
Abstract
Patellar instability is a common debilitating injury affecting young active individuals. It accounts for approximately 3% of all knee injuries. We report a family, of which five members across three generations, who suffered from autosomal dominant familial recurrent patellar dislocation as well as short stature. All of them have recurrent patellar dislocations before the age of 15. The affected patients in all three generations have been genetically screened. Genotypical evaluation revealed a balanced translocation of chromosomes 15 and 20.
Introduction
Patellar instability is estimated to affect 1 in 1000 individuals. 1 Patients with the second episode of injury have a 50% risk of further recurrent dislocation. Miller reported a family with recurrent patellar dislocations inherited in an autosomal dominant pattern in 1978. 2 Borochowitz et al. also described a family in which multiple members had recurrent dislocation of the patella, with several instances of male-to-male transmission. 3
Similarly, Rebolledo reported three patients in one family (mother and two children) with trochlear dysplasia and recurrent bilateral patellar dislocations in 2012 following a French report on familiar trochlear dysplasia by Rouvillain. 4,5 These case reports of familial disease pattern suggest a genetic component, although the underlying genetic basis is yet to be identified.
We report a family, of which five members across three generations suffered from autosomal dominant familial recurrent patellar dislocation and short stature. The cases were genetically confirmed to have balanced translocation of chromosomes 15 and 20.
Case series
Generation 1
Ms F, a 58-year-old lady, presented in her twenties due to recurrent patellar dislocation. She underwent bilateral arthroscopic lateral release in a tertiary hospital in the 1980s. Intraoperative finding revealed bilateral trochlear dysplasia with tight lateral retinacula and moderate osteoarthritic change over bilateral patellofemoral joints (PFJs).
Post-operatively she was well with no further dislocations. However, in the last 5 years, she has been suffering from bilateral PFJ osteoarthritis. She complained of anterior knee pain when walking on stairs. Clinical examination shows short stature with a height of 136 cm (12 cm below 3rd centile) and weight of 46.7 kg (25th centile). General examination revealed no nail or iliac abnormalities to suggest nail-patella syndrome. There was no coronal or rotational malalignment. Bilateral knees examination revealed bilateral PFJ crepitus and a positive grind test. X-ray of the knees showed severe PFJ arthritic changes with relatively preserved medial and lateral compartment (Figure 1). PFJ replacement is planned for Ms F.
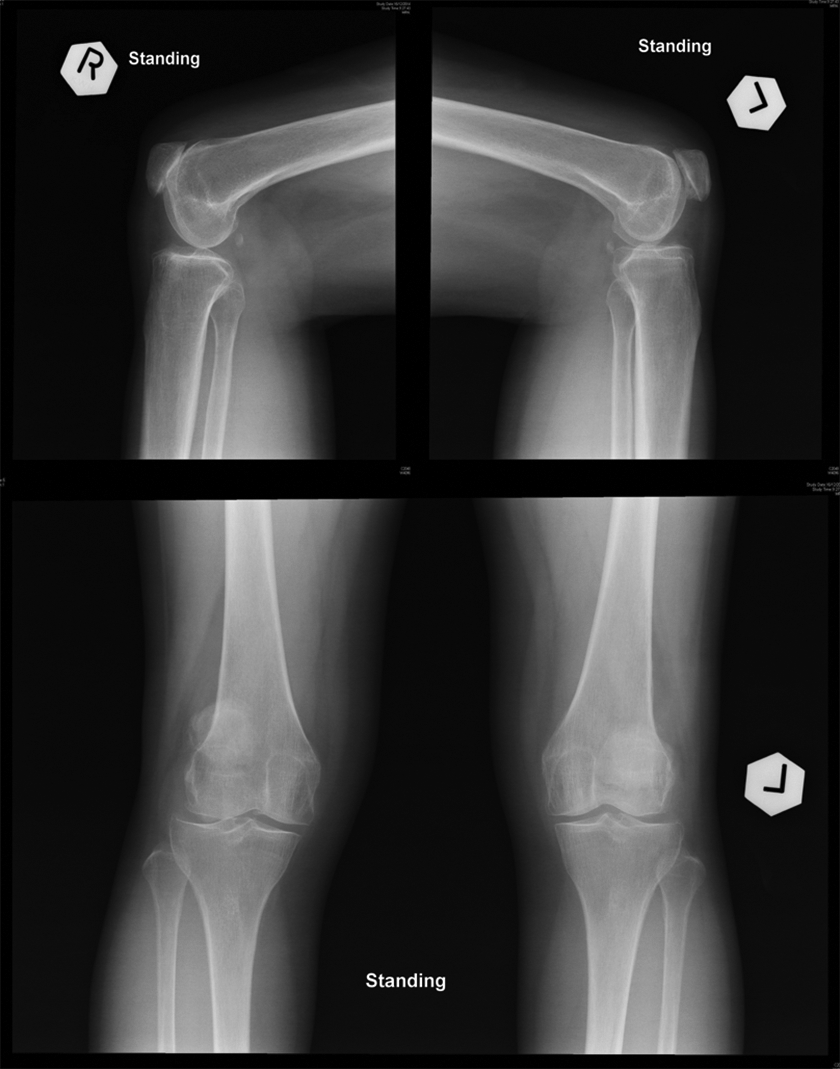
X-ray of the bilateral knees of Ms F.
Generation 2
Case 1: Ms K, a 33-year-old housewife, who otherwise enjoyed good past health. She is the daughter of Ms F and also the mother of the three patients in the third generation.
She complained of bilateral recurrent patellar dislocations since the age of 10, more severe over the left side. When she first presented at the age of 16, bilateral knees were in valgus. Both patellae were everted to the lateral sides. The left patella could be dislocated upon extension every time. Crepitus could be felt over the PFJ upon grinding.
Computer tomography (CT) of her knees showed bilateral shallow trochlear grooves with marked lateral dislocation of the patellae (Figure 2). She underwent medial patellofemoral ligament (MPFL) reconstruction and anteromedial tibial tuberosity transfer of the left knee in 2011. Intraoperatively, it was found that the patella was dislocated laterally upon full extension and reduced every time when it was passively flexed beyond 45°. Arthroscopy showed a hypoplastic lateral femoral condyle with cartilage degeneration over the medial facet and a crabmeat appearance. After the first surgery, there were no further dislocation or subluxation of the left knee.

CT of bilateral knees of Ms K.
MPFL reconstruction and anteromedial tibial tuberosity transfer of the right knee was also performed in 2013. Intraoperative findings again showed a hypoplastic lateral femoral condyle and a loose body within the knee joint, probably an old osteochondral fragment loosely attached at the lateral gutter. The patellar cartilage was eburnated with the loss of normal bifacetal configuration. Post-operatively she recovered well and reported no further instability symptoms. Currently, her height is 140 cm (8 cm below 3rd centile), her weight is 54.1 kg (75th centile).
Case 2: Mr J, 31 years old, is the son of Ms F. He presented with bilateral recurrent patellar dislocations since the age of 12. He underwent bilateral reconstructive surgeries including bilateral lateral release, tibial tuberosity medialization, medial plication and microfracture in 2003. Intraoperative findings showed bilateral eburnated patellae, shallow femoral trochleae and osteophytes over bilateral lateral femoral condyles. Post-operatively he recovered well. There were neither dislocations nor instability symptoms afterwards. The left patella is seen partially on the lateral aspect of the femoral trochlea. X-ray skyline view showed laterally subluxed left patella. However, the patient is asymptomatic. The latest height is 153 cm (5 cm below 3rd centile) and the weight is 71 kg (75–90th centile).
Generation 3
Case 1: Ms Y is the elder daughter of Ms K, currently 15 years old. She had two episodes of right knee sprain with patellar dislocation and spontaneous reduction when she first presented at the age of 11. Magnetic resonance imaging (MRI) of the right knee showed that the trochlea was shallow with a lax MPFL (Figure 3). She is having recurrent dislocations of the right patella, around three episodes per month, usually when walking on stairs, with minimal trauma. Clinically, she is 131 cm (14 cm below 3rd centile) tall and her weight is 41.5 kg (10–25th). Examination of the knee revealed positive J sign and lateral displacement test over both knees. There is generalized ligamentous laxity, with a Beighton score of 5/9. Further preoperative imagings were arranged in preparation for her patella stabilization surgery.

MRI of the right knee of Ms Y.
Case 2: Ms L, the younger daughter, is currently 13 years old. She has recurrent patellar dislocations of the left knee, about once a month. Clinically, she has generalized ligamentous laxity, bilateral valgus knees, positive J sign and displacement test. Her current height is 128 cm (14 cm below 3rd centile) and her weight is 35.8 kg (10–25th).
Case 3: Ms W, as the youngest daughter, is currently 7 years old. She has no history of patellar dislocation so far but clinically she has short stature and genu valgum. She is now followed up by the paediatrician (Figures 4 and 5).

Pedigree of the family.

Clinical photo of the family members showing all of them having short stature.
Genetic evaluation
Genetic studies were performed on all of the above subjects and karyotyping showed 46, XX, t(15;20) (q24;q13.1). This is an apparently balanced translocation between chromosome 15 and 20, with breakage and reunion at band 15q24 and 20q13.1. The segments distal to these bands have been exchanged. Chromosomal array showed no clinical significant copy number change at the breakpoint. Family studies showed the chromosomal translocation is inherited from the maternal side of the family and is completely segregated among those affected individual (Figure 4).
Discussion
Patellar instability is a common injury typically affecting young active individuals. It can result in significant limitations of activity and long-term arthritis especially over the PFJ. Instability of the PFJ is multifactorial in cause. Abnormalities including the bony structure of the patella and trochlea, the alignment of the lower limb, the integrity of the surrounding soft tissues, systemic conditions affecting connective tissues and overall muscle tone might lead to instability. Familial patellar dislocation is uncommon but has been reported in the literature. 2 –5 Previous case series have suggested a genetic cause of but the exact genetic and molecular basis has not been well studied.
In this family, all the family members with recurrent patellar dislocation, except the younger sister in the third generation, showed trochlear dysplasia either intraoperatively or radiologically. The younger sister is still skeletal immature and further imaging including MRI is arranged to look for evidence of trochlear dysplasia. Their first dislocations were all before the age of 15. We also notice that all of them have short stature with heights way below the 3rd percentile of their corresponding ages. Genetic studies revealed that they all have a balanced translocation between chromosomes 15 and 20. A detailed literature search failed to identify any identifiable diseases related to the genetic abnormalities of the chromosomes 15 or 20. This case series reports a novel association of familial patella dislocation and balanced translocation of chromosomes 15/20. This translocation seems to segregate with the condition of familial patellar dislocation with features of trochlear dysplasia and may also be responsible for the short stature that runs in the family. The mode of inheritance appears to be autosomal dominant, which echoes with Miller’s case showing an autosomal dominant pattern of familial patellar dislocation. 2 That means there should be a potential ‘new’ locus for autosomal dominant patellar dislocation and short stature syndrome. Further follow-up of the whole family and further genetic workup are warranted so as to delineate the exact causal relationship between this chromosomal abnormality and the conditions of familial patellar dislocation together with short stature.
The current concept of treatment of a first-time dislocation is still debatable. Most centres suggest a conservative treatment with a short period of immobilization followed by quadriceps muscle strengthening and range of motion exercise. Exception scenarios include the presence of osteochondral fracture or joint incongruity. For patients with recurrent dislocations, surgery is usually recommended for correcting pathological structures. If the risk of recurrence is high, it is recommended to correct significantly abnormal anatomic features that can contribute to the increased risk.
Since all the affected members in this family have their first dislocation at a young age, subsequent recurrent dislocations, and all demonstrate trochlear dysplasia, their risk of recurrence is very high. They may therefore benefit from an earlier operative treatment even after their first episode of dislocation, so as to prevent recurrent dislocation and complications of dislocation including fracture and PFJ arthritic change.
There are quite a few genetic disorders that are well known to present with patellar instability. The most famous one is nail-patella syndrome, which is an autosomal dominant genetic disorder with mutation of gene LMX1B. Patients usually present in late childhood with patellar instability due to hypoplastic patella and lateral femoral condyle. They also present with dystrophic nails or hypoplastic radial neck causing radial head subluxation. Up to 80% of patients have iliac horns in their pelvic X-rays, which is a feature considered to be pathognomonic of nail-patella syndrome. Other disorders which may present with recurrent patella dislocation include Larsen syndrome, Amyoplasia congenita and syndromes of generalized ligamentous laxity including Ehlers Danlos syndrome and Marfan syndrome. Larsen syndrome is a rare disorder affecting the development of bones and connective tissues throughout the body. It is caused by a genetic defect in the gene encoding filamin B, which is a protein that is important in regulating the structure and activity of the cytoskeleton. 6 Patients can present with dislocation of hips, knees and shoulders together with flattened facial appearance and a variety of cardiovascular abnormalities. 7 Amyoplasia congenital, the classical form of arthrogryposis multiplex congentia, is characterized by four limbs contractures and deformities and by the replacement of skeletal muscle by dense fibrous and adipose tissue. 8 The occurrence is sporadic, with no specific gene that is known to cause such disorder, and individuals with amyoplasia have unaffected children. 9 In contrary to these well-known disorders, all the family members in this case neither have syndromal features nor other skeletal abnormities, except for the presence of short stature.
This case report illustrates a unique family whereby three serial generations have been affected with recurrent patellar dislocation. It is also the first case in the literature where an identified genetic component, namely a balanced translocation of chromosomes 15 and 20, is suggested to be responsible for such a familial patellar dislocation. It should be noted that karyotyping is warranted if more than one family member have recurrent dislocations. Counselling and screening of family members are essential, and offering earlier operative treatment may decrease morbidity and improve the outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.