
Abstract
Introduction:
Anatomic repair of the anterior talofibular ligament (ATFL) is challenging when the local ligamentous tissue is severely attenuated. Anatomic reconstruction of the ATFL with tibial tuberosity–patellar tendon (TT-PT) autograft is a feasible choice that can avoid the complicated tendon–bone healing and restore ankle stability.
Materials and methods:
From 2009 to 2015, 31 chronic lateral ankle instability (CLAI) patients (31 ankles), who had a serious injury on the ATFL only, were treated with anatomic reconstruction of ATFL with TT-PT. American orthopedic foot and ankle society ankle–hindfoot score (AHS), visual analog scale for pain score (VAS), Karlsson–Peterson score, Tegner activity level, and objective examination comprehending range of motion were used to evaluate the clinical outcomes before and after operation. Radiographically, talar tilt angles and anterior drawer were assessed in pre- and postoperative ankle stress views.
Results:
Among the 31 ankles, 17 ankles with single-bundle ATFL and 14 ankles with double-bundle ATFL were found at operation. At a mean follow-up of 42 months (24–82 months), all patients were satisfied with the procedure. Mean AHS significantly increased from 60.5 ± 8.2 to 93.5 ± 4.8. Mean Karlsson–Peterson score significantly increased from 55.2 ± 11.0 preoperatively to 91.2 ± 6.9 at final follow-up. Average VAS significantly decreased from 5.9 ± 1.6 preoperatively to 1.4 ± 1.0 at the latest follow-up. Mean Tegner activity level was 3.7 ± 0.9 before operation, compared with 7.0 ± 0.8 after operation. On stress radiographs, mean talar tilt angle was 17.0 ± 3.4° before operation and 3.8 ± 2.1° at the latest follow-up. In addition, mean anterior tibiotalar translation was 7.5 ± 2.2 mm before operation and 1.8 ± 1.1 mm at the latest follow-up.
Conclusion:
Anatomic reconstruction of the ATFL using a TT-PT autograft allows bone–bone healing in talus and tendon–tendon/periosteum healing in fibula rather than requiring tendon–bone healing, which is an alternative choice for treating CLAI caused by single ATFL insufficiency.
Keywords
Introduction
Lateral ankle sprains are one of the most common lower extremity injuries in sports. 1,2 A majority of patients recover without significant long-term consequences, but about 20% of patients with a first-time ankle sprain will develop chronic lateral ankle instability (CLAI). 3,4 The patients with CLAI usually suffer recurrent ankle sprains, pain with routine activity, and even difficulty in walking. 1,5,6 The development of CLAI mainly ascribed to the injuries of lateral ankle ligaments which generally occurred during forefoot adduction, hindfoot inversion, and tibial external rotation with the ankle in plantar flexion. 7 –9 Anatomically, lateral ankle ligaments are made up of anterior talofibular ligaments (ATFLs), calcaneofibular ligaments (CFLs), and posterior talofibular ligaments, which function synergistically to provide lateral ankle stability. 7,10 Among them, the ATFL is the most vulnerable ligament in lateral ankle sprains. 7,8,11,12 Clinically, the conservative treatment, such as peroneal muscle strengthening, balance reflex training, and external bracing to prevent recurrent injury, was an available protocol for the injuries of the lateral ankle ligaments, but some patients who follow these nonoperative regimens have no effects. 10,12,13 In these patients, surgical repair or reconstruction may be indicated.
Many surgical procedures have been used to treat CLAI with variable success. 10,14 The Broström technique is a classical procedure for CLAI patients, which directly and anatomically sutures the torn ends of the lateral ligaments in patients. 15 About 80% of patients do well with the Broström procedure. However, there remains a subset of patients who continue to experience recurrent ankle instability and generalized joint hypermobility. 13,16,17 Thus, some modified Broström techniques were described to overcome the shortcomings of the Broström technique through tenodesis or suturing of the lateral extensor retinaculum to the anterior distal end of the fibula. 18 –22 However, some operative procedures may damage the anatomy of lateral ankle ligaments, and then interfere with the normal kinematics of the ankle–hindfoot joint. 18,19 Moreover, the Broström procedure and its modifications were challenging when the local ligamentous tissue was severely attenuated and insufficient. 16,17,23 Therefore, in these circumstances, some reconstruction techniques utilizing an autograft or allograft tendon were performed to replicate the anatomic positions of the origin and insertion sites of lateral ankle ligaments, which can not only restore normal resistance to anterior translation and inversion without restricting ankle motion but also be suitable for the revision of failed Broström repair. 24 –26 However, most techniques in the literature cannot avoid the slow and complicated healing process between bone tunnel and graft tendon 27 –30 and never take the individual anatomic variations in ATFL into consideration. 7,8,31
In this study, based on previous reported cadaveric studies and the individual’s specific anatomy, 7,8,31 we described a new surgical technique to reconstruct the ATFL as anatomically as possible for those CLAI patients who only had a serious injury on the ATFL. Specifically, this technique involved anatomic reconstruction of the ATFL with tibial tuberosity–patellar tendon (TT-PT) autograft, as well as bone–bone healing in the talus and tendon–tendon healing in the fibula instead of the sophisticated tendon–bone healing. This technique restores ankle anatomy and preserves joint mechanics. The purpose of this study was to determine the clinical results of this approach to reconstructive surgery.
Materials and methods
This study was approved by a local Institutional Clinical Ethics Review Board. From February 1, 2009 to June 28, 2015, CLAI patients who had an established diagnosis based on clinical and radiographic features were eligible to participate in this clinical study. At last, 31 CLAI patients (31 ankles), who had prior informed consent to participate in the study, were treated with our surgical technique and followed up for at least 2 years. Pre- and postoperative records, radiographs, and operative notes were reviewed; moreover, functional statuses and radiographic parameters were prospectively assessed.
Inclusion criteria for single ATFL reconstruction
The inclusion criteria for our surgical procedure were CLAI of at least 3-month duration with repeated episodes of recurrent inversion sprain and evidence of lateral ankle instability by clinical (patient history and physical examination) and stress radiographic (significant ankle laxity with a 10° difference in talar tilt angle when compared with the opposite side or an absolute talar tilt angle 15°) evaluations that failed to respond to peroneal strengthening and proprioceptive training. The stress radiographic evaluation included talar tilt stress radiographs and anterior talar displacement radiographs using a Telos machine (model SE 2000; Telos GmbH, Marburg, Germany) set at 150 N of stress force. Our surgical procedure was also indicated for CLAI patients with generalized ligament hyperlaxity or for those who had failed the Broström procedure and its modifications. Additionally, patients with high-demand activities or a body mass index greater than 30 kg/m2 were also indicated. Young people, strenuous workers, or athletes were favored for surgery. But more importantly, to eliminate interference factors of our study, the patients with the insufficiency of both ATFL and CFL were excluded during the intraoperative evaluation of the lateral ankle ligaments. Furthermore, we excluded the cases of combined rheumatoid arthritis or grade II or more of ankle degenerative arthritis according to the radiographic classification. 16,32 In addition, the patients with some surgery or trauma on the graft donor knee were also not indicated for our surgery.
Patients
All patients had not suffered any surgery or trauma on the graft donor knee. Of the 60 CLAI patients, 5 patients who declined to participate in current study, 8 patients who were confirmed of the insufficiency of both ATFL and CFL during the intraoperative evaluation, 11 patients with torn ATFL with healthy margins who were cured with the Broström procedure, and 5 patients who had returned for follow-up evaluation less than 2 years were excluded from the final analysis. Therefore, 31 patients (31 ankles) who had undergone complete preoperative evaluation and been followed for a minimum of 2 years were included in the present study. The patients included 11 women and 20 men, the ages of whom, at the time of surgery, ranged from 16 years to 52 years (mean, 33.1 ± 9.4 years). The left ankle was involved in 18 cases and the right ankle in 13 cases. Four patients failed a previous Broström procedure, and two patients underwent arthroscopic ankle debridement with removal of loose bodies during our surgery.
Operative technique
The surgery was performed with the patients under general anesthesia. Ankle arthroscopy was firstly performed under noninvasive distraction to assess and address the concurrent intra-articular pathological changes. If the patients had anterior impingement exostosis, arthroscopic resection was performed. 33 According to the modified version of the Pritsch classification, 34 if there was a grade I or grade II osteochondral lesion, it was treated with debridement. In patients with grade III or IV osteochondral lesions, the lesion was treated with microfracture. 35 In addition, the osteophytes, impinged soft tissue, synovitis, and fibrous tissue adherent to the lateral gutter as well as the loose bodies were removed by ankle arthroscopy. 35 Generally, no tourniquet control was used before beginning the open portion of the procedure.
Anatomical reconstruction of the ATFL was performed after the arthroscopic procedure with a thigh tourniquet. To facilitate the follow-up operative procedure, a 12-cm extended U-shaped incision was centered over the tip of the fibula and extended anteriorly over the lateral talus and posteriorly over the lateral calcaneus and posterior border of the fibula (Figure 1). ATFL and CFL were carefully dissected without damage to the lateral cutaneous branch of the superficial peroneal nerve and sural nerve, and then its condition was evaluated by intraoperative findings together with preoperative MRI. If there was confirmation of torn ligaments with healthy margins, the Broström procedure was performed. 15 If severe attenuation of the ATFL and CFL stump was found during the operation, the lateral ankle ligaments were reconstructed with a semitendinosus autograft. 13 If the CLAI patients had single ATFL insufficiency with poor quality for the Broström procedure, central third TT-PT autograft was harvested from the ipsilateral knee for ATFL reconstruction.

U-shaped skin incision. The black solid line indicates the operative skin incision and the red dotted line indicates the sural nerve.
In order to avoid the injury of the infrapatellar nerve(s), we made a 4-cm longitudinal incision on the distal half of the patellar tendon, 36,37 and a mid-third patellar tendon with 40-mm length, 10-mm width, and 1.2-mm thickness was harvested with a rectangle bone block from the tibial tuberosity. 8 The rectangle bone block was about 10-mm length, 10-mm width, and 8-mm thickness. In patients with single-banded ATFL, only the tendon part of the harvested graft was split with a width of 6 mm and 4 mm, and the surface of the attached bone block was smoothed (Figure 2(a)). 7,8 If there was a double-banded (superior and inferior) ATFL, the patellar tendon–tibial tuberosity graft was separated into two bundles by a width of 6 mm and 4 mm, and the attached bone block was also split into two bone blocks with a size of 10 × 6 × 8 mm3 and 10 × 4 × 8 mm3 (Figure 2(a)). 7,8 And then, the ends of the split patellar tendon grafts were sutured over a length of 15 mm by a whip stitch using #2 Ticron suture (Tyco Healthcare Syneture, Norwalk, Connecticut, USA) (Figure 2(a)).

(a) The patellar tendon was harvested with a bone block from the tibial tuberosity, and the tibial tuberosity–patellar tendon graft was prepared on the basis of individual’s specific anatomy of ATFL. (b) According to individual’s specific anatomy of ATFL, one or two grooves were made on the talus insertion of ATFL. The close-up views showing the size of the talus groove(s). (c) The suture anchor was inserted into the bottom of talar groove(s) to fixate the graft(s). ATFL: anterior talofibular ligament.
The fibrocartilage of the ATFL insertion on the talus was removed (Figure 2(b)), two anchors were inserted into the groove(s) of talus created by removing the fibrocartilage and subchondral bone, and the bone block of the graft was anatomically fixed on the groove with suture anchor (TwinFix 3.5 Titanium, Smith & Nephew Endoscopy, Andover, Massachusetts, USA) (Figure 2(c)). Two evenly spaced tunnels (diameter: 3.5 and 2.5 mm, respectively) were predrilled at the superior and lower edge of the ATFL footprint where the ATFL inserted into the fibula with 3.5- or 2.5-mm Kirschner wires (Figure 3). 8 Based on an autopsy study and individual’s specific anatomy of ATFL, the angle between the drilled bone tunnel and the long axis of the fibula was set to approximately 89 ± 11° (on the right) and 86 ± 8° (on the left). 7 A wire was used to facilitate the passage of the grafts through the bone tunnel. The tendon ends of the TT-PT grafts were respectively passed through the two predrilled bone tunnels in the distal fibula, and then securely and tensely tied and sutured together with 2-0 absorbable PDS II suture (Ethicon, Edinburgh, UK) at the exit holes of bone tunnels with the ankle in neutral position, with an approximately 30-N tension force manually applied to both threads, so that tension could be applied to the tendon grafts. 10 At last, the remnant of the tied tendon grafts was firmly sutured to the periosteum around the exit holes of bone tunnels with 2-0 bioabsorbable suture (Coated Vicryl, Ethicon, Inc., Somerville, New Jersey, USA) to strengthen the fixation site (Figure 4). The inversion stress and anterior drawer tests were used to check the stability and range of motion of the ankle as well as the strength of the reconstructed ligament before closing surgical incision. After closing the operative wounds in layers, the ankle was immobilized by a short leg cast in neutral position.
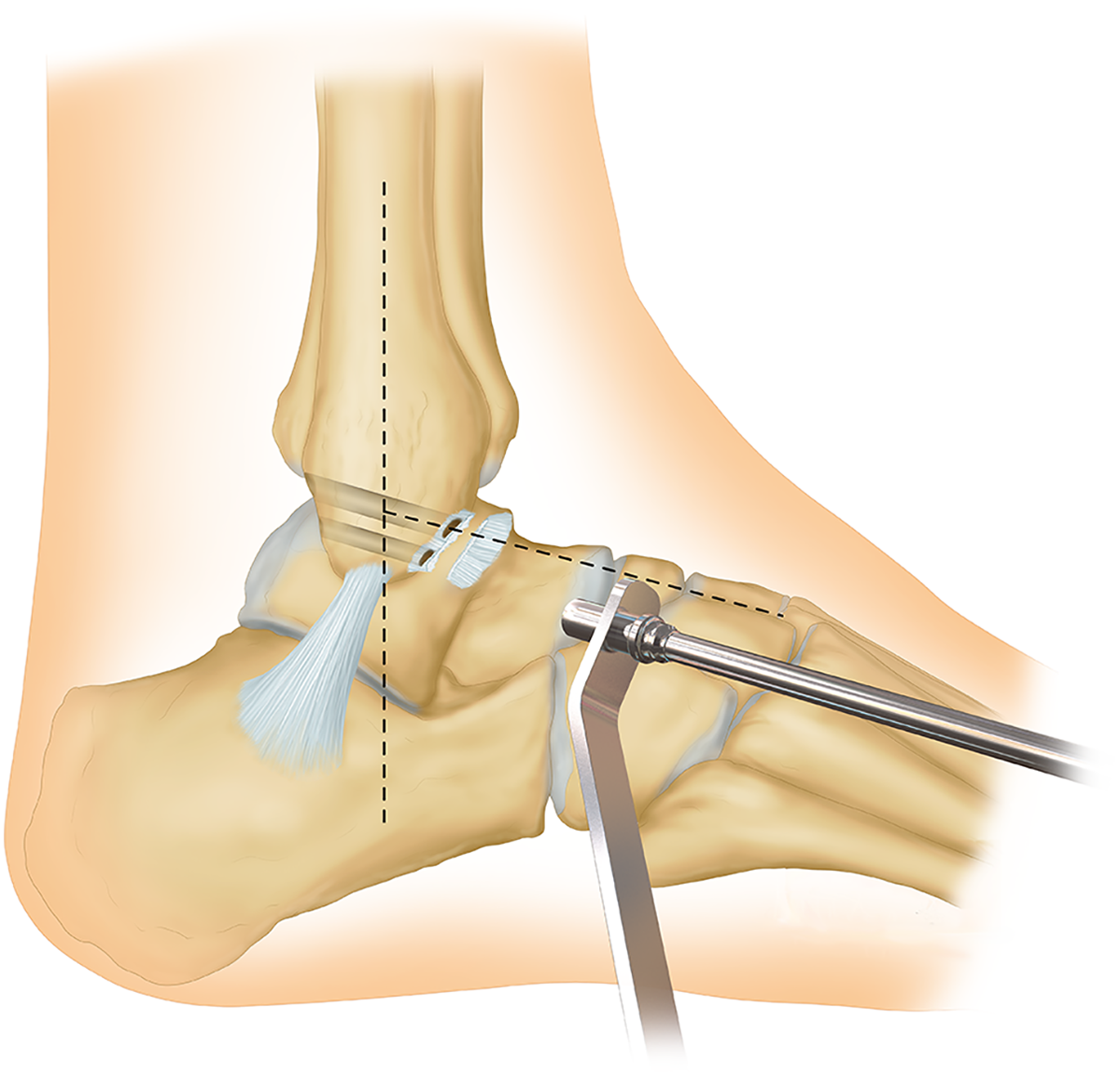
Two evenly spaced tunnels with a diameter of 3.5 and 2.5 mm were predrilled at the superior and lower edge of the ATFL footprint where the ATFL inserted into the fibula. ATFL: anterior talofibular ligament.

Bone block(s) of the tibial tuberosity–patellar tendon graft were firmly and anatomically fixated on the talus groove(s) at the talar neck of the ATFL footprint(s) with a suture anchor, and two tendon ends of the tibial tuberosity–patellar tendon graft were respectively passed through the two predrilled bone tunnels in the distal fibula. Under the tension force of about 30 N manually applied on the tendon grafts, two tendon ends of the tibial tuberosity–patellar tendon graft were securely and tensely tied and sutured together at the exit holes of bone tunnels with the ankle in the neutral position, and then firmly sutured to the periosteum around the exit holes of bone tunnels to strengthen the fixation site. The close-up view showing the completed way of the suture and fixation in the distal fibula. ATFL: anterior talofibular ligament.
Rehabilitation
Postoperatively, the ankle was immobilized in a neutral position with a short leg cast. Rehabilitative exercises including isometric contraction of muscles around the ankle were initiated at the day after the operation. Two weeks after surgery, the operative sutures were removed, and partial weight-bearing was allowed while the cast was still on the ankle. Four weeks after the surgery, the cast was changed to soft ankle orthosis and active range of motion was allowed. Gradually, full weight-bearing was allowed. Eight weeks after the surgery, the patient transitioned to a normal shoe with a brace, and formal physical therapy was initiated. Three months after the surgery, jogging was allowed, and brace was abandoned. At 6 months, a full range of sports activities was allowed.
Clinical assessment
Postoperatively, 31 patients were successfully contacted and returned for a final follow-up examination at a median of 43 months (24–82 months). At the final follow-up examination, patients were asked to fill out four postoperative questionnaires (visual analog scale for pain score (VAS), American orthopedic foot and ankle society ankle–hindfoot score (AHS), Karlsson–Peterson ankle score, Tegner activity level and satisfaction). A 10-point VAS scale was used to rate the current pain levels of patients, and AHS and Karlsson–Peterson scores were elected as the primary outcome measurement for assessing this ankle surgery. Patients were also asked to rate their overall satisfaction with their surgical results as dissatisfied, fair, satisfied, or very satisfied. Additionally, ranges of movement of ankles (plantar flexion and dorsiflexion) and of subtalar joints (eversion and inversion) were physically examined before surgery and at latest follow-up by two of the same orthopedic surgeons using a standard goniometer.
Radiologically, talar tilt angles on varus stress views and anterior talar displacement (defined as the distance between the anteroinferior margin of distal tibia and the anterosuperior tip of the talar head as determined by the anterior drawer test) were measured and compared with preoperative radiographs. 38 Three orthopedic surgeons individually measured the radiographic value using a picture archiving and communication system (GE Healthcare, Mt. Prospect, Illinois, USA) workstation and then calculated the average values.
Statistical analysis
Statistical analysis was performed using the SPSS software (version 17.0, SPSS Inc., Chicago, Illinois, USA). VAS pain score, AHS value, Karlsson–Peterson score, Tegner activity level, radiographic anterior talar displacement, and varus talar tilt angle were presented as the mean ± standard deviation. Additionally, differences of VAS pain score, AHS value, Karlsson–Peterson score, Tegner activity level, radiographic anterior talar displacement, and varus talar tilt angle before operation and at the latest follow-up were evaluated using paired t-test, with statistical significance established at p < 0.05.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Results
Among the 31 patients, 19 patients were treated by reconstructing the ATFL with one-bundle grafts. The patients included 8 women and 11 men, the ages of whom, at the time of surgery, ranged from 19 years to 52 years (mean, 32.6 ± 9.7 years). The remaining 12 patients were treated by reconstructing the ATFL with two-bundle grafts. The patients included 4 women and 8 men, the ages of whom, at the time of surgery, ranged from 16 years to 45 years (mean, 34.3 ± 9.2 years). Additionally, based on the arthroscopic findings, 7 cases of anterior impingement exostosis, 13 cases of osteochondral lesions of the talar dome, and 23 cases of ankle synovitis were found among the 31 ankles, which were dealt with the arthroscopic technique. After operation, 27 patients (87%) were very satisfied with the results of our reconstruction technique, 7 patients (13%) were satisfied with the results, and no patients experienced any symptoms of swelling, giving way and recurrences of lateral ankle instability.
Clinical assessment
A total of 23 patients were followed up for a mean of 41 months (range 24–73 months). In comparison with preoperative values, significant differences were found in the VAS, AHS, Karlsson–Peterson scores, and Tegner activity level (Table 1). Additionally, the mean ranges of ankle inversion were significantly decreased, while the mean ranges of ankle movement in the others plane showed no significant difference between preoperative testing and the latest follow-up testing (Table 1). The mean preoperative VAS pain score was 5.9 ± 1.6 points (range 4–9 points), and this score significantly decreased to 1.4 ± 1.0 points (range 0–3 points) at the final follow-up (p < 0.05). Meanwhile, the AHS score significantly increased from 60.5 ± 8.2 at the preoperative assessment to 93.5 ± 4.8 at the latest follow-up assessment (p < 0.05). Similarly, the Karlsson–Peterson score significantly increased from 55.2 ± 11.0 at the preoperative assessment to 91.2 ± 6.9 at the latest follow-up assessment (p < 0.05). Additionally, the Tegner activity level was 7.0 ± 0.8 in operated ankle, compared with 3.7 ± 0.9 in the non-operated ankle (p < 0.05).
Results of anatomic ATFL reconstruction with TT-PT for CLAI (mean ± standard deviation).

AHS: American orthopedic foot and ankle society ankle–hindfoot score; VAS: visual analog scale for pain score; ATFL: anterior talofibular ligament; TT-PT: tibial tuberosity–patellar tendon; CLAI: chronic lateral ankle instability.
Radiographic assessment
According to stress radiographs, the mean talar tilt angle decreased significantly from 17.0 ± 3.4° preoperatively to 3.8 ± 2.1° at the final follow-up (p < 0.05) (Table 1 and Figure 5). Meanwhile, the average anterior tibiotalar translation was significantly increased from 7.5 ± 2.2 mm preoperatively to 1.8 ± 1.1 at the final follow-up (p < 0.05).

Standard stress talar tilt angle of the right ankle at the preoperative radiograph and the final follow-up radiograph. (a) Preoperative stress radiograph of the right ankle demonstrating 16° of talar tilt with inversion stress testing. (b) Postoperative stress radiograph of the right ankle showing reduction of the inversion talar tilt to 3°. The red arrows in the distal-central fibula correspond to the fibular tunnels created during reconstruction.
Postoperative complication
Four patients experienced postoperative complications. Two patients developed a local infection of the surgical incision with skin sloughing, which resolved with local wound care and oral antibiotics. Two patients had donor site-related problems caused by the injury of infrapatellar nerve(s) in the process of harvesting the TT-PT grafts. 37 After conservative treatment, the donor site-related problems of those patients were gradually resolved.
Discussion
Many reconstruction techniques have been introduced for treating CLAI, but no techniques have taken the complicated tendon–bone healing into consideration. This study described a novel reconstruction technique for those CLAI patients with single ATFL injury, which involves anatomic reconstruction of the ATFL using mid-third TT-PT autograft. The principal findings of the current study were that the described technique could achieve anatomic reconstruction of ATFL, and moreover allow bone–bone healing in the talus and tendon–tendon healing in the fibula rather than requiring complicated tendon–bone healing.
Repair or reconstructive surgeries for CLAI were typically divided into anatomic or nonanatomic. 13 In the past, nonanatomical reconstruction methods such as tenodesis, including Evans, Chrisman, and Snook, and Watson-Jones, were widely used procedures for lateral ankle instability with variable success. 10,19,39,40 Those procedures sacrifice normal tissue, and the reconstructed ligaments are far from anatomic, resulting in limited joint motion and altering the kinematics, which may later cause degenerative disease in ankles, including chronic ankle pain, increase in postoperative osteoarthritis, recurrence of instability, and changes in both dynamic and static plantar pressure distribution. 41 –44 Anatomical reconstruction of the lateral ankle ligaments can avoid the restriction of the range of ankle motion and effectively reduce the long-term risk of osteoarthritis and/or chronic pain; thus, it becomes more and more popular for treating ankle lateral instability in recent years. 13,45 –47 The Broström techniques were the common anatomic repair surgery of ankle instability, and favorable outcomes have been reported with radiological evidence of improved lateral ankle stability. 13,19 But some patients lack the necessary amount of local ligament tissue or the healthy margin of the torn ligament. 15 In this situation, it is difficult to repair or reconstruct the torn ligament with local ligament tissues. Besides, residual mechanical instability after the Broström procedure often occurred in patients with a history of long-standing instability and generalized joint laxity. 19,22,46,48 Therefore, the Broström procedure was modified for those patients, which involves in suturing of the inferior extensor retinaculum to the anterior distal end of the lateral malleolus. 18,19 However, some procedures of the modified Broström surgery may change the normal kinematics of the ankle–hindfoot joint; thus, it may increase the incidence of long-term ankle degeneration. 10,13,14,21 In recent years, many reconstruction techniques of the lateral ankle ligaments based on detailed anatomic study or isometry of the ligaments have been introduced that utilize synthetic carbon fiber and autograft/allograft tendon. 13,14,49 Those procedures have advantages of lower incidence of postoperative arthrofibrosis and reduced postoperative complications; however, their disadvantages include technical difficulty in recovering the lateral ankle ligaments anatomically, difficult healing between tendon graft and bone interface, and questionable stability of tendon graft–bone fixation. 10,13,14,19,25,49,50
To avoid those limitations, we designed a new surgical procedure for anatomic reconstruction of ATFL according to previous reported cadaveric studies and the individual’s specific anatomy by meticulous dissection. 7,8,31 Compared with the procedures designed for treating CLAI with bone–patellar tendon, 19 our procedures took more ATFL anatomic details into consideration and were only suitable for single ATFL reconstruction. During our surgical procedures, the bundle and footprint position of the reconstructed ATFL and the bone groove for graft fixation were on the basis of the detailed morphology of the ATFL 7,8,31 ; thus, it provided reassurance to restore the ATFL anatomically. In the fixation site of the talar neck, two titanium suture anchors were used to fix the graft bone block(s) with the talar neck. A research launched in porcine cancellous bone shows that the failure load of this anchor can reach about 435 ± 52.1 N, in contrast with 138 ± 23.5 N for the human ATFL. 51,52 Thus, this titanium suture anchor has sufficient tensile strength for fixation of the ATFL. In addition, this fixation method at the talar neck can tactfully avoid slow and difficult tendon–bone healing; thus, it ensures quick and high-quality healing between the tibia block and the talar groove. Besides, it is possible to perform an MRI for the follow-up evaluation with a titanium suture anchor. In the fixation site of the distal fibula, the two split patellar tendons were respectively pulled across the predrilled tunnels in an anterior to posterior direction, and then the tendon ends were tightly sutured together at the posterior border of the fibula to bolt on the distal fibula while the ankle was in the neutral position, with an approximately 30-N tension force manually applied to both tendons, so that the tension of the graft could ensure the stability and isometry of lateral malleolus. 10 After that, the free end of the stitched tendons was tightly sutured to the posterior lateral fibular periosteum. By this fixation way, the healing process in the distal fibula involves tendon–tendon healing, tendon–periosteum healing as well as tendon–bone healing. According to previous studies, 53 the tendon–tendon and tendon–periosteum healing was faster and easier than tendon–bone healing, thus playing a major role for this fixation way at the early postoperative stage. Unlike published literature, no surgical materials, such as staple, screw, bone suture anchor, Endobutton, and interference screw, 10,54 –59 were applied to attach the tendon graft to bone tunnel in our procedures. This particular fixation could not only economize iatrical resource and reduce sanitary investment but also provide good ankle stability and enable the fibular fixation site to strongly and firmly repair as soon as possible.
Our results show that anatomic reconstruction of the ATFL with TT-PT results in radiographic stability and excellent clinical outcomes. In addition, all of the patients were satisfied with the results of this procedure. Although two patients suffered donor site-related problems caused by intraoperative injury to the infrapatellar nerve(s) in conjunction with patellar tendon harvest, they gradually relieved after conservative treatment. Furthermore, no loosening of the fixation site was observed at the distal fibula or talar neck after operation. Even so, it is important to stress that our surgical procedure is not available for the vast majority of CLAI patients. Several series have documented good results from an isolated or modified Broström procedure. 15,21,23 However, we used specific criteria to carefully select which patients underwent this surgical procedure in the current study. If there was confirmation of torn ligaments with healthy margins after assessment, the Broström procedure was performed to restore the lateral ankle ligaments. 15 If severe attenuation of the ATFL and CFL stump was found during the operation, the lateral ankle ligaments can be reconstructed with a semitendinosus autograft. 13 When the CLAI patients have single ATFL insufficiency with poor quality for Broström repair, ATFL reconstruction with TT-PT can be considered to restore ankle function and stability.
It is important to recognize the limitations of our study. Firstly, our results were based on a relatively small number of cases and that the follow-up period was relatively short, and thus, additional large-scale study is required with a long-term follow-up. Secondly, during our procedures, about 12-cm-long “U”-shaped incision was made on the lateral malleolus, which was relatively large and in contradiction with the prevailing trend of minimally invasive technology in medical surgery. 12,35,49 Thus, reducing the surgical trauma of this technique is an urgent need. Arthroscopic anatomical lateral ankle ligament repair/reconstruction, similar to knee and shoulder ligament surgery, 60,61 may be a way to decrease surgical wound in our procedure. Thirdly, our procedure was only near anatomic, because the TT-PT was designed for stress along an axis vertical to the floor whereas the ATFL acts at an axis oblique to the floor, so fibers of one may not be an anatomic replacement of the other. Fourthly, according to our selection criteria, only single ATFL injury with poor-quality ligament tissues was suitable for our reconstructive procedures, while a higher rate of combined injuries to the ATFL and CFL has been demonstrated in clinic. 10,13,14,16,19,25,50 So, this may limit the widespread application of our reconstructive procedures. In our opinion, despite the limitations of this technique, it remains an available option for anatomic reconstruction of ATFL, especially for the single ATFL injury without healthy ligament margins suitable for suturing.
In conclusion, anatomic reconstruction of the ATFL with TT-PT autograft achieves high patient satisfaction, improved ankle stability, and significant recovery of ankle function for those CLAI patients with single ATFL insufficiency with poor quality.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundamental Research Funds for the Central Universities of Central South University (2016zzts124) and Xiangya-PKU Weiming Research Fund (xywm2015I34).