
Abstract
Purpose
The study aimed to describe the distal triceps brachii insertion on the olecranon and to correlate the findings with those seen in normal MR (Magnetic Resonance) anatomy of the triceps brachii insertion.
Materials and methods
14 un-paired fresh frozen elbows were included according to the institution guidelines and dissected. Histologic examination was performed to the distal triceps brachii insertion. The dimension of the distal triceps brachii tendon insertion was measured and defined based on its layer. The measurement of distal triceps brachii insertion was performed with image processing program (Image J, National Institute of Health, Bethesda, Maryland). T1-weighted elbow MR images (3.0 T) of a 102 patients were acquired and analyzed according to its sagittal plane.
Results
All specimens shows that distal triceps brachii tendon is with three distinct insertional areas in the olecranon which are: (1) capsular, (2) deep muscular, (3) superficial tendinous insertion with the areas of 80.7 mm2, 56.4 mm2, and 175.2 mm2, respectively. The superficial tendinous insertion was observed with a thickened portion, the “central cord” with 0.5 occupation ratio. MR analysis showed that 30% (31/102) of the distal biceps brachii insertion was with a cleft between the bipartite insertion of the superficial tendinous and the deep muscular insertion on olecranon which designated as the “lacuna” which was also found in 35% (5/14) of the specimens.
Conclusions
The distal triceps brachii has three distinct insertion on the olecranon. The superficial tendinous layer was separated with the deep muscular layer by a cleft in one third of the cases. Knowledge of this anatomy will help surgeon to understand the partial triceps injury and to avoid iatrogenic injury to the distal triceps tendon during surgery.
Introduction
The distal triceps brachii tendon has been investigated regarding its anatomy1–6 and imaging.7,8 Once rarely reported, the injury of distal triceps tendon was described more in accordance to the current trends in sports activity. The triceps tendon injury occur as an indirect result of a strong eccentric contraction of the muscle which explain why the injury is more often found in the insertional part.
There were not many reported studies previously which make the distal triceps tendon injury often overlooked. The complex anatomy of the distal triceps itself without adequate description in the imaging literature may contribute to the underreporting of this lesion. In general, any tear involving more than 50% of the tendon structural integrity necessitate surgical repair. 9 For this reason, a complete understanding of the anatomy and imaging are needed for the accurate management of distal triceps brachii injury. Furthermore, besides distal triceps tendon injury, the knowledge of anatomy and imaging will be helpful when surgeon perform a surgical procedure related to the distal triceps brachii tendon which may encompasses the open reduction and fixation of a distal humerus, osteotomy of os olecranon, triceps tendon repair or reconstruction, and osteo-capsular arthroplasty (posterior compartment).
The purpose of the current study was to describe the distal triceps brachii insertion on the olecranon and to correlate the findings with those seen in normal MR (Magnetic Resonance) anatomy of the triceps brachii insertion.
Material and methods
Gross tissue preparation
Convenience sample of 14 fresh-frozen elbow specimens (spanning from the trans-humeral level to forearm) from deceased individuals (Korean ethnicity) were obtained from the Department of Anatomy at our institution. The IRB approval was issued prior to the study (IRB S2020-0978). All the specimen were examined and cleared from the evidence of prior surgery or injury to the elbow. The mean age of the individuals was 62.8 (range, 51–69 years). There were six male and eight female specimens. There were an equal number of right and left specimens (n = 7). The elbow specimens were stored at −25°C and thawed overnight at room temperature prior to the study. Each elbow were dissected from the skin and subcutaneous fat following a midline posterior skin incision in 90 degree of flexion. The brachial and antebrachial fascia was removed to allow the triceps muscle and tendon to be exposed. The ulnar nerve was freed from the medial head of the triceps tendon and off the cubital tunnel.
Footprint measurement
The triceps muscular portion were isolated from the medial and lateral intermuscular septum. Dissection were continued to separate the triceps muscle from the brachioradialis and wrist extensor to expose the deep portion of the triceps muscle. The deep portion of triceps muscle were reflected from the posterior aspect of the humerus while preserving the distal attachments. The posterior fat pad of the triceps tendon was removed to allow the detail observation of the distal triceps insertion. From this point, the dissection were carried out using surgical loupes (Mini Loupes ×2.5 Magnification, Keeler Ltd, Windsor, UK) and a no.15 surgical scalpel. The capsule was isolated by sharp dissection from proximal to the distal, revealing its insertion on the olecranon. The insertion of the capsule was photographed using a digital camera (Olympus OM-D E-M10 Mark II with a M. Zuiko ED 14–42 mm f/3.5–5.6 EZ lens; Olympus Corp, Tokyo, Japan) along with a ruler as a fixed reference. The image was then imported to an image processing program (ImageJ, version 1.43; National Institutes of Health, Bethesda, Maryland, USA)10,11 to allow footprint measurement. In the ImageJ software platform, a straight line was drawn along the ruler using the “straight line” tool to obtain a fixed scale of 10 mm as the calibration process. The corresponding footprint area was outlined using the “freehand selections” tool. The medio-lateral (width), proximo-distal (length) and cross-section of the selected area was measured using the “measure” tool. Following the capsule removal and footprint measurement, careful observation was performed to identify deep and superficial layers of the distal triceps tendon. The footprint measurement were performed for deep and superficial layers is a respective manner. All measurements were expressed up to 0.1 mm. The mean and standard deviation of the measurement were recorded.
Magnetic resonance imaging analysis
The MRI was collected from patients which were diagnosed with lateral epicondylitis, ulnar neuropathy, cubital tunnel syndrome and medial epicondylitis in the outpatient clinic without clinical evidence of having triceps muscle pathology. There were 167 patients with elbow MRI from March 2013 to August 2020. Exclusion were made to 29 patients for the absence of sagittal projection, 31 patients for the absence of T1 sequence and seven patients with MR performed outside from our institution. All MR examinations were performed on a 3.0-T MR unit with a dedicated elbow coil (Ingenia; Philips Medical Systems, Best, The Netherlands) in our institution. The elbow MR sequences were axial fat-suppressed T2-weighted, axial T1-weighted, coronal fat-suppressed T2-weighted, coronal T1-weighted, sagittal T2-weighted and sagittal T1-weighted. One physician assistant collected the MRI of the elbow using a medical imaging database. Four surgeons reviewed the elbow MR images independently, being blinded to the patient’s data. The evaluation were performed for the distinction of distal triceps tendon attachment on the olecranon. The greater sigmoid notch was served as the reference section representing the center of olecranon (Figure 1). The order of the MR images was randomly changed and re-evaluated after 4 weeks from the initial evaluation. A second evaluation was performed by the same group of surgeons. Sagittal MRI showing the section represent the center of olecranon which include the greater sigmoid.
Statistical assessment
Statistical analyses were performed with SPSS software (version 12, IBM; Armonk, NY, USA). The medio-lateral (width), proximo-distal (length) and cross-section of the footprint of each layer of distal triceps attachment were compared using one-way ANOVA test and Bonferroni post hoc analysis. The significance level was set at <0.05. The intra-observer and interobserver agreement for the MR analysis were evaluated with intraclass correlation coefficient (ICC) as described by Landis and Koch. 12 The ICC reported a value between 0.0 and 1.0, as follows: 0.01–0.20 for slight agreement; 0.21–0.40 for fair agreement; 0.41–0.60 for moderate agreement; 0.61–0.80 for substantial agreement; 0.81–0.99 for almost perfect agreement; and 1.00 for perfect agreement.
Results
Gross anatomy
All specimens shows that distal triceps brachii tendon is with three distinct insertional areas in the olecranon facet which are: (1) capsular, (2) deep muscular, (3) superficial tendinous insertion (Figure 2). In a respective order to the sagittal orientation, the capsular layer attached to the most ventral facet, the deep muscular layer attached to the middle facet and the superficial tendinous layer attached to the dorsal facet of the olecranon (Figure 3). There was a thickened portion at the center of the superficial tendon layer, namely, central cord (Figures 2 and 3). There was a bare area without soft tissue insertion between the deep muscular layer (middle facet) and the tendinous layer (dorsal facet) resembling a cleft (lacuna) (Figure 4) which was observed in four of 11 specimens (36.3%). The fresh frozen specimen of distal triceps brachii tendon with three distinct insertional areas which consist of (1) capsular, (2) deep muscular and (3) superficial tendinous insertion. (asterisks: central cord). The enface view of distal triceps brachii insertion on the olecranon facet showing the (1) capsular (black area), (2) deep muscular (blue area) and (3) superficial tendinous layer (red) in which the central cord was occupied (asterisks). The enface view of distal triceps brachii insertion on the olecranon facet showing the (1) capsular (red area), (2) deep muscular (blue area) and (3) superficial tendinous layer (intact). The area marked by dash line represent the cleft (lacuna).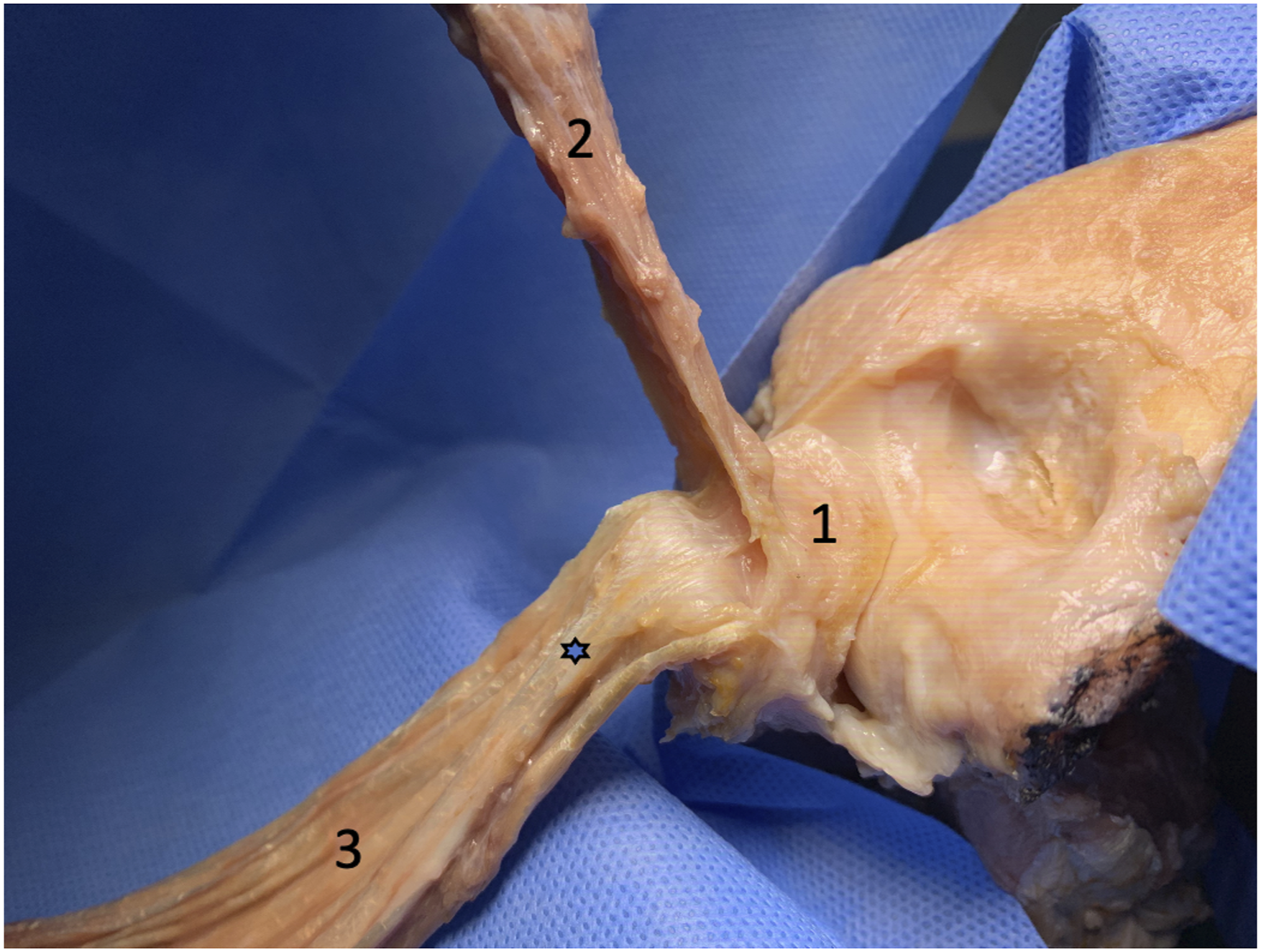


Footprint analysis
Footprint dimension.

Magnetic resonance imaging analysis
The mean age of the patients included in the MRI analysis was 51.6 years. The triceps muscle was inserted to the olecranon with three distinct layers (capsular layer, deep muscular layer and superficial tendon layer) which correspond to the gross anatomy finding of the specimen. The lacuna which was observed to be presented in 26.4% (mean) (Figure 5). The ICC for interobserver reliability for the incidence of lacuna for are 0.957 (95%CI, 0.941–0.970) for the first observation and 0.909 (95%CI, 0.829–0.936) for the second observation which implied for almost perfect agreement. The intraobserver reliability for the incidence of lacuna also showed almost perfect agreement (Table 2). MRI figure showing the presence of lacuna between the muscle layer and tendon layer. Intra-observer reliability.

Discussion
The footprint of distal triceps insertion has been reported in an inconsistent manner. 4 The current study showed that the distal triceps tendon is with consistent insertional footprint at the ventral, middle and dorsal facet of the olecranon. The dorsal facet was with the largest footprint which serve as the attachment of the superficial tendinous portion of distal triceps. The central cord, being the thickest part of the superficial tendinous portion occupied half of the dorsal facet of the olecranon. The study also observed a cleft between the deep muscular and superficial tendinous insertion which may have an association to the partial rupture of the distal triceps. The findings of the present study should be considered in the clinical practice.
First, the footprint of distal triceps is distinctly separated with three layers. The finding was suggested in previous study that three distinct insertional areas were found in the olecranon corresponding to the posterior capsular insertion, the deep muscular portion, and the superficial tendinous portion of the triceps with areas of 1.5, 1.2, and 2.8 cm2, respectively. 2 The largest portion was in the tendinous portion and the smallest was in the muscular insertion that were the same result in our study. Recently, arthroscopic capsular release for the management of stiff elbow has been widely performed. Surgeon had to release the posterior capsule to improve the flexion of the elbow without the clear reference when to stop and the risk of the iatrogenic damage of triceps muscle and tendon has been existed. Our recommendation for the posterior capsular release based on our finding is that the surgeon start release the capsule from the insertion site first with the insertional length of 6–7 mm as the reference and stop until the muscular part was exposed.
Second, we found the that there was a space between the deep and superficial layer (the lacuna) which presented higher (36.3%) at the specimens evaluation compare to those at the MRI evaluation (26.4%). Previous study from Akamatsu et al. 13 dissected 41 en-balmed elbow specimens and found a space at the distal triceps brachii tendon insertion. Belentani et al. 7 reported a split distal triceps insertion with an MRI observation which was not confirmed with histological evaluation. Celli 3 described the “triceps decussation” as a discrete interval between the lateral triceps expansion and medial triceps tendon and showed a bipartite distal triceps insertion on MRI observation. Regarding the result in the current study, due to its nature as a cross-sectional evaluation, it was not clear whether the lacuna represent a pathologic condition (such as partial thickness tear) or normal variation. Theoretically, it could be explained that the degeneration process may contribute because the mean age of the specimens was older (62.8 years) compare to patients with MRI evaluation (51.6 years). In an asymptomatic individuals, the overall prevalence of partial thickness rotator cuff tear was 4% in patients under the age of 40 and increase to 26% in patients over the age of 60. 14 Intrinsic changes within tendon has been observed at the partial thickness rotator cuff tears especially in areas with relative avascularity which correlate with tendinopathies. 15 In view of this, we postulate that the lacuna may indicate a partial thickness tear resulted from degeneration process of the triceps tendon insertion. Further longitudinal study is required to confirm the correlation between clinical finding and serial radiographic changes. Other possible explanation for the lacuna was that the different origin of lateral and medial head of triceps tendon might create different resultant of force continuously which resulted in the cleft observed between the deep muscular layer and the superficial tendon layer. Barco et al. 2 described the correlation the distal insertion with the origin of triceps based on their observation that the deep muscular head corresponded to the medial head of the triceps and the tendinous portion corresponded to the long and lateral heads and correlated with the height of the specimen. Future biomechanical investigation is necessary to confirm this postulation with the clinical correlation.
Third, the thickest part of tendinous of the distal triceps that was described as ‘central cord’ in our study was observed in all specimens. Despite the lack of biomechanical study for the role of the central cord in this study, the central cord was observed as the most robust anatomical structure for the elbow extension thus may play the dominant role in elbow extension mechanism. The clinical translation of this finding can be apply in the surgical approach for distal humerus, several recommendations have been included such as triceps split, triceps tongue and triceps reflecting. Based on the finding of the current study, we would like to favor the triceps sparing approach as to preserve the central cord in the premise of avoiding triceps insufficiency.
Strength and limitations
The study is not without limitations. The study was with small number of specimens with the average age of 62.4 years which may limit the translation to younger population. The data measured from the gross anatomy study and MRI include different patients which prevent a direct association. The footprint area data in this study were not normalized with the individual anthropometric measures. Therefore, there is a possibility of data variation depending on the size of individual measures. Despite that, the study include MRI of a living subject as the advanced imaging analysis with the participation of multiple evaluators in the determination of interobserver reliability. The footprint area was not measured in the MRI study because the traditional measurement on tendon insertion is calculated by the longest length x width which may underestimate the accurate 3-D structure of its actual insertion area. The lack of histological evaluation also prevent us to delineate the capsule, tendon and muscular part of the distal triceps tendon. However, this is inevitable because the anatomy study include detachment of the tissue from the bone which hinder the histological evaluation. Despite the above mentioned limitations, the information provided in this study may help to elucidate the previous conflict about the diagnosis of partial tears of distal triceps tendon as to avoid misdiagnosis the lacuna as an artefact or vice versa.
Conclusion
The distal triceps brachii has three distinct insertion on the olecranon. The superficial tendinous layer was separated with the deep muscular layer by a cleft in one third of the cases. Knowledge of this anatomy will be beneficial as to avoid iatrogenic injury to the triceps insertion when performing elbow surgery, to understand the partial triceps injury and to opt for an optimal surgical approach in elbow surgery.
Footnotes
Author’s note
This investigation was performed at Asan Medical Center, Seoul, Republic of Korea.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by EMBRI Grants 2021-EMBRI-SN-0008 from the Eulji University.