
Abstract
Purpose:
Reconstruction of the anterior cruciate ligament (ACL) is the most frequently performed reconstructive surgery in the knee. Biomechanical studies have shown that double bundle (DB) reconstruction is better than single bundle (SB) reconstruction with regard to rotational stability. It is postulated that resection of ACL fibres that remain in continuity may be counterproductive for the knee as these fibres have the capacity to produce collagen. In this study, we aimed to evaluate the efficacy among selective bundle, DB and SB ACL reconstructions over a 2-year post-operative follow-up period.
Methods:
A retrospective comparative study was conducted for comparison between selective bundle, DB and SB reconstructions. Between 2012 and 2014, 291 ACL reconstructions were performed. Of these, 68 patients had selective ACL reconstructions (group SLB), 147 had DB ACL reconstructions (group DB) and 76 had SB ACL reconstructions (group SB). Institutional Review Board approval was obtained, and all patients provided informed consent. Clinical results were assessed with the International Knee Documentation Committee (IKDC), Lysholm and Tegner scores. Stability was measured using Lachman, pivot shift and anterior drawer stress tests using the KT1000 at 30° of knee flexion.
Results:
There was no significant difference in ligament grade, function grade, IKDC grade, as well as Tegner and Lysholm means among all three groups after a 2-year follow-up period.
Conclusion:
Selective bundle reconstruction provides comparable results to DB and SB reconstruction techniques. It is a viable alternative for patients with partial tears.
Introduction
Reconstruction of the anterior cruciate ligament (ACL) is the most frequently performed reconstructive surgery in the knee. 1 The goals of ACL reconstruction are the restoration of normal knee anatomy and function, re-establishment of biological and biomechanical homeostasis and prevention of osteoarthritis. 2 Recent studies have reported that 63–75% of patients returned to pre-injury sports activity, and only 44% of patients were able to perform competitive sports activity. 3
The ACL consists of two functional bundles: anteromedial (AM) and posterolateral (PL). The AM bundle mostly controls anterior translation of the tibia at more than 45° of flexion, while the PL bundle is non-isometric, more oblique, and plays a fundamental role in rotational stability between 0° and 30° of flexion. 4 While the AM bundle is taut throughout range of motion (ROM) with maximum tension between 45° and 60° of knee flexion, the PL bundle is primarily tight in extension. 5
Partial ACL tears account for 10–35% of all ACL lesions, and symptomatic partial lesions account for only 5–10%. 6 The wide range of percentage of incidence of partial tears might be because partial ruptures of the ACL may evolve to complete tears secondary to necrosis of the intact fibres produced by blood supply interruption. 7
The definition of a partial ACL tear remains controversial in the current literature. The American Medical Association defines a partial tear on the clinical assessment, 8 while other studies base it on the percentage of ACL remnant 9 and on arthroscopic evaluation. 10 Yet another study based the definition on a multifactorial definition with an asymmetric Lachman test, a negative pivot shift, differential KT1000 laxity equal to or less than 3 mm and the results of an arthroscopic examination. 11 Also, the accuracy of standard magnetic resonance imaging (MRI) in the diagnosis of partial tears is low, ranging from 25–53%. 12
In recent years, it is postulated that resection of ACL fibres that remain in continuity may be counterproductive for the knee as these fibres have the capacity to produce collagen. 13 Resection of these remnant fibres removes numerous mechanoreceptors that favour knee proprioception. 14
In this study, we aimed to evaluate the efficacy of selective bundle reconstruction over complete bundle reconstruction (both double bundle (DB) and single bundle (SB) reconstruction) over a 2-year post-operative follow-up period.
Materials and methods
A retrospective comparative study was conducted for comparison between selective ACL reconstruction and complete ACL reconstruction, in the form of DB and SB reconstructions.
Between 2012 and 2014, 291 ACL reconstructions were performed. Of these, 68 patients had selective ACL reconstructions (group SLB), 147 had DB ACL reconstructions (group DB) and 76 had SB ACL reconstruction (group SB). Institutional Review Board approval was obtained, and all patients provided informed consent.
All patients who underwent the reconstruction had positive clinical feature of ACL laxity and/or MRI findings of ACL tear. A relatively intact ACL remnant on arthroscopic examination, which was focused on the proximal segment, would be classified as a partial ACL tear. This arthroscopic examination was done in 90° of knee flexion for the AM bundle, and in a figure-of-4 for the PL bundle. All the patients with partially torn ACLs underwent selective reconstruction. The patients with completely torn ACLs had either DB or SB reconstructions depending on surgeon’s preference.
Exclusion criteria included the following: (1) multiple ligamentous injuries (posterior cruciate ligament, PL corner injury, medial collateral ligament injury requiring surgical repair or reconstruction), (2) revision ACL reconstruction and (3) previous injuries or associated fractures of the lower extremity.
Surgical technique
DB ACL reconstruction
A four-strand semitendinosus graft was used for the AM bundle and a four-strand gracilis tendon graft was used for the PL bundle. The femoral tunnel was placed using an arthroscope inserted through the anterolateral portal and a femoral guide through the AM portal. The tip of the guide pin was pointed at the central portion of the footprint of each bundle. The AM bundle was placed at 2 or 10 o’clock position of the notch and the PL bundle was placed 5 mm above the tibiofemoral contact point with the knee flexed at 90°. The tibial tunnels were placed with the guide pins in the central portion of each bundle using the tibial spines and menisci as landmarks.
Selective bundle ACL reconstruction
The intact remnant bundle of the torn ACL was preserved and the ruptured bundle was carefully debrided (Figure 1). The AM bundle was assessed with the knee in 90° of flexion and the PL bundle was assessed in a figure-of-4 position. The tunnels were positioned in the same way as in the DB technique. Care was taken to preserve intact remnant bundle during the tunnel preparation.

Selective bundle reconstruction of left knee with debridement of torn bundle and preservation of intact bundle.
SB ACL reconstruction
After debriding all torn ACL, a quadrupled hamstring graft of both the semitendinosus and gracilis tendons was used to reconstruct the ACL in its anatomical position. A femoral tunnel was sited at the 2 or 10 o’clock position with an offset guide through a transportal approach. The tibial tunnels were placed with the guide pins in the central portion of each bundle using the tibial spines and menisci as landmarks.
Post-operative rehabilitation
All patients followed the same rehabilitation protocol. This consisted of immediate active quadriceps isometric exercises and active ROM exercises. Patients were allowed to fully weight-bear as tolerated on post-operative day 1 in a knee brace. Ninety degrees of motion was allowed 4 weeks after surgery. At 6 months after surgery, straight-line running was allowed, and 9 months after surgery, changing the direction while running was allowed. Return to full sporting activity was allowed at 1 year after surgery.
Evaluation method
Clinical results
Clinical results were assessed with the International Knee Documentation Committee (IKDC), Lysholm and Tegner scores. Stability was measured using Lachman, pivot shift and anterior drawer stress tests using the KT1000 at 30° of knee flexion.
Statistical analysis
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS 19, IBM, USA). Pearson’s χ2 test, Mann–Whitney U test and the Student’s t-test were used to analyse clinical results. p Values of <0.05 were considered statistically significant.
Results
Group SLB consisted of 54 male and 14 female patients, with a mean age of 29 ± 7 years. Group DB consisted of 105 male and 42 female patients, with a mean age of 27 ± 7.5 years. Group SB consisted of 63 male and 13 female patients, with a mean age of 29 ± 8.8 years. Preoperative demographic data, ROM grade, ligament grade and prevalence of associated injuries did not differ statistically between groups.

IKDC: International Knee Documentation Committee.
ROM grade (IKDC)
The ROM grade is recorded from the lowest score obtained in the ROM category of the IKDC questionnaire. At pre-op, 6 months, 1 year and 2 years, the ROM grade was not statistically different between the three groups.
Ligament grade (IKDC)
The ligament grade is recorded from the lowest score obtained in the ligament category of the IKDC questionnaire. This ligament grade was statistically different between the three groups (Tables 1 and 2). At 1 year, group SLB had the highest proportion of patients with ligament grade A, when compared to both group DB (p = 0.046) and group SB (p = 0.012). Anterior drawer, pivot shift and reverse pivot shift showed better results in group SLB, although this was not statistically different between the three groups at baseline and at the 1-year post-operative mark.
Comparison of stability results between SLB and DB at 1 year.
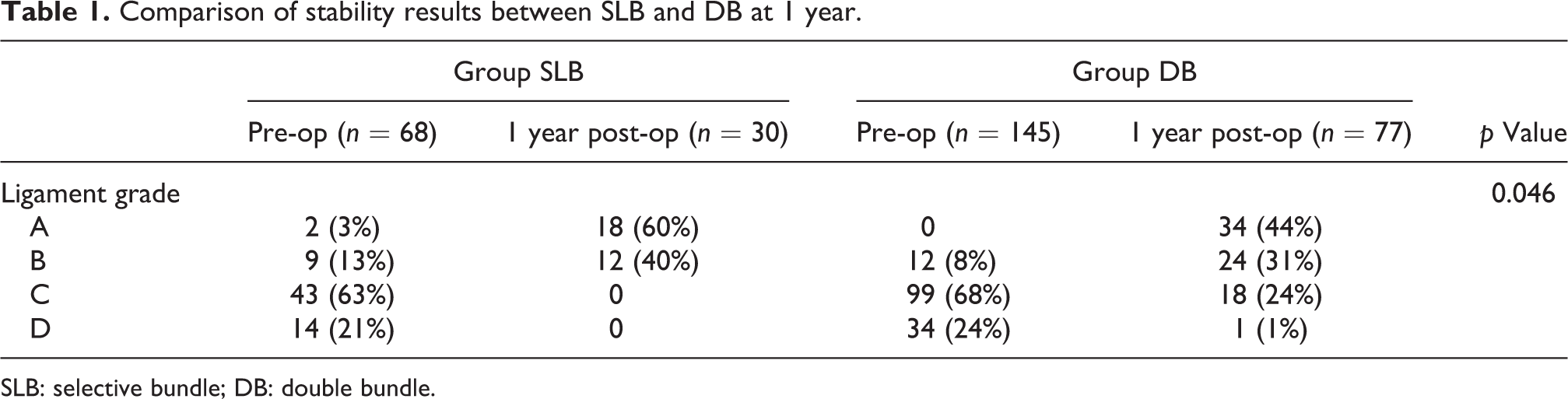
SLB: selective bundle; DB: double bundle.
Comparison of stability results between SLB and SB at 1 year.
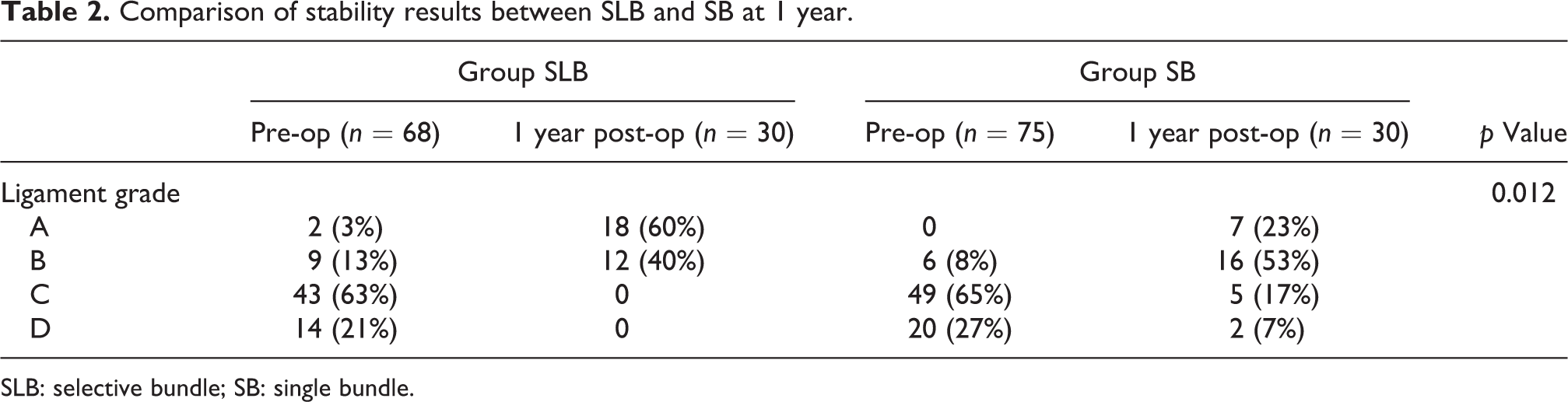
SLB: selective bundle; SB: single bundle.
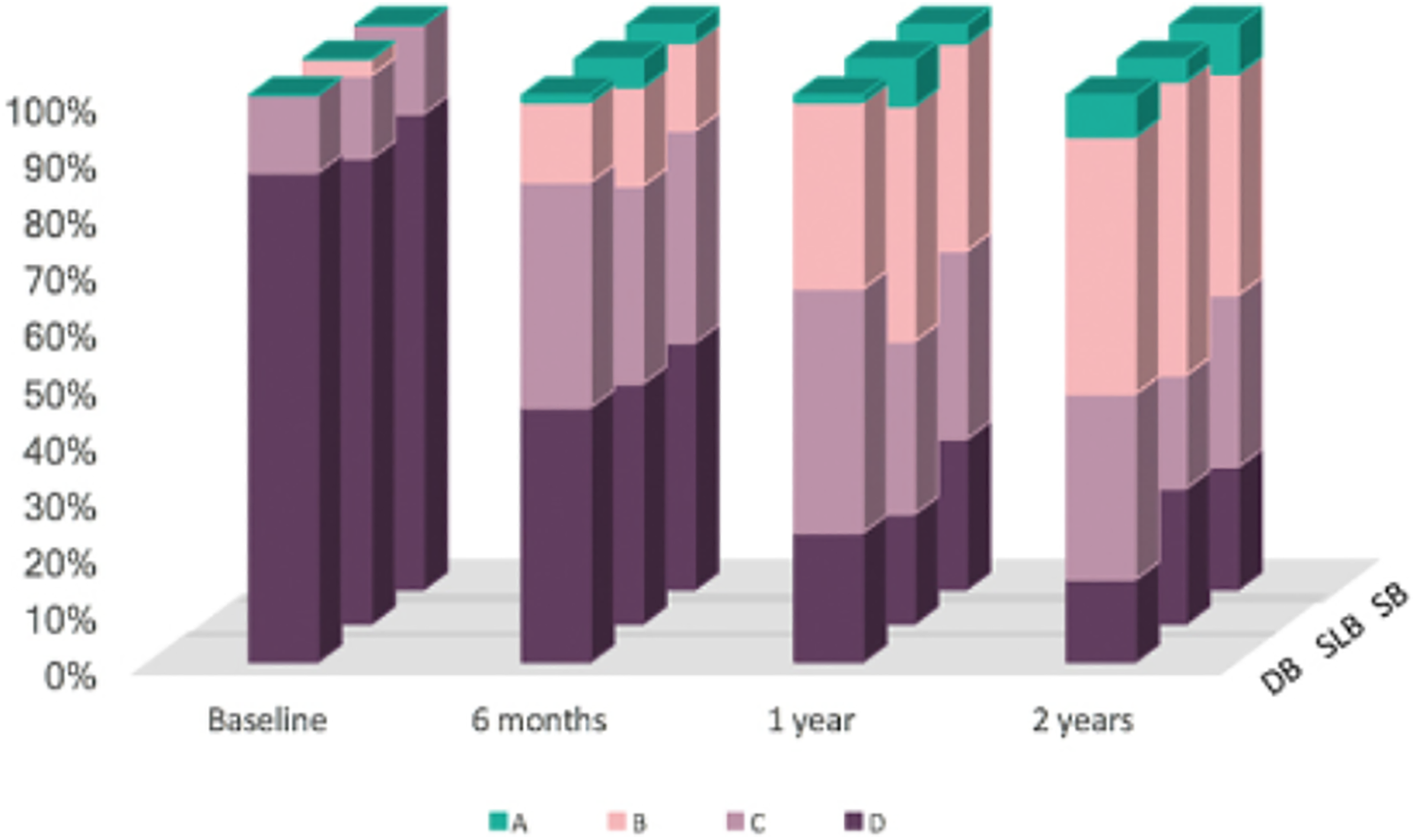
However, after 2 years of follow-up, ligament grade was not statistically different between the three groups (p = 0.662 for group SLB vs. group DB, p = 0.485 for group SLB vs. group SB and p = 0.556 for group DB vs. group SB). Nonetheless, group SLB had the highest proportion of patients with ligament grade A (45.8%), when compared to groups DB (32.1%) and SB (27.3%), as shown in Figure 2.

Ligament grade over 2 years.
KT1000
The KT1000 measurements at 30° of knee flexion were not statistically different between the three groups at pre-op, 1-year and 2-year follow-up. Throughout the 2-year follow-up period, however, group SLB had the lowest mean KT1000 measurement, as shown in Table 3 and Figure 3.
Comparison of KT1000 mean measurements at 30° flexion.

SLB: selective bundle; SB: single bundle; DB: double bundle.

Trend of KT1000 across 2 years.
Function grade (one leg hop)
The one leg hop test is a test of functional stability. This test evaluates the distance covered by the operated knee as a percentage of the normal knee and reflects the integration of neuromuscular control, strength and the patient’s confidence in the knee. Although group SLB had the fastest recovery in the one leg hop test, no statistical difference was found between all three groups at 2 years (p = 0.298 for group SLB vs. group DB, p = 0.456 for group SLB vs. group SB and p = 0.301 for group DB vs. group SB), as shown in Figure 4.

Comparison of functional grade.
IKDC grade
The IKDC grade reflects both the patient’s subjective assessment and objective ROM and ligament grades. At 1 year and 2 years, although not statistically significant, group SLB had a higher proportion of patients with IKDC grade A and B when compared to group DB (52.7%) and group SB (47.8%), as shown in Figure 5 and Table 4.
Comparison of IKDC grade. IKDC: International Knee Documentation Committee.
Comparison of IKDC, Lysholm and Tegner scores.
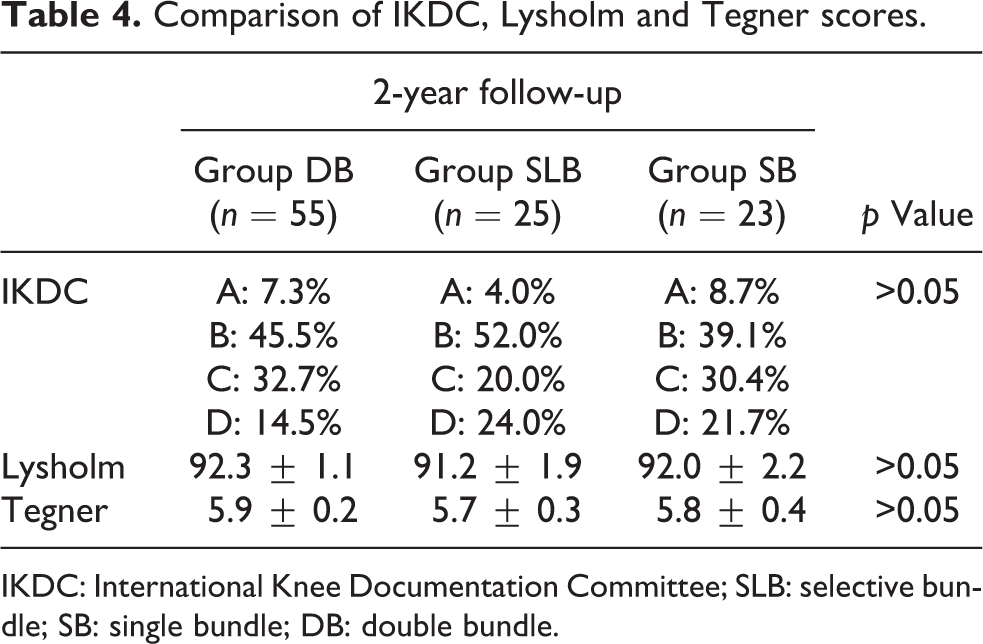
IKDC: International Knee Documentation Committee; SLB: selective bundle; SB: single bundle; DB: double bundle.
Functional tests: Lysholm and Tegner
Lysholm mean scores were not statistically different between all three groups at baseline and at 2-years post-op (Table 4).
At 1 year, Tegner for group SLB (5.4) and group DB (5.3) was superior to group SB (4.8), but the difference was not statistically significant (p = 0.307 for group SLB vs. group SB and p = 0.626 for group DB vs. group SB). At 3 years, the absolute Tegner scores of all three groups were similar (5.7 for group SLB, 5.9 for group DB and 5.8 for group SB), as shown in Table 4.
Re-tear rates
Although there was no significant difference in re-tear rates among the three groups, the percentage of re-tears was significantly higher in group SB (9.2%) than in groups DB (2.7%) and SLB (2.9%), as shown in Table 5.
Comparison of re-tear rates.

SLB: selective bundle; SB: single bundle; DB: double bundle.
On further comparison, group DB had significantly less re-tears than group SB (p = 0.034). Group SLB had less re-tears than group SB, although this was not significant (p = 0.113).
Discussion
Our study confirms that the selective bundle reconstruction technique is at least equivalent to conventional complete bundle reconstruction. This result is consistent with that from current literature. A study comparing selective bundle reconstruction with complete ACL reconstruction concluded that joint stability, joint position sense and Lysholm knee scores improved significantly post-operatively after selective AM or PL bundle reconstruction. 15 This result was supported by another study which compared a group of 40 patients undergoing either AM or PL bundle reconstruction with another group undergoing complete reconstruction, and found that the results were superior in the partial group, both in passive stability and proprioception. 16 Yet another study on selective bundle reconstruction proved that the anatomic augmentation of ACL partial injuries with selective bundle reconstruction showed significant improvement in Lysholm scores and joint stability. 17
Improvement in knee instability could be attributed to ACL remnant scarring on the roof of the notch and the lateral wall of the notch, or on the medial aspect of the lateral femoral condyle, which contributes to the prevention of tibial anterior laxity. 10 Furthermore, nerve fibres might come from the preserved ACL remnant and regenerate mechanoreceptors around the augmented graft, thereby aiding in joint position sense. 18 A positive correlation was also found between the number of mechanoreceptors and the degree of accuracy in detecting joint position. 19 This finding was reproduced in our patients – those who underwent selective reconstruction were found to have better post-operative anteroposterior stability.
Remnant preservation could have potential problems such as (1) increasing the risk of non-anatomic ACL positioning due to poor visualization, (2) technically demanding, (3) cyclops formation and (4) graft passage difficulties. 20 Interestingly, we noted a shorter mean operating time for group SLB (74 min), when compared to group DB (95 min) and group SB (82 min). This could possibly stem from the multitude of factors which influence this parameter, one of which being surgical expertise.
Though not statistically significant, it was noted that group SLB had better preoperative KT1000 findings than groups DB and SB. This could contribute to the improved ligament grade and KT1000 scores at the 1-year and 2-year post-operative mark.
In addition, intuitively, patients in group SLB would have a less injured knee given the higher prevalence of partial tears. This is supported by the lower incidence of associated injuries, such as the presence of fewer meniscus tears and fewer collateral ligament injuries (Table 6). Interestingly, group SLB had more lateral than medial meniscus tears, in contrast to groups DB and SB. This implies that not only was the initial injury less traumatic but a different mechanism was involved.
Comparison of associated injuries.

SLB: selective bundle; SB: single bundle; DB: double bundle; MCL: medial collateral ligament; LCL: lateral collateral ligament.
This suggests that patients with a partial tear may have better outcomes, which may be a result of the different nature of initial trauma, or that of the preserving selective reconstruction technique.
Regardless, this highlights that the profile of a partial tear can be better defined in terms of clinical, radiological and arthroscopic findings. This subgroup could then be better studied for outcomes from different reconstruction techniques.
In our study, MRI findings predicted partial tears with moderate reliability. Group SLB had the highest proportion of partial tears on MRI (57%), when compared to group DB (5%) and group SB (22%). This highlights that arthroscopic findings have to complement the MRI findings in the assessment of a partial tear and that there is still no reliable radiographic means of quantifying a partial tear.
While it has been theorized that partial tears have negative or trace positive pivot shift, 21 our study shows no significant difference in that analysis. Given that the PL bundle has been more closely linked with rotational stability, 22 –24 the prevalence of positive pivot shifts in this subgroup of PLB tears could be further studied.
Another advantage of intact bundle preservation is that it assures mechanical strength in the immediate post-operative period, which is when the graft strength depends primarily on the fixation device. This allows for accelerated rehabilitation and rapid return to sports. This was reflected in superior outcomes for group SLB at 1 year, such as in terms of the ligament grade. In addition, the residual bundle can maintain its blood supply, providing support for the healing process in the graft. 13,25,26 Also, proprioception innervation is maintained which can improve subjective outcome and facilitate a safer return to sports. 7
In a prospective randomized control trial, Jarvela et al. found that DB reconstruction had significantly fewer graft failures at 10 years, when compared to SB reconstruction. 27 This is reflected in our study whereby both groups DB and SLB had fewer re-tears than group SB.
There was a trend across all three groups whereby the ligament grade improved to its peak at 1 year, beyond which there was a slight increase in laxity. This could be attributed to a multitude of factors, including rehabilitation or the effect of return to sports. Although this trend did not translate in terms of KT1000 measurements or functional scores, it can be further studied to optimize long-term outcomes of ACL reconstruction.
The selective bundle reconstructive technique reserves the residual ACL and harvests only one of two hamstring tendons. This may influence the single leg hop test, which reflects the integration of neuromuscular control, strength and patient’s confidence in the knee. Although the results of this test were not statistically significant, group SLB had the highest percentage of patients with grade A at 1 year (68%), when compared to group DB (53%) and group SB (40%).
This study has several limitations, the first of which is selection bias. The group that underwent selective reconstruction had partial tears, which might have translated into better preoperative scores, however, statistically insignificant, that could have contributed to the improved post-operative scores. Second, the loss to follow-up at 1 year is significant in all three groups. Third, there are no definitive criteria for a partial tear and neither is there a stipulated threshold for which a partial tear is considered suitable for a selective reconstruction.
Conclusion
Selective bundle reconstruction provides comparable results to DB and SB reconstruction techniques. It is a viable alternative for patients with partial tears.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.