
Abstract
Introduction:
Hip osteoarthritis is an important orthopedic problem frequently observed in the elderly. Acetabular dysplasia (AD) is one of the pathologies that cause coxarthrosis. Nearly 20–45% of primary or idiopathic hip osteoarthritis is linked to AD. In our country, there are few studies on this topic. We measured the center–edge (CE) angle, Sharp’s angle, acetabular depth, and femoral head coverage ratio on pelvis anteroposterior radiographs of patients with primary coxarthrosis and calculated the dysplasia rates.
Patients and method:
Age at surgery and sex of the patients; and CE angle, Sharp’s angle, acetabular depth, and femoral head coverage ratio for both operated and opposite hips were evaluated in 223 total hip prosthesis–performed patients with coxarthrosis. Also the distribution of mean age at surgery, sex of patients, dysplasia rates of operated hips, and bilateral dysplasia rates were calculated.
Results:
The right to left ratio of operated hips was 104/119. Female to male ratio was 163/60 (2.7/1), for those with CE angle below 20° it was 123/30 (4.1/1), and it was 40/30 (1.3/1) with CE angle above 20°. Mean age of patients at surgery was 56.9 (±11.4) years. CE angle less than 20° was found in 68.6% of patients, acetabulum depth less than 9 mm was found in 75.3%, Sharp’s angle was more than 45° in 65.9%, and femoral head coverage ratio was less than 70% in 70.3% of patients.
Conclusions:
We identified a high rate of AD in primary coxarthrosis patients undergoing total hip arthroplasty in the study population.
Introduction
Hip osteoarthritis (coxarthrosis) is frequently observed in the elderly and reduces quality of life. Studies in Europe have found the prevalence of osteoarthritis in those above 55 years varies from 7% to 25% 1 and reduces toward the east. 2 In our country, the prevalence is lower than in Europe. 3
There are many publications on the relationship between coxarthrosis and acetabular dysplasia (AD). Some have found a positive correlation between AD and coxarthrosis, while others have stated that there is no correlation. 1,4 –6 When the AD rate in a normal population is examined, the rates in the Eastern population are higher than those in the Western population. 7 –9
In the literature, nearly 20–45% of primary or idiopathic hip osteoarthritis patients are identified to have AD. 10 –12 But these rates are from Western population.
The aim of our study is to describe the rate of AD in patients with end-stage primary (idiopathic) hip osteoarthritis in our country.
In order to find our dysplasia rates in primary hip osteoarthritis, we retrospectively investigated the files of patients who underwent total hip arthroplasty (THA) due to primary coxarthrosis. The center–edge (CE) angle, Sharp’s angle, acetabular depth, and femoral head coverage ratio, which were used to assess AD, were measured from patients’ pelvis anteroposterior (AP) radiographs and the dysplasia rates of hips undergoing THA due to coxarthrosis were calculated.
Patients and method
Patients with THA performed due to coxarthrosis during a 5-year period were retrospectively investigated. A total of 328 patient files were reached. Patient files without preoperative pelvis AP views, cases of coxarthrosis with a determined etiology (secondary coxarthrosis), and cases with a calculated obturator foramen index on pelvic AP (anteroposterior) X-rays outside of normal limits were excluded from the study. Twenty-five files were not evaluated as preoperative pelvic AP (anteroposterior) X-rays could not be reached. The remaining 303 patient files (medical history, laboratory, and radiological investigation) were examined and the etiology of coxarthrosis was determined for 57 patients (Table 1). For the remaining 246 patients whose etiology was not defined (accepted as primary osteoarthritis), the obturator foramen index was calculated on pelvis AP (anteroposterior) radiographs, as described by Tönnis, to evaluate pelvic rotation. 13 The obturator foramen index is found by taking the ratio of the right obturator foramen transverse diameter to the left obturator foramen transverse diameter. Twenty-three patients outside of normal limits (1.8–0.56) were excluded from the study because extreme rotation was considered to affect our calculations. All the measured hips were end-stage hip osteoarthritis according to the Tönnis osteoarthritis radiologic evaluation system and they were all THA performed. 14 Measurements were done once by one of the authors. A transparent ruler with concentric circles and pencil were used to make the measurements on a conventional pelvis AP (anteroposterior) X-ray using techniques listed below on both operated and opposite hips.
Etiology of secondary coxarthrosis and number of patients.

Wiberg’s CE angle
It is the angle between a line parallel to the longitudinal axis of the body and a line joining the center of the femoral head to the superolateral corner of the acetabulum. 15 In our study, angles of 20° or less were accepted as dysplastic. The modified CE angle better reflects dysplasia (the most lateral part of the subchondral sclerosis is taken as the superolateral corner of the acetabulum), so it was used in our study 16 (Figure 1).

Fifty-year old women with left coxarthrosis. CE angle measurement of both hips. CE: center–edge.
Femoral head coverage ratio
It is the ratio of the length between the innermost point of the femoral head and the outer corner of the acetabulum to the length of the femoral head. Head coverage of 70–100% was accepted as normal. In our study group, 70% or less was accepted as dysplastic 17 (Figure 2).

Fifty-seven-year old men with left coxarthrosis. CE angle measurement of the left hip and femoral head coverage ratio measurement of the right hip. CE: center–edge.
Sharp’s angle
A horizontal line is drawn joining the lowest point of both teardrops. From this point, a second line is drawn to the lateral edge of the acetabular roof. The angle between these two lines is Sharp’s angle (transverse acetabular inclination). In addition to the classic measurement method, there is a modified method using the most lateral part of the subchondral sclerosis. 18 In our study group, 45° and above was accepted as abnormal, hence this modified measurement method was used as it better reflects dysplasia (Figure 3).
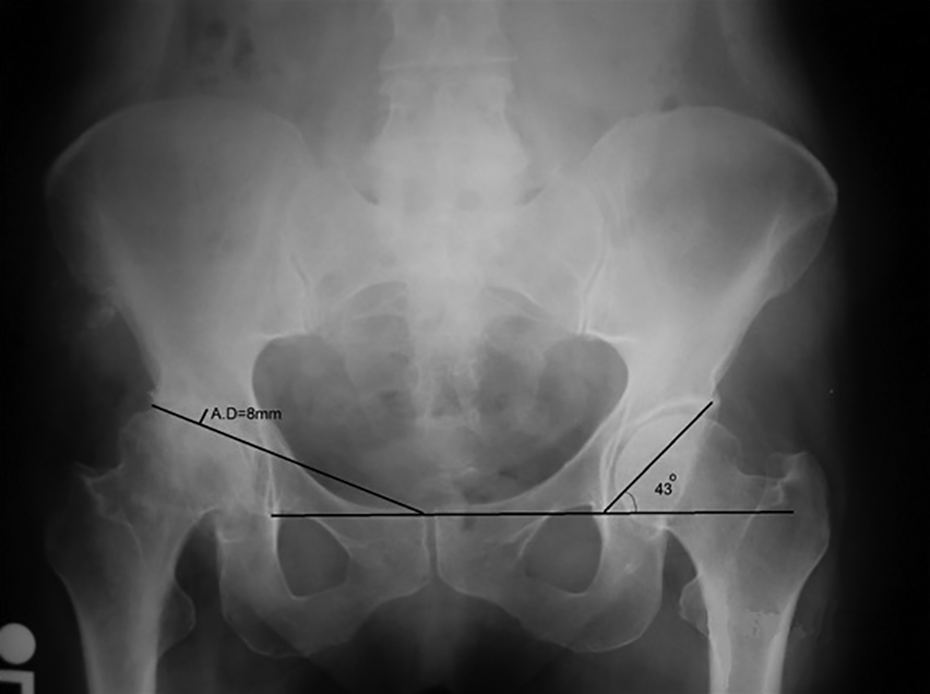
Sixty-two-year old women with left coxarthrosis. Acetabular depth measurement of the right hip and Sharp’s angle measurement of the left hip.
Acetabular depth measurement
A tangent line is drawn from the most lateral edge of the acetabulum to the upper edge of the symphysis pubis on the same side. A perpendicular line is drawn to the deepest point of the acetabulum roof and the distance is stated in millimeters. Values below 9 mm are defined as AD 10 (Figure 3).
The mean age at surgery, surgery side, sex distribution of patients, dysplasia rates of operated hips, and bilateral dysplasia rates were calculated. Statistical evaluation was done using SPSS 16.0 program (SPSS Inc., Chicago, Illinois, USA). Student t-test was used to statistically evaluate the correlation between patients’ age at surgery with CE angle above 20° and those below 20°. The χ 2 test was used to calculate the correlation between sex and surgery side of patients with CE angle above 20° and those below 20°. The Pearson correlation test was used to statistically evaluate the correlation between CE angle values and arthrosis age. Additionally, three groups were created; patients with CE angle 20° and above, CE angle from 10° to 20°, and CE angle below 10°. Ultimately, the one-way analysis of variance (ANOVA) test was used to determine the differences between the groups. Then the Tukey HSD test was used to find the groups causing difference in multiple comparisons.
Results
The distribution of 57 patients with secondary coxarthrosis is given in Table 1. From the remaining 246 patients accepted as primary hip osteoarthritis, 223 cases with obturator foramen index within normal limits were taken for evaluation. Right/left hip ratio of operated hips was 104/119. F/M ratio was 163/60 (2.7/1). F/M ratio in patients with CE angle below 20° was 123/30 (4.1/1), while it was 40/30 (1.3/1) for patients with CE angle above 20°. The mean age of patients at surgery was 56.9 (±11.4) years. When the AD rates were examined, it was 68.6% according to CE angle, 75.3% according to acetabular depth measurements, 65.9% according to Sharp’s angle measurements, and 70.3% according to femoral head coverage ratio measurements. The age at surgery, sex, and side distribution of those who were dysplastic according to CE angle are given in Table 2. The χ 2 test was used to evaluate age, sex, and side differences, whereby no significant difference was found between operation sides (p = 0.386). However, when the female–male ratio and mean age of patients at surgery were investigated, there was a significant difference found between the two groups. The female ratio in dysplastic hips was greater (p = 0.001). Again, the mean age of patients at surgery with dysplastic hips was lower than those without dysplastic hips (p = 0.01).
Age at surgery, sex, and operation side distribution according to CE angle.
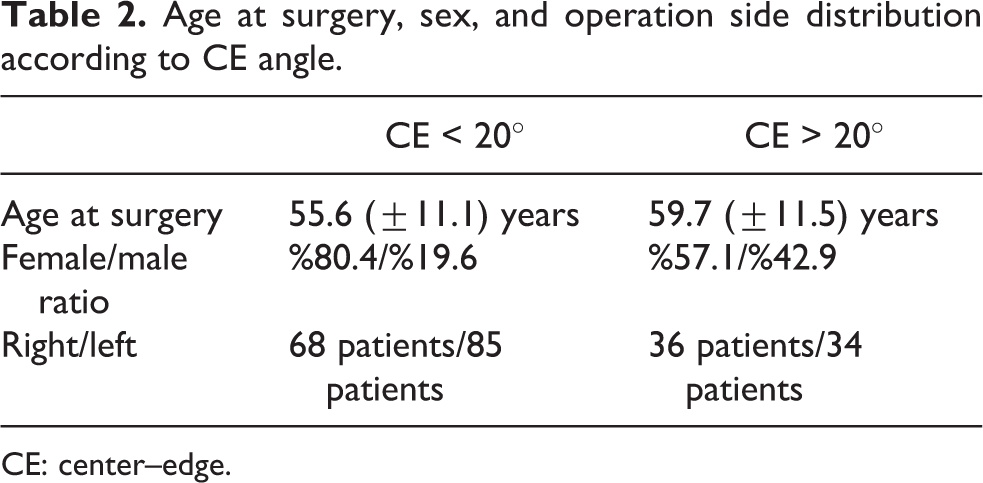
CE: center–edge.
The Pearson correlation test was used to examine whether a significant relationship existed between CE angle and arthrosis age. As the CE angle decreased, the arthrosis age also decreased significantly (r = 0.216; p = 0.001).
Three groups were created according to CE angle: CE angle >20°, CE angle between 10° and 20°, and CE angle <10°. The age difference was examined between the three groups. The one-way ANOVA test found a significant age difference between the groups. The Tukey HSD test was used to determine that the groups causing the difference were the CE angle <10° and CE angle >20° (p = 0.007; Table 3).
Mean age of the patients at surgery according to CE angle.

CE: center–edge.
When we looked at the other hip of patients with CE angle 20° or less, CE angle of the other hips was also 20° or less in 91%. In other words, 91% of patients had bilateral dysplasia.
Of all the patients who were dysplastic according to CE angle, 83.7% were also dysplastic according to Sharp’s angle, 94.8% were also dysplastic according to femoral head coverage ratio, and 95.4% were also dysplastic according to acetabular depth measurements. The χ 2 test was used for CE angle and other measurements, through which a significant positive correlation was found with all measurements (p < 0.001).
Discussion
Coxarthrosis is a common disease, becoming more significant as life span increases. Factors such as age, sex, race, obesity, occupation, trauma, and genetic and developmental deformities are held responsible for the etiology of coxarthrosis. 12
Studies on coxarthrosis in Europe have reported 7–25% prevalence in White Europeans aged 55 years and above. The prevalence is lowest in Asians, while the prevalence is highest in White Europeans. 1
However, studies have found the prevalence of AD is greater in the Eastern population and reduces as you move toward the Western population. Yoshımura et al. found the dysplasia prevalence was significantly lower in England compared to Japan; however, the coxarthrosis prevalence was higher in England. 2 The reasons for this are not fully known; however, it is linked to genetic factors and lower obesity rates in Asians. 19 Our country is a transition zone between Asia and Europe. In this way, it is expected that our coxarthrosis prevalence to be lower than the West, while the AD prevalence is expected to be higher than the West. Göker et al. found that the moderate and severe degree of coxarthrosis prevalence was lower compared to European countries. 3 Studies of normal populations in the West have found AD at 2–5%, whereby in our country this rate up to 10%. 7 –9
In 1924, Le Scolan first discovered the cause–result relationship between hip dysplasia and osteoarthritis. 4 Then in 1939, Wiberg defined the CE angle and succeeded in quantifying dysplasia. 15 Wiberg showed that patients with pathological CE angles developed coxarthrosis and the process of osteoarthritis development was directly related to the reduction in CE angle. Accordingly, the study by Wiberg revealed that patients with mean CE angle of 2° developed coxarthrosis in the fourth decade, those with mean CE angle of 5° developed it in the fifth decade, those with mean CE angle of 10° developed it in the sixth decade, those with mean CE angle of 12° developed it in the seventh decade, while those with angle of 18° developed osteoarthritis in the eighth decade. 4
While there is consensus on the early development of osteoarthritis in subluxated hips, the publications on the relationship of slight dysplasia to hip arthrosis are contradictory. 5 For example, Cooperman et al. determined there was no positive relationship between CE angle and arthrosis age. 4 Contrarily, Reijman et al. determined dysplastic hips were 4.3 times more likely to develop arthrosis, compared to normal hips. 6 Harris-Hayes and Royer, in a review evaluating 20 studies assessing the correlation between AD and osteoarthritis, found that there was a correlation between AD and osteoarthritis development. 20 When we examine the relationship between CE angle and age, statistically there is a significant difference between the mean age of patients with hip dysplasia and those without hip dysplasia. Significantly, as CE angle decreases, the arthrosis age also decreases. The results are parallel to the study by Wiberg. 15 However, the parallel fall in CE angle and arthrosis age was not as dramatic as the studies by Wiberg. There was a nearly 5-year age difference between those with CE angle below 10° (54.38 ± 11.02) and those with CE angle above 20° (59.95 ± 11.44). However, we cannot say CE angle is a prognostic factor in the etiology of coxarthrosis because coxarthrosis is a multifactorial disease. When other parameters (such as occupation, trauma, genetics, and obesity) are used as independent variables, there is a need for more comprehensive studies.
The studies on the AD rate in coxarthrosis are generally from the West. Murray 10 and William and Harris 11 stated that 25–40% of hip osteoarthritis developed secondary to developmental hip dysplasia. Chitnavis et al. identified that after CE angle and acetabular depth measurements on the pelvis AP (anteroposterior) radiographs of patients with primary coxarthrosis in hospital for THA surgery, 40% had hip dysplasia. 12 Uluçay et al. found AD as a cause of coxarthrosis in 43.5% of females and 17.6% of males. In summary, they reported that in 37.1% of cases, coxarthrosis developed secondary to AD. 21 In our study, we found 68.6% according to the CE angle. In our cases, the female–male ratio was 163/60 (2.7/1), while in patients with CE angle below 20° this ratio was 123/30 (4.1/1) and in patients with CE angle above 20° it was 40/30 (1.3/1). The reason for the high female ratio may be linked to our high AD rate and the majority of females in our country have a body mass index above normal limits. Chitnavis et al., in a 312-patient series, gave the female–male ratio as 1.33/1. 12 There was no clear sex difference in primary coxarthrosis patients in the study by Danielsson et al.; however, within these patients the majority of patients with THA were significantly stated to be women. 22 Though it is not fully known why more women have THA operations, the disease may be more progressive in women and this may be linked to a range of hormonal reasons. 23 Uluçay et al. reported that in 886 patients with THA due to coxarthrosis, 75% was female with 24.7% male. 21
In our study, when the opposite hips of patients with CE angle below 20° are investigated, 91% also had CE angle below 20° in the opposite hip; in other words, they were dysplastic.
The high rate of bilateral dysplasia in our cases was unusual according to the current literature. As we know, developmental hip dysplasia is most frequently found in the left hip, with second highest frequency bilateral and third highest frequency in the right hip. 24,25 However, Jacobsen et al. investigated the opposite hip of unilateral dysplasia patients with computed tomography (CT). They found that compared with the CT of a normal control group without hip disease, the normally evaluated opposite hips actually had hidden dysplasia and nearly all the patients were found to have bilateral dysplasia. 26 Additionally, Yurdoğlu et al. identified dysplasia in the opposite hip in 20% of patients with unilateral dysplasia after measurements of the opposite hip. 27 Again, Zorer et al. investigated the diseased and healthy hip of unilateral dysplasia patients with CT and found that both diseased and healthy hips had close values for acetabular anteversion. 28
Our study has some limitations. As it was retrospective, the standards of X-rays may be debated. We have no information on how many patients were standing and how many were lying down during radiography. We know that pelvis AP (anteroposterior) radiography when taken while standing is better at showing arthrosis, compared to those taken while lying down. 29 However, as we did not define coxarthrosis by joint interval measurements, but did a rough definition, we do not believe this will affect our results.
Jacobsen et al. showed that pelvic rotation affects dysplasia measurements in a cadaveric study. 30 We performed obturator foramen index measurements and did not include cases outside of normal limits to prevent inappropriate results.
Another limitation is the classic knowledge that with time, coxarthrosis disrupts the hip affected, causing subluxation. However, we know that the main pathology of coxarthrosis is loss of cartilage. Cartilage loss generally occurs in three ways. The superolateral, medial, and axial migration of the femur head within the acetabulum shows whether cartilage loss affects the whole joint or only a portion. After cartilage loss in the whole joint, the femur head migrates axially. Axial migration shows that all cartilage is affected. This indicates that the cartilage in the joint is affected by inflammatory and deposition diseases. Superolateral and medial migration develops after abnormal mechanical stresses in the hip. With osteoarthritis developing after hip dysplasia, the hip migrates superolaterally. This may cause a slight increase in CE angle; however, this does not prevent us from seeing the underlying pathology. 31
Another limitation is the reality that errors can be made during dysplasia measurements in coxarthrosis patients. For example, finding the center of a deformed femoral head or finding the lateral edge of the acetabulum due to osteophytes is not easy. 1 To reduce our errors to a minimum, all measurements were made by considering the lateral acetabular osteophytes. For this, the subchondral sclerosis was followed laterally. The point where the subchondral sclerosis ends was accepted as the lateral of the acetabulum roof. 32
When measuring the CE angle in deformed femur heads, it is difficult to find the center of the femur head. The decision must be made whether to base measurements on the round or the flattened portion of the femoral head. The central point of the femoral head that bears load and is equivalent to the circular portion of the acetabulum should be taken. 33 Additionally, to reduce measurement errors to a minimum in our study, we measured four values for each hip. In hips considered to be dysplastic according to CE angle, 83.7–95.4% was dysplastic according to the other measurements.
When we investigate the reliability of the chosen measurement methods, we found that these are the most commonly used methods in the literature. Thus, Nelitz et al., in 100 unilateral hip dysplasia patients, investigated CE angle, Sharp’s angle, acetabular index of the load-bearing portion, acetabular depth ratio, ACM angle, MZ distance, femoral head coverage ratio, lateral subluxation, and neck shaft angle on pelvis AP radiographs. They found high reliability for all measurements, except ACM angle, acetabular depth ratio, and MZ distance, both by the same observer and between observers. 34 Additionally, Chitnavis et al. stated that the CE angle was a repeatable parameter even in hips with arthrosis. 12
In conclusion, we identified a high rate of AD in primary coxarthrosis patients undergoing THA in the study population. We believe our study provides some information about the relationship between primary coxarthrosis and AD in our country. However, prospective, controlled studies with other causes of coxarthrosis used in the literature (e.g. heredity, body mass index) as statistical variables and larger series are required to research the relationship between coxarthrosis and AD.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.