
Abstract
Purpose:
To evaluate the role of fractures on pathologic bone in healing of proximal humerus unicameral bone cysts (UBCs) and investigate the clinical factors that affect healing of UBCs after fractures on pathologic bone.
Methods:
This prospective study was carried out between 2002 and 2014. We evaluated 56 patients with a UBC accompanying fractures on pathologic bone in the proximal humerus. Clinical data were collected from the patients’ medical records. Age, gender, degree of fracture displacement, location of cyst, and cyst size were investigated, and we assessed how these factors affected cyst healing.
Results:
The overall healing rate of UBCs 1 year after fracture was 66% (37 of 56 cases). The healing rate was significantly lower in pubescent patients (10–14 years old; 45%) than in those who were 9 years old (76%) or 15 years old (80%). The rate of healing of fractures in the metaphysis (53%) was lower than that of breaks in the diaphysis (85%). The mean cyst ratio was 1.31 in the 37 patients who experienced cyst healing within 1 year and 1.79 in the 19 patients who needed surgical treatment within 1 year.
Conclusion:
In latent lesions and in patients who are older (after puberty), UBCs of the humerus after fracture have better clinical results than do active lesions and those in younger patients (before puberty). Fractures on pathologic bone in proximal humerus UBCs often dramatically decrease cyst size, and patients with such fractures have excellent clinical results in terms of healing rate.
Introduction
Unicameral bone cysts (UBCs) are benign, fluid-filled cavities that are most often found in the metaphysis of long bones in children and adolescents, predominantly in the proximal humerus and femur. 1 On radiography, a UBC appears as a centrally located, lytic lesion with well-defined margins that often expands concentrically. The cyst wall is lined with a fibrous membrane and contains clear yellow, serous fluid. 2
The exact pathogenesis of these cystic lesions and fractures on pathologic bone is unclear. The most widely accepted theory is that a focal defect in metaphyseal remodeling blocks interstitial fluid drainage, leading to increased pressure from focal bone necrosis and accumulation of fluid. 3,4 So, paradoxically, UBCs may heal spontaneously after fractures via decompression of the cyst and induction of normal bone marrow inflow into the cyst.
About 75% of patients who have UBCs present with fractures on pathologic bone. 5 Thus, numerous treatment methods, such as percutaneous drilling, steroid injections, open curettage and bone grafting, placement of a cannulated screw to provide drainage, and partial or total resection, have been proposed. 6 –11 However, some recent studies have reported no difference in healing rate between cases of UBC with pathologic fractures and those without fractures in the proximal femur. 12,13
Therefore, the purposes of this study are to evaluate the role of fractures on pathologic bone in healing of proximal humerus UBCs and to investigate clinical factors that affect healing of UBCs after pathologic fractures.
Materials and methods
Patients
All clinical and radiological evaluations were approved by the Hospital Ethics Committee and Institutional Review Board of our institution (IRB no. CNUH-2017-05). Eighty-two patients with a UBC accompanying a fracture pathologic bone of the proximal humerus visited our outpatient clinic from January 2002 to December 2014. We excluded 11 cases who had a follow-up duration less than 1 year or a lack of clinical records and 15 patients who underwent surgical treatment within 2 months after fracture due to severe displacement over 1 cm on anteroposterior (AP) and lateral simple radiographic images or delayed healing of the fracture. Therefore, we finally enrolled and evaluated 56 of 82 patients.
We used the same treatment strategy for all patients. Initially, conservative treatment was done for 3–6 weeks with immobilization using long arm splint and arm sling until union of the fracture. For the first 2 weeks, long arm splint and arm sling were used together, and then only arm sling was used for immobilization. After fracture healing, we performed follow-up X-ray imaging at 1, 2, 3, 6, and 10 months. Activity was partially restricted until satisfactory cortical thickening or consolidation of the cyst was observed.
Clinical data were collected from the patients’ medical records. Age, gender, degree of fracture displacement, location of cyst, and cyst size were investigated, and we assessed how these factors affected cyst healing.
Age, gender, and degree of fracture displacement
The mean age at the time of the first visit was 10.8 years. Considering growth spurts, the patients were divided into three groups: before a growth spurt, during a growth spurt, and after a growth spurt (≤8, 11–14, and ≥15 years). 11 We evaluated 37 male patients and 19 female patients.
The degree of fracture displacement at fracture occurrence was also evaluated as a clinical factor that might affect cyst healing. The grade of fracture displacement was classified into three groups (non-displacement, ≤2 mm, and >2 mm). Non-displacement cases were defined as when only the fracture line was observed and there was no displacement visible AP and lateral simple radiographic images. Minimal displacement was defined as a fracture with a displacement of less than 2 mm on AP and lateral X-rays, and displacement was defined as a fracture with a displacement of greater than 2 mm on either the AP or lateral X-ray image, or both.
Location and size of cyst
We divided the cysts into metaphysis and diaphysis groups according to the location of the cyst and analyzed the radiological results.
The size of the cyst was defined as the ratio of the length of the cyst to the width of the adjacent physis based on picture archiving and communication system software (m-view 5.4; Marosis Technologies Inc., Seoul, Korea; Figure 1). 14 Because a cyst does not appear as an exact ellipse or quadrangle, the length of the cyst was based on the longest line that could be drawn in the cross section in the AP or lateral view.
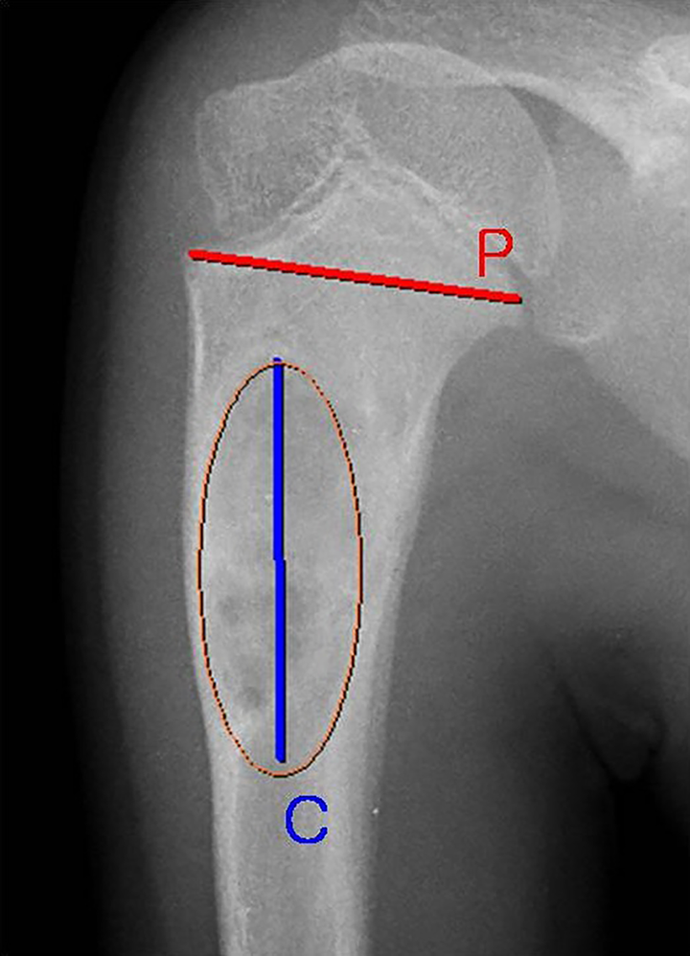
Cystic ratio. The size of a cyst was defined as the ratio (C/P) of the length of the cyst (C = blue line) to the width of the adjacent cyst (P = red line).
This method allowed for direct comparison of cyst size without the need for correction factors for differences in age between patients. This method also avoided errors resulting from radiological magnification. We did not calculate the width of the cyst because it was always equal to or slightly larger than the metaphyseal width.
The same two orthopedic surgeons reviewed all the X-rays of this study and measured the index on the AP and lateral radiographs; thus, the mean value was defined as the cystic ratio.
Clinical outcome evaluations
Patients who had bone consolidation and cyst healing without surgical treatment at the time of the last follow-up were considered to have a positive impact on healing. As a short-term result, patients who experienced recurrence more than 1 year after fracture and underwent surgical treatment but who showed cystic healing during the 1-year follow-up period were also considered to have a positive effect on cystic healing.
Statistical analysis
Statistical analysis was performed using SPSS ver. 18 (SPSS Inc., Chicago, Illinois, USA). Correlations between clinical results and parameters such as gender, location, size, and age were assessed with Fisher’s exact and χ 2 tests. Correlations between clinical results and age or degree of fracture displacement were investigated by one-way analysis of variance (ANOVA). A p value of less than 0.05 was considered statistically significant, and all aspects of the statistical analysis were reviewed by a statistician.
Results
We evaluated 56 consecutive patients, each of whom had a UBC in the proximal humerus. The mean follow-up duration was 58.2 months.
The overall healing rate of UBCs after fractures on pathologic bone was 66% (37 of 56 cases) (Figures 2 and 3). Of the 37 patients who obtained cyst healing, 11 underwent additional surgical treatment for recurrence or fracture of the cyst after 1-year of follow-up. As a short-term result, as previously noted, we considered those 11 patients as cases of healing after fracture.

Case presentation representing a 4-year-old girl with UBC of the left proximal humerus shaft. (a) Simple radiograph at first visit. (b) One month later, a fracture occurred on pathologic bone. (c) Observation of healing after 6 months of fracture. (d) Radiographs of the humerus at the time of final follow-up (3 years after fracture). UBC: unicameral bone cyst.

Case presentation representing an 8-year-old boy with UBC of the left humerus shaft. (a) Simple radiograph at first visit. (b) Two months later, a fracture occurred on pathologic bone. (c) Observation of healing after 6 months of fracture. (d) Radiographs of the humerus at the time of final follow-up (5 years after fracture). UBC: unicameral bone cyst.
The healing rate was significantly lower in 10–14-year-old patients (45%) who were in puberty than in those who were 9 years old or less (76%) or over 15 (80%). The healing rates of males and females were 68% and 63%, respectively, and there was no statistically significant difference between the two.
There was no statistically significant difference according to fracture displacement. The healing rate was 67% in those with non-displaced fractures, 70% in those with fractures with a displacement of less than 2 mm, and 58% in those with fractures with a displacement of 2 mm or more. There was a significant difference according to cyst site: the healing rate of cysts in the metaphysis (53%) was lower than that of those in the diaphysis (85%; Table 1).
Clinical and radiologic parameters affecting UBC healing after fractures on pathologic bone in the proximal humerus.

UBC: unicameral bone cyst; ANOVA: analysis of variance.
a The sum of cases that achieved consolidation and cyst healing without surgical treatment until the last follow-up visit and cases that recurred more than 1 year after the initial fracture and underwent surgical treatment; that is, those who showed cystic healing during the follow-up period of 1 year.
b Univariate analysis and one-way ANOVA. The p values are of intergroup comparisons. Significance was accepted for p values of <0.05.
The mean initial cystic ratio was 1.31 in the 37 patients who showed cyst healing within 1 year and 1.79 in the 19 patients who needed surgical treatment within 1 year, and this difference was statistically significant (Table 2).
Initial cystic ratio in the healed group and the non-healed group.

ANOVA: analysis of variance.
a Univariate analysis and one-way ANOVA. The p values are of intergroup comparisons. Significance was accepted for p value of <0.05.
Discussion
Numerous previous reports focused on certain clinical factors that are associated with an increased incidence of fractures on pathologic bone with UBC (such as radiographic features, 15 percentage of bone occupied by the cyst, 16 and cortical thickness 17 ) and treatment plans for pathologic fractures and cystic lesions. 18,19 This is the first study that focused on factors related to healing after fractures on pathologic bone of UBCs in the proximal humerus.
We concentrated on the role of fractures on pathologic bone in cyst healing. So, we evaluated proximal humerus lesions because conservative treatment is generally the initial approach to UBCs in the upper extremities, whereas treatment of fractures on pathologic bone in the proximal femur is usually done surgically. 3,20
For UBCs, the ratio of males to females is about 2:1. 21 However, the male-to-female sex ratio in fractures on UBCs is not known. This study suggests that the incidence of fractures on pathologic bone is similar to the incidence of UBCs (1.95:1).
The natural history of UBCs is variable, but the cysts tend to improve gradually with time and growth. 22 Many UBCs persist into adulthood, whereas some spontaneously resolve during puberty. 11 Despite having a small number of patients, this study showed poor cyst healing after fractures on pathologic bone in the pubescent group. These results suggest that the healing process of cysts after a fracture is negatively correlated with normal growth promotion. Of course, in order to support this hypothesis, a long-term study is needed that follows patients into adulthood and includes many patients of various ages.
Another limitation of our study involved the degree of fracture displacement. In cases of severely displaced fractures, immediate surgery was done and those cases were excluded from our analysis, so we cannot conclude that the degree of displacement of a fracture is independent of cyst healing. Also, because most fractures on pathologic bone of UBCs are microfractures or minimally displaced fractures, 23 the number and amount of information on such cases is insufficient to distinguish between the degree of fine fracture displacement in millimeters.
A previous report showed that active-phase UBCs in an upper limb are associated with a greater risk of fracture. 22 The high occurrence of fractures in ballooning bones and reduced cortical thickness may reflect the vulnerability of ballooning bones and the mechanical weakness of long bones, and multilocular UBCs were usually observed in widely spaced cysts. In UBCs in the humerus, a latent phase significantly promoted healing of the UBC, and this finding is consistent with previous reports. 24 Several previous studies reported that active cysts cause fractures more often and active cysts are also unlikely to regress. 16 In contrast, latent cysts are more likely to resolve, with or without treatment. Taken one step further, our study suggests that cystic activity inhibits the healing process by decompression after fracture as well as by inducing fractures. Of the 14 patients who experienced cyst healing without recurrence or additional surgery, only 5 had active cysts. Also, among the patients who underwent surgical treatment, eight of nine had active cysts and showed treatment failure at the final follow-up.
Several studies have reported that the larger the size of a cyst, the higher the probability of a fracture on pathologic bone. 15,16 There have only been a few studies on the effect of size on cyst healing after fracture, and the aim of those studies was to evaluate clinical outcomes after steroid injection or open surgery. 14,25 The results of those studies are similar to our results in that large cysts were less likely to heal after a fracture. However, our study is useful as it looked at the outcome of purely conservative treatment without injection or surgery after fracture.
Recent studies have engendered some debate regarding fractures on pathologic bone of proximal femurs with UBCs. De Sanctis and Andreacchio 12 found no difference in healing time between UBCs with fractures on pathologic bone in the proximal femur and those without such fractures. A longer healing time was needed in patients without a fracture, though that result was not statistically significant. Cha et al. 13 reported that whether or not a fracture had occurred before surgical treatment, intramedullary nailing of femoral UBCs resulted in reliable healing, and the frequency of recurrence did not differ. Those results contradict the existing idea that fractures induce healing of cystic lesions. It is possible that these results are related to weight-bearing in the bone and surgical treatment that should have already been done. As previously mentioned, a study of fractures on pathologic bone in the upper extremities should be free from such biases.
This study found a positive effect, 66%, of fractures on cyst healing. Of course, the relatively small or equal number of individuals compared to previous studies for fractures on pathologic bone of the proximal humerus 25 (68 patients) is one of the limitations of this study.
Conclusion
In conclusion, UBCs of the humerus after fractures on pathologic bone have better clinical results in latent lesions and in older patients who have gone through puberty than in active lesions and in pre-pubescent patients. Fractures on pathologic bone in proximal humerus UBCs often dramatically decrease the size of the cyst, and such patients have excellent clinical results in terms of healing rate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.