
Abstract
Purpose:
Injury to the distal triceps brachii tendon is rare. Imaging radiographs are used to confirm the findings of physical examination, classify the extent of injury, and guide treatment. Magnetic resonance imaging (MRI) is considered the gold standard of diagnostic imaging. However, no previous study has reported on the accuracy of differentiation between partial- and full-thickness triceps tendon tears. Our study’s aim was to define the accuracy of MRI in differentiating partial- from full-thickness tear of the distal triceps tendon. We hypothesized that MRI has low accuracy in differentiating partial- from full-thickness tears.
Methods:
A total of eight patients with nine triceps tendon tears underwent surgical repair from 2011 to 2015. MRI of the elbows were retrospectively reviewed for the presence and type of tear, tendon involvement, and location of the tear, and later correlated with surgical findings.
Results:
Of the three surgically confirmed complete tears, MRI correctly reported a complete tear in all patients. Of the six partial tears confirmed at surgery, MRI correctly identified four tears. In two cases, MRI described a complete tear, but only a partial tear was noted at surgery.
Conclusion:
False-positive MRI assessment of distal triceps injury is not rare. Surgeons should rely on clinical examination in assessing distal triceps tendon injury, with imaging studies providing an adjunctive role in the diagnosis and decision-making.
Keywords
Introduction
Triceps tendon rupture is rare, accounting for less than 1% of all tendon ruptures, with male predominance. 1 The use of anabolic steroid has been associated with this injury. The current trend in sports participation, especially in weight lifting and professional football players, also contributes a higher risk for rupture. 2 Other risk factors include local steroid injection and olecranon bursitis. 3 –6 Metabolic bone disease such as hyperparathyroidism and adolescent age with incompletely fused physes are also risk factors for triceps tendon rupture. 7
Triceps tendon ruptures occur as an indirect insult resulting from forceful eccentric contraction of the muscle such as falling on the outstretched hand or during weight lifting. Insertional injury is more common rather than musculotendinous injury. A report indicated that more than half of all acute triceps injuries were misdiagnosed. 8 An apparent loss of elbow extension strength is the hallmark subjective complaint. Swelling and bruising are usually present in the acute setting. On physical examination, localized tenderness over the proximal site of the olecranon is almost always present. A palpable “step-off” defect will confirm the diagnosis. Terminal flexion pain may be present with full range of motion. However, if the elbow is positioned against gravity, its inability to extend will confirm the diagnosis. This is due to the failure of lateral expansion of the muscle as the dominant anatomical structure to preserve elbow extension in antigravity position. Hence, accurate and systematic physical examination is never to be underestimated.
Plain radiographs should be presented in every case. The presence of small flakes superior to the olecranon is a telltale sign of avulsion fracture. Soft tissue shadow representing edema, which indicates olecranon bursitis, frequently accompanies triceps tendon injury. Advance imaging techniques such as ultrasonography (US) and magnetic resonance imaging (MRI) are usually necessary to confirm muscle integrity, and the latter is commonly accepted as the best modality to determine soft tissue injury. Studies have shown that MRI can distinguish between normal and torn tendons. 9,10 However, the visualization of partial tears may hinder the final conclusion. Accurate diagnosis plays an important role in the management of triceps injury. Sagittal MRI remains the gold standard of triceps tendon injury diagnosis. To the best of our knowledge, only one study reported on the discrepancy between surgical and magnetic resonance (MR) findings. 11 Nevertheless, no previous study has reported on the accuracy of differentiation between partial- and full-thickness triceps tendon tears. This concern is raised because of the possible conservative treatment of partial tears. The aim of this study was to define the accuracy of MRI in differentiating partial- from full-thickness tears of the distal triceps tendon. We hypothesized that MRI has low accuracy in differentiating partial- from full-thickness tears.
Materials and methods
The study was performed in accordance with the World Medical Association Declaration of Helsinki and Health Insurance Portability and Accountability Act (HIPAA). An electronic retrospective review was performed for patients who underwent elbow MRI between 2011 and 2015. A total of 13 patients with 15 distal triceps tendon tears were found. Patients who received conservative treatment and did not have preoperative MRI were excluded from the study. A total of eight patients with nine triceps tendon tears underwent surgical repair. Two musculoskeletal radiologists retrospectively reviewed the MRI. Descriptions regarding the presence and type of tear, tendon involvement, and location of the tear were documented by the radiologist and then correlated with our surgical findings.
All MR examinations were performed on a 3.0-T system (Ingenia; Philips Medical Systems, Best, the Netherlands). The acquired sequences were coronal and axial fat-saturated T2-weighted image, sagittal T2-weighted image, coronal T1-weighted image, coronal intermediate-weighted image, and coronal and sagittal fat-saturated T2-weighted image after injection of gadolinium contrast agent.
A complete tear was defined as a full-width, full-thickness tear. A partial tear was defined as a partial-width tear, partial-thickness tear, or both. A tear reported by the radiologists to involve more than 90% or nearly full-thickness was considered a complete tear. Partial tears usually occur distal to the olecranon insertion and become visible as a small fluid-filled gap inside the ruptured distal triceps tendon. A complete tear is characterized by a large fluid-filled gap in the T2-weighted image between the retracted stump of the triceps tendon and the olecranon process. Acute tears are clearly delineated by the surrounding fluid. Tendinosis could be appreciated if there is tendon thickening with or without edema (Figure 1). Partial tears will appear as a hyperintense area in both T1- and T2-weighted images with an intact hypointense portion (Figure 2).

T2-weighted sagittal MRI showed full-thickness rupture of the distal triceps tendon with soft tissue edema. MRI: magnetic resonance imaging.
T2-weighted sagittal MRI showed partial-thickness tear. The deep layer of the distal triceps tendon remains in continuity. MRI: magnetic resonance imaging.
Patient demographic data, injury mechanism, and type of surgical intervention were documented.
Results
Nine distal triceps tendon tears were identified in eight patients (female, n = 2, 22%; male, n = 6, 78%). The mean age was 45 years (range, 32–58 years). The most common cause of injury was direct posterior elbow force after a fall. One male patient who sustained a bilateral distal triceps tear after simple fall injury had a history of chronic renal failure.
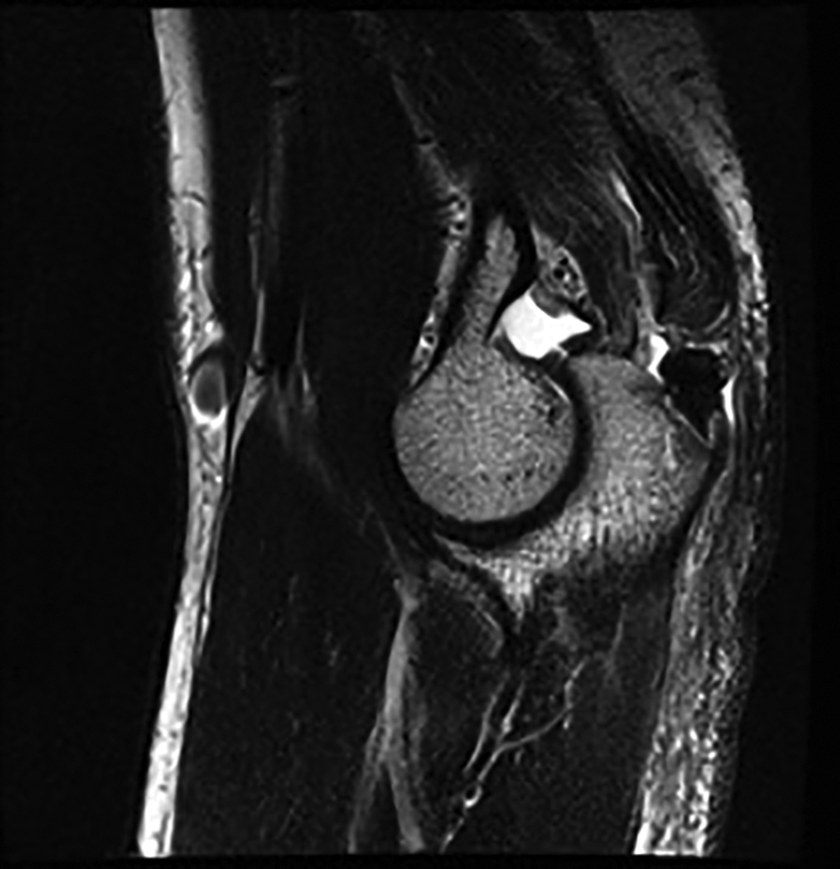
All cases of torn tendon as reported by the radiologist have been confirmed surgically. MRI was accurate in detecting all tears. There was no reporting discrepancy between two radiologists. Of the three surgically confirmed complete tears, MRI correctly reported a complete tear preoperatively in all patients. Of the six partial tears confirmed at surgery, MRI correctly identified four tears (Table 1). In two cases, MRI described a complete tear (Figure 3), but only a partial tear was noted at surgery (Figure 4). Primary repair was done in all cases with heavy-suture transosseous equivalent technique or suture anchor. One patient needed V-Y lengthening for retracted tear.
The presentation of MRI findings in association with surgical findings.

MRI: magnetic resonance imaging.

T2-weighted sagittal MRI showed full-thickness tear of the distal triceps tendon. MRI: magnetic resonance imaging.
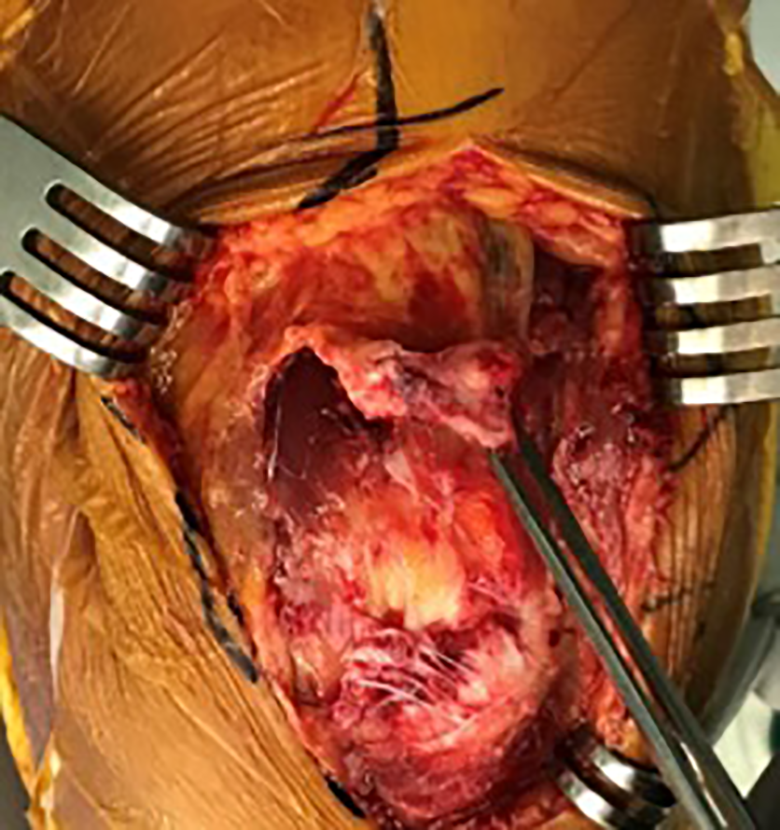
Intraoperative findings revealed that only the superficial layer of the distal triceps tendon was torn and the deep layer was intact; however, MRI reported a full-thickness tear. MRI: magnetic resonance imaging.
Discussion
The triceps brachii muscle has three heads: medial, lateral, and long heads. The footprint insertion covers a wide area (466 mm2) starting 12 mm distal to the tip of the olecranon and blending with the posterior capsule. The mediolateral and proximo-distal footprint widths were 20.9 and 13.4 mm, respectively. 12 –14 A study has shown that the distal part of the medial aspect is confluent with the remaining triceps tendon rather than a distinct separation, often showing a thickened cord appearance. The lateral aspect is more convoluted and expansive and maintains a continuity to the anconeus fascia down to their common fascial insertion on the lateral aspect of the forearm. The lateral aspect of the distal triceps comprises approximately 70% of the width of the central triceps tendon. 14 The length of the triceps is critical to its extension strength. A shortening as little as 2 cm may cause a 40% decrease in extension strength. 15
The management of distal triceps tears is generally dictated by muscle integrity and functional assessment of extension strength. In general, any tear extending more than 50% of the tendon’s integrity and full-thickness tear are managed surgically, which, according to a study, remains superior for such tears. 12 In our study, MRI has proven to be sensitive in diagnosing tendon tear, but it was inferior in differentiating full- and partial-thickness tear. False-positive interpretation of partial-thickness tendon tear is not rare as reported by previous studies. 11,16 –18 Similar circumstances have been shown in the diagnosis of a delaminated rotator cuff tear using MR. The sensitivity, specificity, and positive predictive value of MRI in identifying partial-thickness tear were reported as 51.6%, 77.2%, and 41.3%, respectively, 19 which shows the limitation of MRI in diagnosing partial-thickness tendon tear. Several factors might be contributing to this imaging–anatomical pathology discrepancy. First, the large area of the distal triceps tendon necessitates the expansion of the axis plane of the main magnetic field. The three-dimensional extension of the partial-thickness tear of the distal triceps (thickness, proximo-distal retraction, mediolateral extension) should be noted carefully while analyzing and evaluating the MR images. 16 Orthopedic surgeons should always evaluate MRI on their own, taking into consideration the background of the clinical examination, history, and current complaints of the patients. Second, both surgeon and radiologist need to be careful in their assessment and avoid false-positive diagnosis of tendinous disease by bearing in mind the so-called magic angle effect phenomenon, which has a substantial angle-dependent effect on tendon orientation that can increase signal intensity in vivo. 20 Third, anatomically, the distal triceps is tubular in the central area and becomes sheet-like as it expands mediolaterally. This tubular solid form is subjected to higher shear loading due to its volume–area proportion, resulting in a tear, despite the mediolateral expansion hood sharing the load as a result of its larger volume area. This posits a likelihood that a complete tear will almost never be discovered in an indirect injury mechanism.
Although the value of elbow MRI is well-known, US examination is advantageous in terms of time, cost-effectiveness, and accessibility. Direct patient interaction allows direct correlation with the site of pain through comparison with the contralateral elbow. Dynamic US allows the use of stress maneuvers and visualization of transient conditions that may not otherwise be revealed during static examination. 14 Furthermore, because of the superficial location of the triceps muscle combined with the real-time dynamic properties of US examination, it is considered as an important tool in diagnosing triceps tendon tear and in differentiating partial from complete tear aside from detecting various elbow abnormalities and could be an alternative to MRI. However, US remains an operator-dependent modality and only provides minimal information regarding muscle quality. MRI is proven to be useful in assessing muscle quality, especially for delayed chronic cases, and can determine if a more extensive reconstruction of the defect is required. 8
A partial-thickness tear less than 50% can still be treated conservatively. Hence, with the management of distal triceps tendon ruptures being dependent on the extent of the tear, accurate diagnosis is important.
Our study has its limitations. First, the small sample number was due to the low incidence of distal triceps tendon rupture in our center. Second, it was retrospectively designed. Nevertheless, we would like to share our valuable findings that MRI may not be as accurate in differentiating partial- from full-thickness distal triceps tendon tear.
Conclusion
False-positive MRI assessment of distal triceps injury is not rare. Therefore, surgeons should rely on clinical examination in assessing distal triceps tendon injury, with imaging studies providing an adjunctive role in the diagnosis and decision-making. A further evaluation of pre-injury functional level and patient expectation is essential.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed the receipt of following financial support for the research, authorship, and/or publication of this article: This study was supported and funded by the National Research Foundation of Korea via the Korean Government (MSIP) [grant no. 2017-0522].