120 degrees of elbow flexion. The sequence always started at the smallest degree of flexion of the nondominant arm and the angle was increased incrementally. Subsequently, the dominant arm was tested in all previously mentioned angles. We performed three of these sequences per arm during one session.
The examiner sat at a table in front of the volunteer. The volunteer placed the elbow on a plateau of the same height as the top part of the dynamometer to prevent leverage over a ramp under the forearm. For standardized angles of flexion of the elbow, wedges of 30°, 60°, and 90° were sequentially placed under the upper arm as illustrated in Figure 1. With the thumb pointing upward, the pronators and supinators of the forearm could not exert extra pressure on the dynamometer. The dynamometer was positioned in line with the plateau 1 cm proximal to the styloid process of the ulna, to prevent forearm muscles and the wrist to interfere with the force produced by the triceps brachii. To measure the extension force in 120 degrees of flexion, the volunteer had to flex the elbow to 120° and push against the dynamometer held by the examiner. This was done in a standing position or in a sitting position by both the volunteer and the examiner. The examiner had to withstand the extension force to maintain elbow flexion of 120°, so no actual extension of the elbow was made and isometric force was measured.

Setup for testing of different flexion angles using the wedge. The upper arm is put on the wedge, with the elbow on a plateau of the same height as the dynamometer. (a) 0 degrees of flexion, (b) 30 degrees of flexion, (c) 60 degrees of flexion, (d) 90 degrees of flexion, and (e) 120 degrees of flexion.
To evaluate repeatability of the tasks, a random subgroup of 20 volunteers performed a second session with a minimum interval of 1 week. The same examiner performed the measurements using the same protocol as during the first session. The volunteers were blinded to previous measured values.
Data and statistical analyses
Data were collected and analyzed using SPSS version 23 (IBM, Armonk, New York City, USA). The variation coefficient was calculated for both dominant and nondominant arms to analyze which degree of flexion was most accurate. The variation coefficient is calculated by dividing the standard deviation (SD) by the mean, which results in a ratio that describes the dispersion in measured values. Since previous research showed that a “tryout” measurement was useful in measuring hip flexors because of a learning curve, the first step in the analyses was to determine whether we would use all three measurements or only the second and/or the third measurement. 16 Therefore, a potential learning curve was examined using a repeated measures analysis of variance (ANOVA) for all measurements per arm in each elbow flexion angle. A significant difference implies a difference between sessions and could reveal a learning curve.
Test–retest reliability was measured with two-way random intraclass correlation coefficients (ICCs) for the subgroup of volunteers who completed a second session. For each arm and every flexion angle, an ICC was calculated. To determine ratios between dominant and nondominant arms, a ratio was calculated by dividing the mean extension force of the sequences of the dominant arm by the mean extension forces of the nondominant arm in each position. Paired t-tests were used to test the differences between dominant and nondominant arms. A p-value of less than 0.05 was considered as significant, and when five or more tests were performed on the same subject, a significance level of p < 0.01 was used.
Results
We included 176 volunteers, 88 women and 88 men. Mean age was 44.1 years with an SD of 18.8 years (mean age of men: 50.4 years, range: 19–93 years; mean age of women: 37.7 years, range: 18–87 years). Of all participants, 86% had the right arm as dominant side (men 86% right dominance; women 86% right dominance).
Assessment of the learning curve revealed a significant difference in the repeated measure ANOVA for almost all tasks (Table 1). Post hoc analysis showed that during the first sequence in nondominant arms, significantly fewer forces were exerted on the dynamometer, for all degrees of flexion, compared to the second and third sequences. For the dominant arm, this effect was observed in 0, 30, and 60 degrees of flexion (Table 1). Because of this learning curve, only the second and third trials of each task were used in the subsequent analyses.
For every elbow flexion angle, the results of the learning curve assessment using repeated measures ANOVA, variation coefficients, intraclass correlation coefficient, absolute difference in Newton, and ratio between dominant and nondominant side are given.

ANOVA: analysis of variance.
a p < 0.001.
b p < 0.01.
c p < 0.005.
The variation coefficients across all subjects ranged from 0.31 to 0.39 across the different elbow angles (Table 1). The measurement in 30 degrees of flexion had the lowest values with 0.31 and 0.32 for the nondominant and dominant sides, respectively. Measurements in 0 and 120 degrees of flexion had the highest values.
Test–retest reliability was calculated for 20 volunteers who repeated all tasks in a second session. The ICCs ranged from 0.86 to 0.96 in nondominant arms and from 0.89 to 0.97 in dominant arms (Table 1). The measurements in 30 degrees of flexion had the highest ICC.
For all elbow angles, extension forces were higher (ranging from 3.2 N to 6.9 N) for the dominant arm compared to the nondominant arm. These differences were significant for all measurements except in 90 degrees of flexion. The ratio produced by this difference indicates that the dominant side has a positive ratio of 1.01–1.06, compared to the nondominant side during all elbow extension tests (Table 1). The influence of elbow flexion on triceps brachii force is depicted in Figure 2. Repeated measures ANOVA showed significant differences between all positions (p < 0.001), except for the difference between 60 and 90 degrees of flexion (p = 0.75).
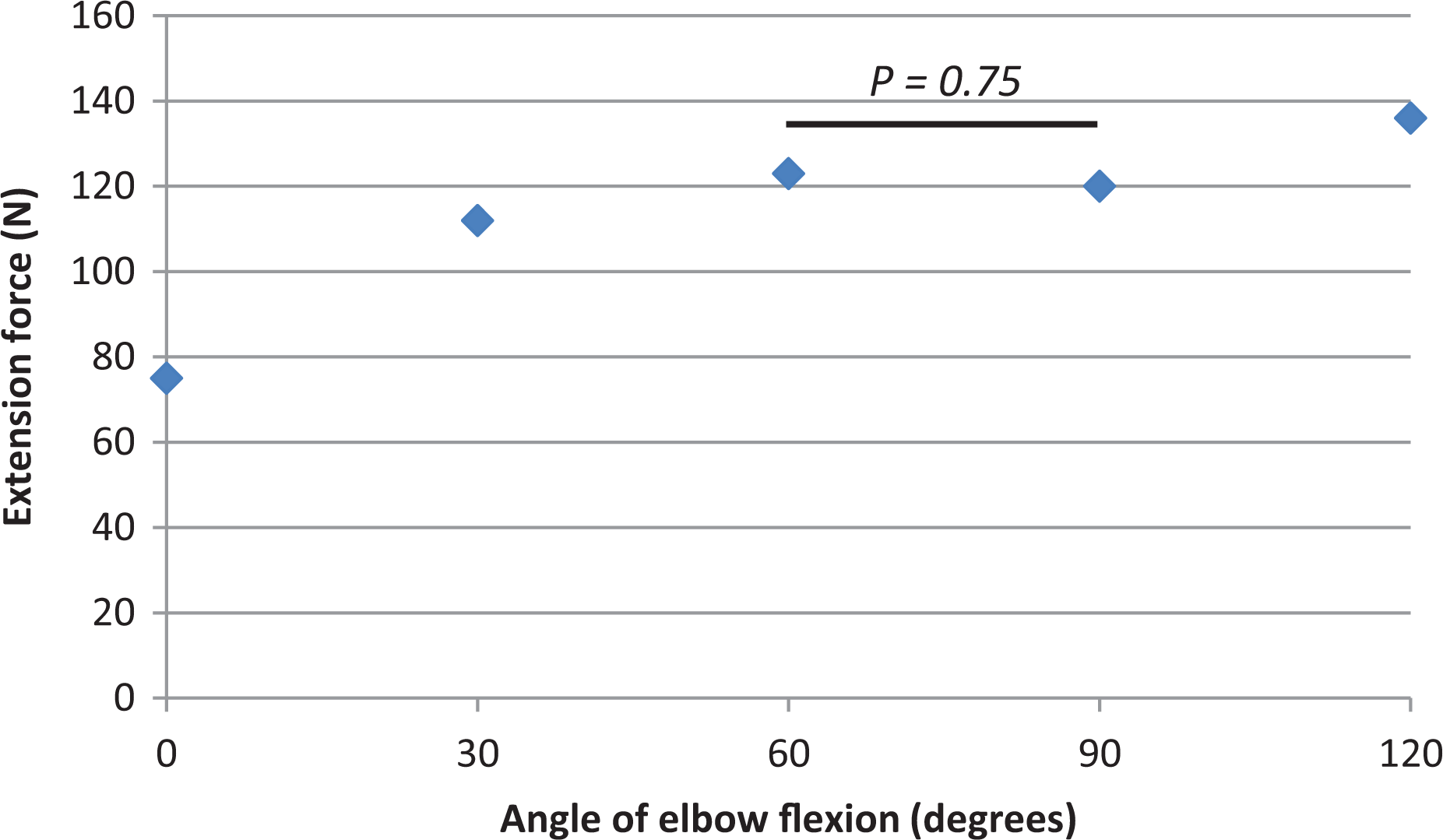
Repeated measures ANOVA for all tested angles. Significant differences between all positions (p < 0.001), except for the difference between 60 degrees of flexion and 90 degrees of flexion (p = 0.75). ANOVA: analysis of variance.
Discussion
This study shows that isometric triceps brachii force of healthy volunteers can be most accurately and consistently measured using a handheld dynamometer in 30 degrees of elbow flexion. This position has the lowest coefficients of variation and highest ICCs. The dominant arm provides 2% more extension force in this position than the nondominant arm.
In the literature, the extension force of the triceps brachii is usually tested in 90 degrees of elbow flexion. 3,14,17 –21 However, we found this position less reliable than 30 degrees of elbow flexion.
The measurements in 30, 60, and 90 degrees of flexion can be performed in a sitting position, which is most comfortable. In accordance with the previous research by Pinter et al., the flexion angles of 60° and 90° exhibit more force than 30 degrees of flexion. 19 Contradictory, in our study, most force was exerted in 120 degrees of flexion. However, overall it was shown that triceps force measurement in 30 degrees of elbow flexion is more reliable than the commonly used 90 degrees of flexion. The test–retest variation coefficients were excellent in all positions. 22 In the case of contracture of the elbow of more than 30 degrees, we advise to use an angle of 60 degrees of flexion as it has the second-best variation and ICCs.
In line with the study of Askew et al., we observed a ratio that favored the dominant arm in extension force. 17 We calculated a positive ratio of 1.01–1.06, depending on the amount of elbow flexion. In the same elbow flexion as in the study of Askew et al. (90°), our ratio was 1.01 compared to their ratio of 1.04. This ratio is helpful in unilateral conditions, that is, traumatic triceps brachii ruptures or triceps brachii-affecting surgery, as the “full recovery force” may be calculated from the contralateral arm, bearing in mind the dominant arm is stronger than the nondominant arm.
In cadaveric studies, the tensile strength resistance of repaired triceps brachii tendon appeared to be 17–60% of normal triceps brachii tendon, varying on the surgical approach. 23,24 Augmented repair using autologous flexor carpi radialis or hamstring tendons significantly increases tensile strength after triceps tendon repair yet provides more patient morbidity. 21 Mode of failure exists of loss of grip from the proximal sutures. 21,23,24 In practice, however, the testing of the triceps brachii will be performed in an outpatient setting several weeks after surgery, allowing the healing process to improve tensile strength resistance. We regard triceps brachii force testing safe when performed at least 6 weeks after surgery.
There are some limitations to our study. First, a multitude of muscle contractions might lead to fatigue and thus to erroneously lower measured force values. Our testing method requires five muscle contractions per arm per session. In literature, no signs of fatigue were seen with electric myographic activity monitoring up to five muscle contractions of the triceps brachii. 20 Therefore, we do not consider fatigue as a compromising factor in our study protocol. Second, we observed a learning curve during the data analysis. The first measurement was in almost all flexion angles significantly lower than the subsequent measurements. This effect was seen in isometric testing of hip flexors too. 16 Our data analysis thus excludes all the first measurements to correct for this learning curve. A “tryout measurement” for both arms could have minimized this phenomenon.
Furthermore, the 120° test was not possible with a wedge on the table. Some volunteers tried to push with their entire body and it was hard to instruct the subjects not to do this. Previous research already demonstrated that when measuring isometric force against an observer, the observer’s strength affects the values; stronger observers score higher force values. 18 This might have influenced the measurements in 120 degrees of flexion most, as the volunteer pushes against the observer who keeps the dynamometer in place. Variation in the amount of abduction of the upper arm to place it on the ramp does not interfere with the accuracy of the measurements. 19 When used clinically in patients with elbow disorders, not all patients will be able to extend the elbow to full extension. During the measurement in full elbow extension, the anconeus muscle may act as an elbow extensor because the line between origin and insertion lies posterior to the center of rotation of the elbow, up to 15% of the elbow extension force. 25,26
Concluding, the most reliable isometric triceps brachii muscle force measurement position using a dynamometer was at 30 degrees of flexion of the elbow. Test–retest reliability was excellent for both dominant and nondominant arms. A learning curve of one measurement was observed. Therefore, isometric force testing of the triceps brachii muscle is advised in 30 degrees of flexion of the elbow after one tryout session to diminish a learning curve effect. To assess full recovery, the ratio to the contralateral side of 1.02 can be used as a reference.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.