
Abstract
Purpose:
Synovial membrane inflammation is the most commonly presenting finding during hip arthroscopy and may have a role in the pathomechanism of hip osteoarthritis (OA). The aim of this study was to determine the relationship between synovial cytokine levels and progression of OA after hip arthroscopy.
Methods:
We prospectively examined 20 patients (20 hips) who underwent arthroscopic hip surgery. For all patients, radiographs and severity of pain were evaluated preoperatively. During arthroscopy, we harvested a sample of the synovial membrane and determined the levels of six typical inflammatory cytokines with real-time polymerase chain reaction. We compared the levels of these cytokines in patients who showed OA progression and non-progression after hip arthroscopy.
Results:
Although the average age of patients who showed OA progression postoperatively tended to be higher, there were no significant differences in characteristics involving clinical assessment between patients who showed OA progression and those who showed non-progression. Intraoperative tumour necrosis factor α (TNFα) expression was significantly higher in patients who showed OA progression postoperatively (p = 0.042).
Conclusions:
Elevation of TNFα level might be a predictor of OA progression after hip arthroscopy.
Keywords
Introduction
Hip arthroscopy provides excellent visualization of not only the articular surfaces of the hip joint but also the peritrochanteric, or extra-articular, space around the hip. 1,2 In recent years, this surgery has been reported as having a high degree of utility in treating hip disease and has become a good treatment option. 3 Although existence of hip dysplasia and/or a high-grade chondral injury have been reported as factors that indicate osteoarthritis (OA) progression following hip arthroscopic surgery, 4,5 the preoperative assessment of chondral injury might be difficult with the routine preoperative investigations (e.g. plain radiograph, magnetic resonance imaging (MRI) and computed tomography).
Synovial membrane inflammation is the most commonly presenting finding during hip arthroscopy. Synovial hyperplasia is present in patients with knee pain and OA much more often than in people with OA but without pain. 6 We considered that a reason for progression of OA in some patients may be the presence of inflammatory cytokines within the synovial membrane, which may stimulate nociceptors and signify pathological processes in the hip joint, as has been reported for the knee joint. 7 –9 However, there have been few studies evaluating the cytokine levels in the hip joint. Furthermore, there have been few studies concerning synovial membrane inflammation in patients who underwent hip arthroscopy.
To evaluate whether elevation of synovial cytokine could be a predictor of OA progression after hip arthroscopy, we investigated the relationship between synovial cytokine levels at the time of hip arthroscopy and postoperative OA progression.
Materials and methods
Patients
We obtained approval from our Institutional Review Board for this study, and it has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. Written informed consent was obtained from all participants. We prospectively included 20 patients (20 hips) who were scheduled for arthroscopic hip surgery. Patients who were 60 years and older, with less than 1-year follow-up, and who were diagnosed as having OA with Tönnis grade 3 or higher, with inflammatory disease such as rheumatoid arthritis (RA) and purulent arthritis or with synovial chondromatosis, were excluded from this study. All patients complained of groin pain, restricted hip motion on flexion and internal rotation and had positive anterior impingement test.
Our indications for arthroscopic hip surgery were labral tears and/or increased synovial fluid identified with preoperative MRI and pain relief with 10-ml injection of 0.5% procaine hydrochloride into the hip joint at the initial visit. All patients were resistant to conservative treatment with medication and physical therapy, which was indicated for at least 3 months. As we have empirically established that physical therapy was the most effective conservative treatment for patients with labral tear, including femoroacetabular impingement (FAI), and a report supports our experience, 10 none of the patients were medicated with nonsteroidal anti-inflammatory drugs or steroids in those 3 months. For all patients, age, sex and clinical history were recorded. Physical examination, anteroposterior (AP) and cross-lateral plain radiographs and MRI were evaluated. The pain component of the modified Harris Hip Score (mHHS) and visual analogue scale (VAS) score at rest and on walking were evaluated preoperatively by a physical therapist. 11
The centre–edge (CE) angle of the hip joint was measured using an AP plain radiograph. AP plain radiographs of the hip joint were assessed for the presence of coxa profunda, protrusio acetabuli and CE angle ≥40°, which are indicators of a deep socket, a crossover sign known to be an indicator of acetabular retroversion. The femoral α angle was measured; hip joints with a femoral α angle ≥55° were described as having cam deformity. Hip joints with deep socket, acetabular retroversion and/or femoral cam deformity were described as FAI. 12 Hip joints with CE angle <20° were described as acetabular dysplasia. OA progression was assessed radiographically according to the Tönnis classification system, 13 with comparison between the AP hip radiograph at the time of surgery and at the last follow-up. All radiological assessments were independently performed by two observers. The mean CE angle value as calculated by each reviewer was recorded. In cases of disagreement regarding the definitions of FAI and OA grade, the observers reviewed the radiographs together and conferred until agreement was reached.
Sampling
During hip arthroscopy, patients were placed in the supine position on a fracture table. Two portals (anterolateral and mid-anterior) were used in all cases. We harvested a sample of the synovial membrane from the site of strongest synovitis for further evaluation when we performed the capsulectomy.
Isolation of RNA and quantitative real-time PCR
Total RNA was extracted from harvested synovial samples using TRIzol (Invitrogen, Carlsbad, California, USA) according to the manufacturer’s instructions and was used as a template for first-strand complementary DNA (cDNA) synthesis using SuperScript III RT (Invitrogen). The polymerase chain reaction (PCR) mixture consisted of 2 μL cDNA, the specific primer set (0.2 μM final concentration) and 12.5 μL SYBR Premix Ex Taq (Takara, Kyoto, Japan) in a final volume of 25 μL. The sequences of the PCR primer pairs are listed in Table 1. Quantitative PCR was performed using a real-time PCR detection system (CFX-96; Bio-Rad, Hercules, California, USA). The PCR cycle parameters consisted of an initial denaturation at 95°C for 1 min, followed by 40 cycles of 95°C for 5 s and 60°C for 30 s. Messenger RNA (mRNA) expression was normalized to the level of GAPDH (Glyceraldehyde 3-phosphate dehydrogenase) mRNA.
Sequences of the primers used in this study.
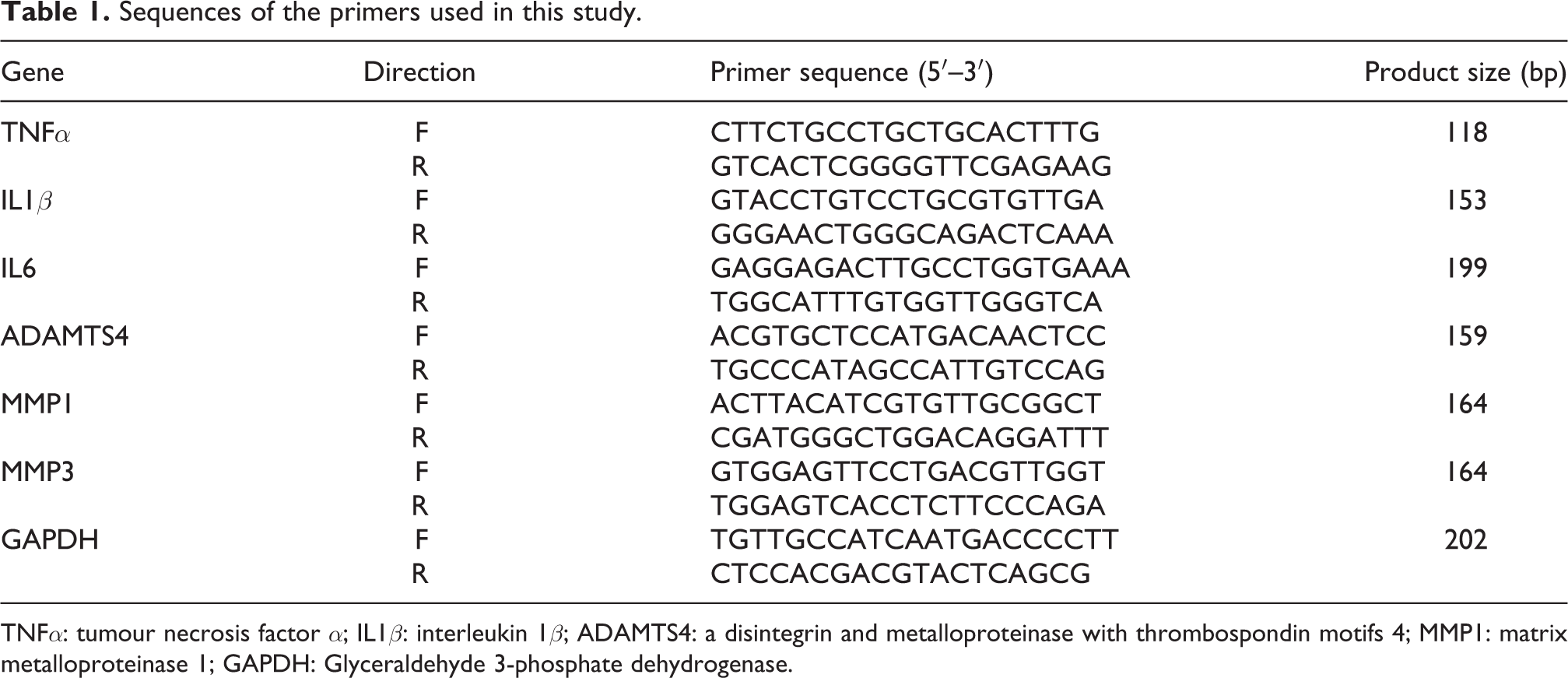
TNFα: tumour necrosis factor α; IL1β: interleukin 1β; ADAMTS4: a disintegrin and metalloproteinase with thrombospondin motifs 4; MMP1: matrix metalloproteinase 1; GAPDH: Glyceraldehyde 3-phosphate dehydrogenase.
Six molecular biomarkers of inflammation within the synovium were measured: tumour necrosis factor α (TNFα), interleukin (IL) 1β, IL6, a disintegrin and metalloproteinase with thrombospondin motifs 4 (ADAMTS4), matrix metalloproteinase 1 (MMP1) and MMP3.
We investigated the relationship between OA progression and cytokine levels in the synovial membrane.
Statistical analyses
Statistical analyses were performed using JMP version 11.0 software (SAS Institute, Cary, North Carolina, USA). Results are expressed as the mean and the standard error of the mean unless otherwise indicated. The results were compared between the two groups (OA progression vs. non-progression). A non-parametric Mann–Whitney U test was used for comparisons of normally distributed data among the groups (age, VAS, mHHS and levels of cytokines). Sex, OA grading and positive radiographic findings of FAI were statistically compared between the groups using Fisher’s exact test. The values of p < 0.05 were considered statistically significant.
Results
In 20 patients (20 hips), there were 7 men (7 hips) and 13 women (13 hips) with an average age of 42.9 ± 3.0 years. None of the patients had diabetes, but one patient had angina and another patient had ulcerative colitis. Their mean preoperative VAS score was 27.5 ± 4.0 during rest and 56.2 ± 4.5 on walking. Their preoperative mean mHHS score was 60.8 ± 2.0. In plain radiographs, 12 hips (60.0%) were classified as Tönnis grade 0, 5 hips (25.0%) as grade 1 and 3 hips (15.0%) as grade 2. Twelve hips (60.0%) were investigated for radiographic findings related to FAI. No hips were described as having acetabular dysplasia.
At the time of the last follow-up (mean: 25 months after the operation), four hips (20%) showed OA progression. There was no disagreement between the observers on the cases which showed OA progression. None of the patients needed further operation such as total hip arthroplasty (THA). The differences of characteristics in patients who showed OA progression and non-progression are shown in Table 2. There was no OA progression in men (seven patients). Among the characteristics of patients, only preoperative OA grading showed a significant correlation with postoperative OA progression (p = 0.016). In addition, the average age of patients who showed OA progression postoperatively tended to be higher (p = 0.06).
Characteristics of the patients who showed OA progression and non-progression.
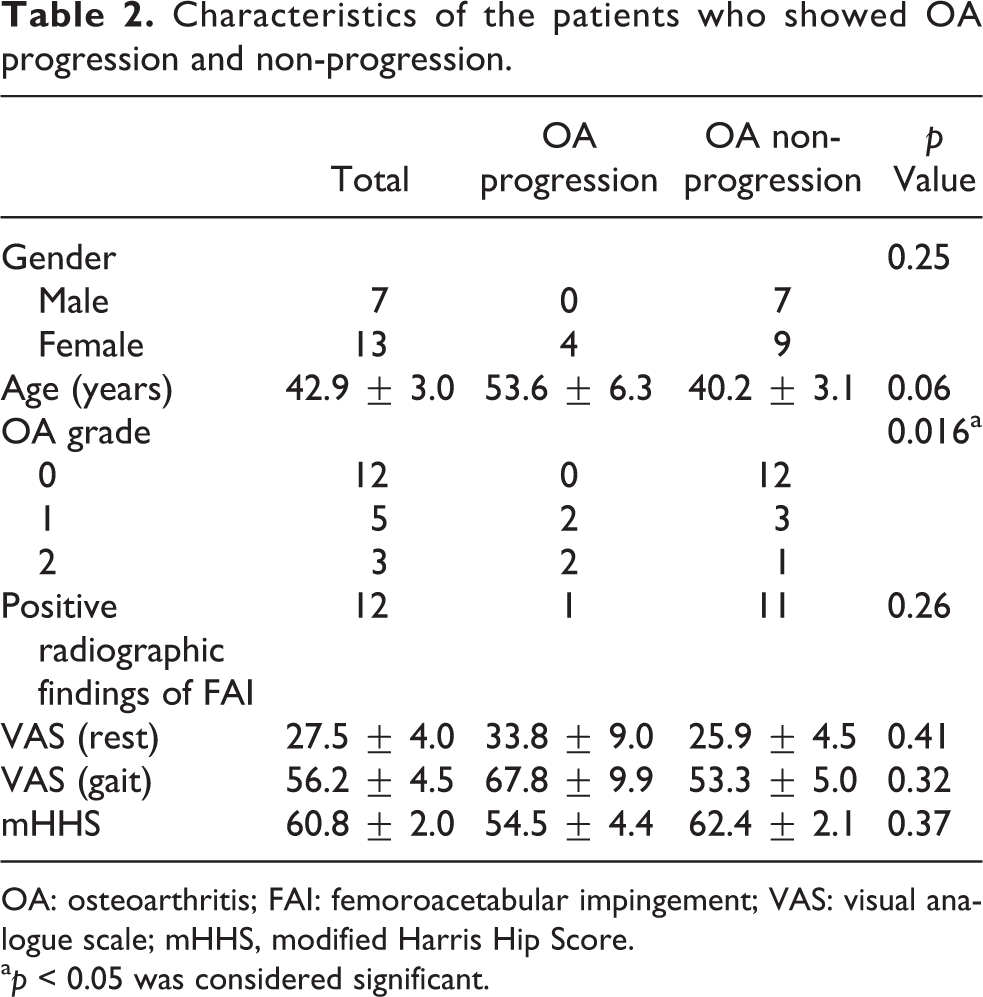
OA: osteoarthritis; FAI: femoroacetabular impingement; VAS: visual analogue scale; mHHS, modified Harris Hip Score.
a p < 0.05 was considered significant.
Comparison of cytokine levels in synovial membrane between OA progression group and non-progression group
We determined the synovial membrane cytokine levels and compared the values between the OA progression group and the non-progression group (Table 3). Only the value of TNFα was significantly higher in the patients who showed OA progression postoperatively than in the patients who showed OA non-progression (p = 0.042).
Levels of cytokine in the OA progression and non-progression groups.

OA: osteoarthritis; TNFα: tumour necrosis factor α; IL1β: interleukin 1β; ADAMTS4: a disintegrin and metalloproteinase with thrombospondin motifs 4; MMP1: matrix metalloproteinase 1.
a p < 0.05 was considered significant.
Discussion
Hip arthroscopy is considered to be a very effective method for examination and treatment of joint disorders, and the use of hip arthroscopy is increasing. Hip arthroscopic treatment has been described as providing good clinical outcomes, low rates of complications and relatively rapid rehabilitation. 1,2,14,15 In an earlier study, McCarthy et al. 5 reported that the patient’s age at arthroscopy and Outerbridge grades (i.e. status of chondral injury) independently predicted OA progression. Domb et al. 16 performed systematic review to assess the extent of preoperative OA which can benefit from hip arthroscopy. They reported that the cases that were recognized as Tönnis grade 1 and better or had a joint space of more than 2 mm should be considered for arthroscopic treatment. In the current study, although the average age of patients who showed OA progression postoperatively tended to be higher, and there were no significant differences in characteristics involving clinical assessment in patients who showed OA progression and non-progression. However, preoperative OA grading showed a significant correlation with postoperative OA progression. There were no OA progression cases among those recognized as Tönnis grade 0 preoperatively. We observed 40% OA progression in grade 1 and 66.7% OA progression in grade 2 cases. As reported previously, preoperative OA grade might be an apparent predictor of postoperative OA progression.
As mentioned previously, synovial membrane inflammation is the most commonly presenting finding during hip arthroscopy. In the current study, we attempted to reveal whether the synovial cytokine levels at the time of hip arthroscopy might be a predictor of OA progression after the operation. In our results, only the value of TNFα was significantly higher in the patients who showed OA progression postoperatively. TNFα is widely considered as a pro-inflammatory cytokine because of its principal role in initiating the cascade of activation of other cytokines in the inflammatory response. 17 TNFα has been reported as a key inflammatory cytokine involved in the pathophysiological processes occurring in the course of OA and RA. 17 –19 TNFα blocks the chondrocytes’ synthesis of proteoglycan components, protein binding proteoglycans and type II collagen. 20 Activated chondrocytes also produce MMP1, MMP3, MMP13 and ADAMTS4. 21,22 MMPs are important mediators in OA, mediated by cytokines such as TNFα and IL1β, which are produced by synovial macrophages. 23 Among the specific subtypes of MMPs, MMP1 is capable of cleaving collagen type II, and MMP3 is active against other components of the extracellular matrix. 24 ADAMTS4 is also an important inflammatory mediator of OA and has degrading effects on the extracellular matrix. 25 In knee OA, Smith et al. 26 reported that the expression of TNFα mRNA in synovial membranes was positively correlated with the degree of articular cartilage degeneration and severity of synovitis. In hip joints, Abe et al. 27 found significantly higher levels of TNFα, IL1β and IL6 in the joint fluid in patients with severe OA compared with early OA. In a recent study involving intra-articular injections of the anti-TNF antibody infliximab, significant symptomatic relief was observed compared with placebo. 28 Infliximab has also been shown to slow the progression of OA. 29 From our results, TNFα might have an important role in the progression of OA.
It remains unclear why the expression of inflammatory cytokines except TNFα did not show significant differences in the present study. However, in knee OA, an increased concentration of IL-6 has been reported to correlate positively with the intensity of radiographic knee OA. 8 In a recent report that investigated and compared the expression of inflammatory cytokines in the cartilage between patients with FAI who underwent hip arthroscopy and those with severe OA who underwent THA, the expressions of IL1β, IL8 and MMP3 in the synovium were significantly lower in patients with FAI patients than in those with severe OA. 30 These cytokines might be increased during the progressive stage of hip OA, but not in the early stage, for which hip arthroscopy is indicated.
Several limitations of this study warrant mentioning. First, the major limitation of this study is the relatively small sample size. Statistical evaluation was performed in 20 hips, without any control sample from subjects without hip pain or patients with another hip diagnosis. Comparative evaluation with a larger sample size would be needed in the future. Furthermore, power analysis, which was not performed in this study, should be evaluated in the future. In addition, we did not assess pathological findings during hip arthroscopy. To assess the correlations between the pathological findings and the expression of inflammatory cytokines, it would be important to clarify the detailed role of inflammatory cytokines and the pathogenesis of OA progression. Second, the average age of patients who showed OA progression postoperatively tended to be higher (p = 0.06) in this study. Malviya et al. 31 reported that patients aged 50 years or older had a 4.65 times higher risk of requiring hip replacement compared with patients younger than 50 years in a large series of 6395 cases of hip arthroscopy. Chondral quality with ageing might have more effect on OA progression. Future studies with a larger sample are needed.
Conclusions
Elevation of TNFα levels might be a predictor of OA progression after hip arthroscopy.
Footnotes
Acknowledgements
The authors are grateful to Ms. Yuko Onuki for her helpful technical support during this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japan Hip Joint Foundation.