
Abstract
Spondylolysis is a major cause of back pain in children and adolescents. The prevalence of spondylolysis depends on the sex, race, and congenital abnormality. These biases suggest hereditary predisposition as an etiology of spondylolysis. However, no conclusive evidence still exists regarding the inheritance for spondylolysis. Herein, we report rare cases with familial occurrence of lumbar spondylolysis. In two generations of a Japanese family, three brothers including identical twins complained of back pain related to sports activities. Clinical, radiographic, and computed tomographic examinations identified spondylolysis at L4 and L5 in all these boys. The father experienced long-term back pain and had spondylolisthesis at L4–L5 and healed spondylolysis at L5. The daughter and mother did not show any lumbar spondylolysis. The frequent development of spondylolysis at L4, a rarely affected segment, in four of six family members (66.7%) support that lumbar spondylolysis has an underlying genetic etiology, primarily autosomal dominant inheritance.
Keywords
Introduction
Spondylolysis is a unilateral or bilateral defect in the pars interarticularis of the vertebral arch that connects the upper and lower facet joints. This disease is observed in 3–6% of the population. 1 –4 In most spondylolysis cases, the lowest level of lumbar vertebrae, L5, is affected. 2 –5 Reportedly in Japan, the prevalence of spondylolysis at L5 is 90.3%, while it is only 5.6% at L4. 4 Spondylolysis can progress into spondylolisthesis if the vertebral body slips forward. 2,3 These structural defects and instability often induce pain and limit physical activities. 6,7 Neurological symptoms are present in rare cases. Spondylolysis and spondylolisthesis are major causes of back pain in children and adolescents, particularly in athletes. 8 The principal etiology of spondylolysis is considered as a stress fracture of the vertebral bone. 9
The prevalence of spondylolysis is higher in men than in women. 1 –4 In Japan, 7.9% of men versus 3.9% of women have spondylolysis. 4 The occurrence of spondylolysis also depends on the race as well as sex, a reported incidence of which is 6.4% in white men versus 2.8% in black men and 2.3% in white women versus 1.1% in black women. 1 It is noteworthy that particular racial groups, such as Inuits, have a quite high prevalence of spondylolysis—approximately 40%. 10 –12 Further, a markedly frequent coexistence of spondylolysis and spina bifida occulta is known. 2,4,13,14 These biases in sex, race, and congenital abnormality strongly suggest hereditary predisposition as an etiology of spondylolysis. However, no conclusive evidence still exists regarding the inheritance for spondylolysis.
The objective of this study was to report rare cases of spondylolysis at L4 from two generations of a family. All family members underwent clinical and radiological examinations, including radiography and computed tomography (CT), which revealed that four of six persons (66.7%) had spondylolysis at L4, a rarely affected segment. These familial cases support the notion that lumbar spondylolysis has an underlying genetic etiology, primarily an autosomal dominant pattern of inheritance.
Case reports
This study was approved by the institutional review board at the authors’ institution. Written informed consent was obtained from each subject. Further, these subjects and/or their families were informed that data from the cases would be submitted for publication and gave their consent. This study was conducted in concordance with the principles of the Declaration of Helsinki and with the laws and regulations of Japan.
Case 1
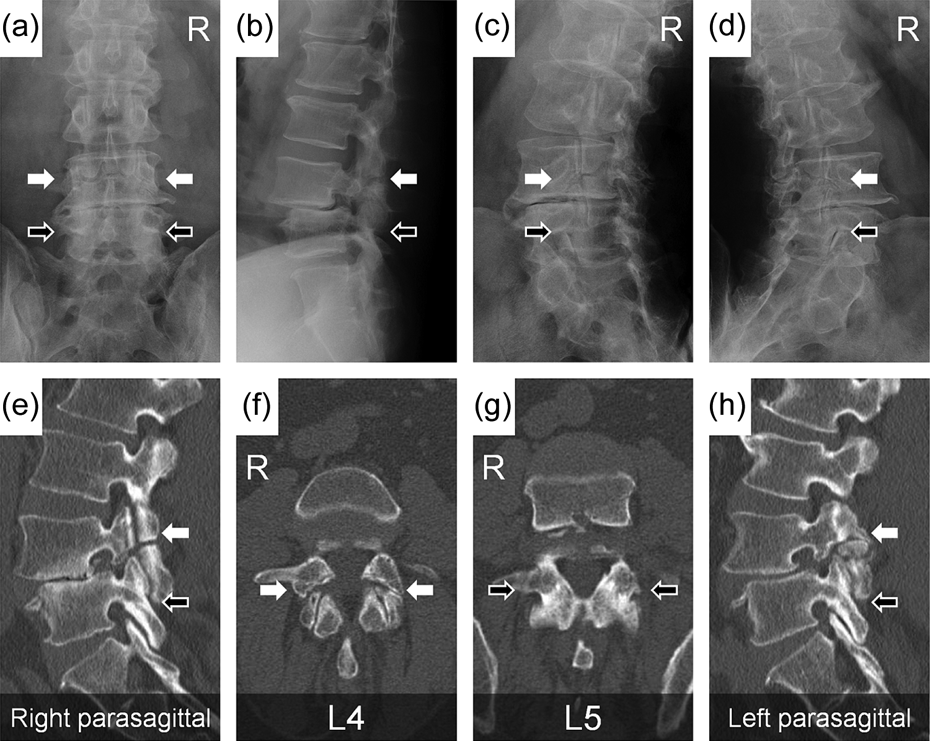
The 17-year-old first-born son visited our clinic and complained of low back pain that arose while playing football. Radiographs showed bilateral spondylolysis at L4 and L5 (Figure 1(a) to (d)). Then, CT multi-planar reconstruction images demonstrated signs of the terminal pseudoarthrosis stage 15 of spondylolysis (Figure 1(e) to (h)). His symptoms were relieved after 1 month of wearing a soft brace. He continued to play football but often felt recurrent back pain.

Lumbar spine radiographs and CT images of the 17-year-old first-born son. Spondylolysis (white arrows) was observed at L4 and L5 in posteroanterior (a), lateral (b), 45-degree right anterior oblique (c), and 45-degree left anterior oblique (d) radiographs and right parasagittal (e), axial parallel to the L4 vertebral arch (f), axial parallel to the L5 vertebral arch (g), and left parasagittal (h) CT images. R indicates the right side of the body. CT: computed tomography.
Case 2
The 14-year-old third-born son and identical twin was a table tennis player. He visited our clinic and complained of frequent low back pain. Radiographs and CT images displayed bilateral complete 15 spondylolysis at L4 and L5 (Figure 2(a) to (h)). He stopped sports activities and underwent three-month wearing of a hard brace but did not obtain bone union of any spondylolytic lesions. Thereafter, he returned to play table tennis with mild back pain.

Lumbar spine radiographs and CT images of the 14-year-old third-born son. Spondylolysis (white arrows) was observed at L4 and L5 in posteroanterior (a), lateral (b), 45-degree right anterior oblique (c), and 45-degree left anterior oblique (d) radiographs and right parasagittal (e), axial parallel to the L4 vertebral arch (f), axial parallel to the L5 vertebral arch (g), and left parasagittal (h) CT images. R indicates the right side of the body. CT: computed tomography.
Case 3
The 14-year-old fourth-born son and identical twin visited our emergency room because of experiencing severe low back pain while playing football. Radiographs and CT images exhibited early to moderate stages 15 of bilateral spondylolysis at L4 and L5 (Figure 3(a) to (h)). After 3 months of rest from sports participation and wearing a hard brace, he obtained bone union at L5, but not L4. He went back to football with lesser back pain.

Lumbar spine radiographs and CT images of the 14-year-old fourth-born son. Spondylolysis (white arrows) was observed at L4 and L5 in posteroanterior (a), lateral (b), 45-degree right anterior oblique (c), and 45-degree left anterior oblique (d) radiographs and right parasagittal (e), axial parallel to the L4 vertebral arch (f), axial parallel to the L5 vertebral arch (g), and left parasagittal (h) CT images. R indicates the right side of the body. CT: computed tomography.
Case 4
The 50-year-old father was the owner of a grocery store and did not practice any sports but complained of long-term low back pain. He visited our clinic and underwent radiographic and CT examinations, which identified established spondylolisthesis at L4–L5 (Figure 4(a) to (h)). His L5 vertebra presented signs of spontaneous healing after spondylolysis. His symptoms were reduced with anti-inflammatory drugs.
Lumbar spine radiographs and CT images of the 50-year-old father. Spondylolisthesis (white arrows) was observed at L4–L5 in posteroanterior (a), lateral (b), 45-degree right anterior oblique (c), and 45-degree left anterior oblique (d) radiographs and right parasagittal (e), axial parallel to the L4 vertebral arch (f), axial parallel to the L5 vertebral arch (g), and left parasagittal (h) CT images. The L5 vertebra presented signs of spontaneous healing after spondylolysis (black arrows). R indicates the right side of the body. CT: computed tomography.
Non-spondylolysis cases
The 16-year-old second-born daughter was asymptomatic. However, she felt worried about spondylolysis and visited our clinic. She underwent clinical and radiological examinations, but all were negative for lumbar spondylolysis (Figure 5(a) to (h)). The 48-year-old mother also underwent similar examinations, which demonstrated degenerative changes but no spondylolysis in the lumbar spine (Figure 6(a) to (h)).

Lumbar spine radiographs and CT images of the 16-year-old second-born daughter. Spondylolysis was not observed in posteroanterior (a), lateral (b), 45-degree right anterior oblique (c), and 45-degree left anterior oblique (d) radiographs and right parasagittal (e), axial at L4 (f), axial at L5 (g), and left parasagittal (h) CT images. R indicates the right side of the body. CT: computed tomography.

Lumbar spine radiographs and CT images of the 48-year-old mother. Spondylolysis was not observed in posteroanterior (a), lateral (b), 45-degree right anterior oblique (c), and 45-degree left anterior oblique (d) radiographs and right parasagittal (e), axial at L4 (f), axial at L5 (g), and left parasagittal (h) CT images. R indicates the right side of the body. CT: computed tomography.
Discussion
Familial occurrence of spondylolysis has been discussed for many years. A prior study from Edinburgh reported that 14.9% of first-degree relatives of patients with spondylolisthesis at L5 had spondylolysis or spondylolisthesis. 16 A similar study also found that the incidence in first-degree relatives of the patients in a Wilmington institute was 22%. 17 Further, another study investigating families of 23 spondylolysis patients in a community of the US East Coast demonstrated that 31.8% of fathers, 17.4% of mothers, and 34.0% of male siblings had spondylolysis. 2 These incidences are higher than that in the general population. 1 –4 However, compared with Western countries, 2,16 –18 evidence of familial spondylolysis in Asia is scarce. 19 –22 More importantly, despite much debate about a genetic etiology of spondylolysis, its specific modes of inheritance are not fully understood. This case report presents characteristic CT images as well as radiographs of all affected and unaffected members of a two-generation Japanese family including identical twins. This yielded a notably high prevalence of 66.7% particularly at L4, a rarely affected segment, thereby suggesting heredity.
A prior report displayed spondylolysis at L5 with spina bifida at L4–S2 in three Japanese brothers of a family (no data of the other members shown). 22 Meanwhile, the current study subjects had no obvious spina bifida, in which pars interarticularis of the vertebral arch were not distinctly attenuated. Therefore, when the cause of spondylosis in the presented cases is considered, it is difficult to completely differentiate pure social factors, activities, and sports injuries from hereditary predisposition. However, the presence of multiple spondylolytic lesions at L4 and L5 indicates a possible inherent genetic weakness of the pars that facilitated stress fracture. It should be noted that familial spondylosis could occur even though the shape of the vertebral arch is apparently normal. Thus, this study findings are still supportive to highlight a genetic bias in lumbar spondylolysis.
In a prior study, the pedigree of a Finnish kindred with spondylolysis was consistent with autosomal dominant inheritance and incomplete penetrance (about 75%). 18 An Iranian family study also drew a similar conclusion. 20 The pedigree of the presented family also indicates an autosomal dominant pattern of inheritance for spondylolysis primarily (Figure 7), although X-linked recessive and Y-linked inheritances are applicable. In X-linked recessive diseases, sons and daughters from the affected father and unaffected carrier mother will have 50% probability to be affected. Generally, Y-linked diseases are rare because of the small size of the Y-chromosome. Y-linked traits are passed only from father to son. We cannot exclude the possibility of these inheritances for spondylolysis in the presented family. However, integrated with prior evidence, this study principally supports an autosomal dominant trait in a subpopulation of patients with lumbar spondylolysis.

Pedigree chart of the family suffering from lumbar spondylolysis. Square indicates men; circle, women; black color, persons with the disease; asterisk, identical twins.
Actually, we proposed formal genetic testing to this family. However, they did not give their consent to the tests because of non-serious symptoms which did not require surgery. Nevertheless, this study indicates a high demand of genetic studies for spondylolysis. This could be highly informative if whole genome sequencing was performed between the affected and unaffected family members. Recently, only a study identifying autosomal dominant SLC26A2 mutations in patients with dysplastic spondylolysis has been reported. 23 However, to date, there is no report of specific mutations in patients with isthmic spondylolysis which are much more common. Further investigations need to be conducted.
Conclusion
We report four cases of spondylolysis at L4, a rare occurrence segment, from two generations of six members in a family—the father and three sons but not the mother and daughter (66.7%). These familial cases suggest autosomal dominant inheritance as the primary genetic predisposition of lumbar spondylolysis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.