
Abstract
Introduction:
Rotator cuff (RC) tears are common and a frequent cause of dysfunction in the shoulder, especially with progression of age. Biceps pathology occurs concomitantly and its relationship with RC tears has been well described. However, the study of biceps intervention affecting outcomes of RC repair is limited. We aim to study the effect of biceps tenotomy in RC repair after matching for cuff tear size.
Methods:
We collected data of 24 consecutive patients undergoing RC repair and biceps tenotomy and matched them with patients undergoing RC repair only (n = 24). The groups were matched for age, RC tear size, and presence of subscapularis tears. All patients of this study underwent RC repair under a single surgeon. Patient demographics and outcome measures in the form of range of motion (ROM) pain scores and validated shoulder scores (Constant shoulder score, Oxford score, and University of California Los Angeles shoulder score) were collected preoperative and at predetermined fixed intervals up to 2 years postoperatively. We then compared the two groups using a mixed analysis of variance design so as to identify any possible differences.
Results:
Patients from both groups demonstrated significant improvement in ROM, lower pain scores, and improvement in functional outcomes (p < 0.05). Patients with biceps intervention demonstrated equivalent outcomes postoperatively up to 2 years with no statistical differences (p > 0.05).
Conclusion:
Arthoscopic RC repair is an effective intervention for improving ROM, reducing pain, and improving function. Concomitant biceps procedure did not negatively impede recovery or affect outcomes.
Introduction
Rotator cuff (RC) tears are common and a frequent cause of dysfunction in the shoulder, especially with progression of age. 1 Surgical repair is a cost-effective solution 2 that offers effective pain relief with good patient satisfaction. 3 Arthroscopic and open modalities demonstrated comparable outcomes 4 although arthroscopic methods are favored among surgeons. 5
The study of biceps intervention together with RC repair is limited even though they frequently occur together. 6 –9 We found two other studies discussing this relationship. Nho et al. prospectively studied 193 patients with RC tears and found that biceps pathology did not affect clinical outcomes of arthroscopic RC repair. 10 Similarly, Kukkonen et al. reported no difference in constant scores 1 year after RC repair with and without biceps tenotomy. 11
Biceps pathologies had been reported to affect 63–76% of patients suffering from RC tears and degree of biceps pathology directly correlating with tear size. 6,8 As biceps pathology reportedly contributes to anterior shoulder pain, 12,13 there are concerns that leaving it untreated in RC repair would result in suboptimal postoperative outcomes. Hence, our study aims to compare outcomes of patients with and without biceps tenotomy after matching for tear size and study for this relationship.
Methods
This is a retrospective review of prospectively collected data for patients with midsize RC tear who underwent biceps tenotomy and RC repair under a single surgeon from 2010 to 2014. Midsize RC tear was defined as tear size between 1 cm and 3 cm. 14 The surgeon of this study performed 307 arthroscopic midsize RC tear repairs during this period. Of which, 30 (9.77%) patients required biceps tenotomy—6 of these patients were excluded due to lack of follow-up data at 2 years postoperation. The remaining 24 cases were matched for age, gender, and presence of subscapularis tear with patients undergoing midsize RC repair without biceps tenotomy from the same surgeon. The patients in this study did not undergo previous RC repair, biceps tenodesis, or any other surgical procedure on the affected shoulder.
There is no clear consensus regarding management of biceps pathology. Various reports have demonstrated that tenotomy and tenodesis both yielded comparable results. 15,16 The benefits of biceps tenotomy include a simpler procedure, lesser postoperative rehabilitation requirements, and faster return to activity. 17,18 In this study, biceps tenotomy was performed for patients with an unstable or partially torn (> 25%) biceps long head tendon (BLHT) as conservative observation or debridement for these patients could result in residual pain after RC surgery. 15,19 Biceps tenotomy on the other hand offered these patients definitive treatment. 17,19,20
All patients were treated in the beach chair position. The biceps tendon and RC were first examined with a 30º arthroscope via the posterior portal. Tendon tears were then debrided with an arthroscopic shaver and ablation wand. Margin convergence sutures passed through the tear to reduce strain of subsequent tendon repair. Repair of the RC tear was then achieved via two medial suture anchors at the anatomic neck brought down to a single suture at the footprint on the greater tuberosity between the medial anchors. The stability of the BLHT was assessed statically by looking for dislocation out of the biciptial groove as far as arthroscopically visible in the neutral beach chair position. Dynamic stability was then assessed with an arthroscopic probe by pushing and pulling on the BLHT as well as the anterior and posterior pulleys followed by internal and external rotation of the arm. The tendon was deemed to be unstable if the BLHT was not held in position statically or dynamically. 21 If unstable or partially torn more than 25%, 22 biceps tenotomy was performed according the surgeon’s decision by cutting the BLHT with an arthroscopic scissors at the insertion of the labrum.
Postoperative care was standardized for all patients. This included appropriate oral and parental analgesia and immobilization of the shoulder joint in an arm sling. Patients were discharged from the hospital on the first postoperative day. The arm sling was kept for 2 weeks postoperatively, and after 2 weeks, patients were called back for assessment of wound healing by the operating surgeon. At this point, the arm sling was removed and patients started on postoperative physiotherapy. The first 4 weeks targeted passive range of movement exercises, the next 6 weeks active range of movement exercises, and subsequently strength training exercises.
Specialist’s review was conducted at 2 weeks, 1 month, 3 months, 6 months, 1 year, and 2 years postoperatively. Patient data were collected preoperatively and postoperatively at 3 months, 6 months, 1 year, and 2 years. These data were collected by a specialized data collection center run by experienced physiotherapist.
Age, sex, and medical comorbities were reported by the patients and collected on standardized forms. Range of motion (ROM) in flexion and abduction of both affected and unaffected shoulders were determined using an inclinometer. External rotation and internal rotation were charted according to the Constant shoulder score external and internal rotation components. 23 Functional outcomes were collected using the Constant shoulder score, 23 University of California Los Angeles (UCLA) shoulder score, 24 and the Oxford shoulder score. 25
Quantile-Quantile plot was used to test continuous variables for normality of distribution. Case and control groups were tested for differences using χ 2 test for categorical variables and Student’s t test for continuous variables. Outcomes were compared from preoperatively to 2 years postoperative using a mixed analysis of variance design. All outcomes were tested for independently. All statistical analyses were performed using Statistical Package for Social Science (SPSS) Version 23 (IBM, SPSS Statistics, Armonk, North Castle, New York, USA)
Results
Patient demographics for case and control groups are listed in Table 1. Both groups were well matched for age, gender, and presence of subscapularis tear.
Comparison of demographics in case and control groups.

Patients from both groups improved in ROM, lowered pain scores, and better function scores up to 2 after operation (Table 2). Both groups performed equally with no significant statistical differences in all aspects. Their improvements in ROM can be seen from Figures 1 to 4.
Outcomes of arthroscopic RC repair with and without biceps tenotomy.

RC: rotator cuff; UCLA: University of California Los Angeles.
Bold values signify P < 0.05.
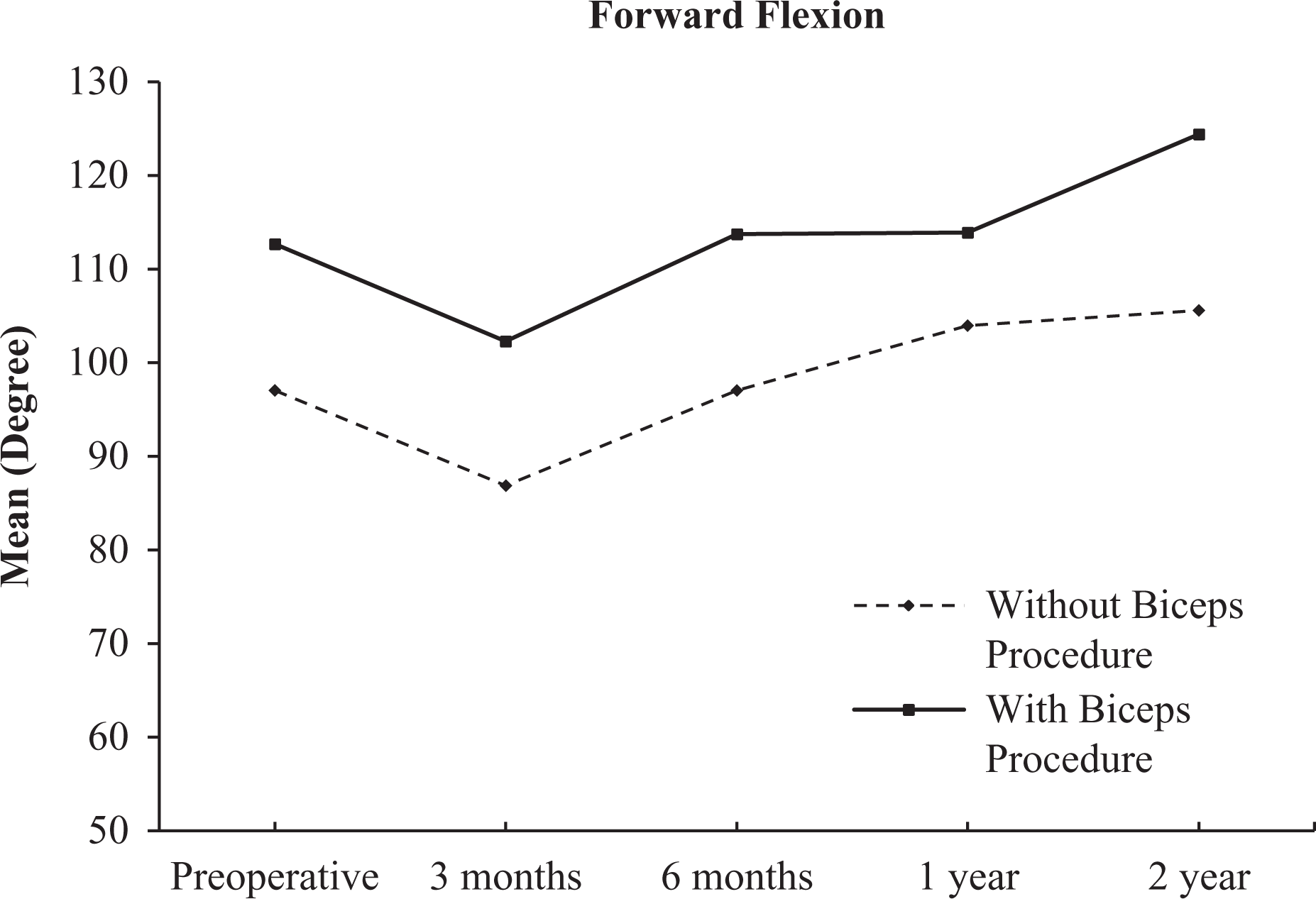
Change in forward flexion over time.

Change in abduction over time.

Change in external rotation over time.
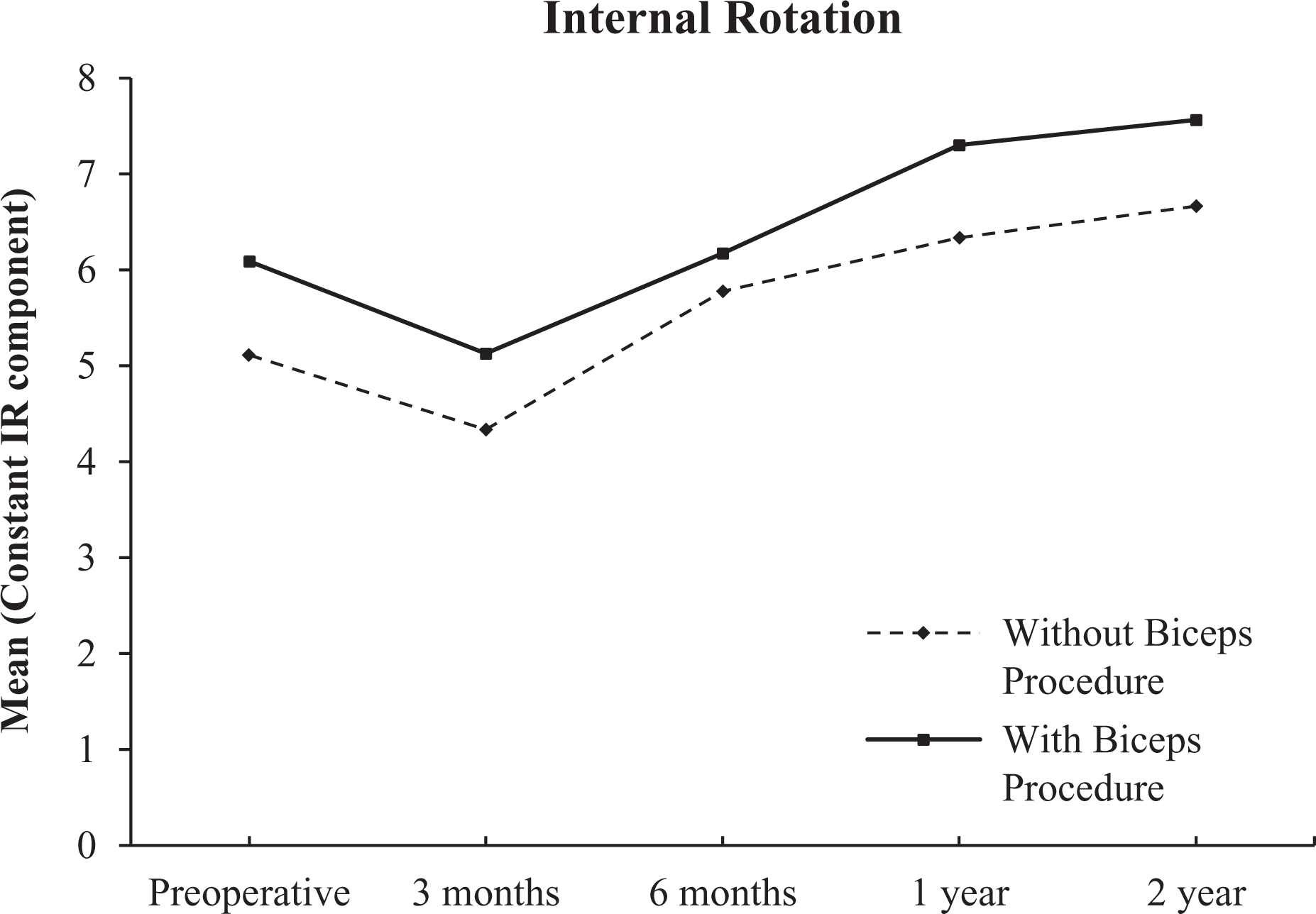
Change in internal rotation over time.
Discussion
Results from our study suggest that BLHT pathology does not affect preoperative or postoperative pain scores. Chen et al. found that in patients with RC tears, 41% had arthroscopic evidence of biceps tendinitis, 8% had biceps subluxation, 10% had biceps dislocation, 12% had partial biceps tendon tear, and 5% had complete rupture of the biceps. 6 Murthi et al. similarly reports that 63% of specimens revealed evidence of microscopic chronic inflammatory changes in the BLHT. 8 Both studies found positive correlation between size of RC and degree of biceps lesion. In our study, we were extremely selective and performed it only in 30 (9.77%) out of the 307 patients with RC tears. The primary surgeon followed strict criteria for tenotomy and only proceeded when the biceps tendon was clearly tendinopathic or unstable. Despite stringent criteria in selecting patients who had clear biceps pathology, our study found no clinical differences in these patients preoperatively and postoperatively. Interestingly, although the BLHT has been described as a source of anterior shoulder pain, 12,13 BLHT pathology has also been reported to be being vague and inconsistent. 26 Lafosse et al. found preoperative tests for biceps pathology to poorly correlate with intraoperative findings. 21 On the contrary, Watson et al. reported significantly poorer preoperative and greater mean improvement in VAS scores for patients undergoing biceps procedure when compared with patients without biceps procedure in his study. 27 However in that study, patients from both groups had statistically significant differences in gender and size of RC tear. Given variable evidence from varying sources, further studies into the role of biceps pathology in shoulder pain are worthwhile.
From our study, biceps tenotomy did not have negative effects on the range of movement and functional outcomes when performed concurrently with RC repair. This is consistent with reports from previous studies. 10,11 There is a belief that the BLHT assists the RC by depressing the humeral head 28,29 and therefore removing the tendon may anatomically and functionally compromise the shoulder joint, 18,19 but Levy et al. and Yamaguchi et al. disputes this and demonstrated from their studies that the BLHT has minimal role in maintaining joint stability. 30,31 Animal model studies report similar findings; there were lesser deforming forces in the shoulder joint and no functional differences after biceps tenotomy was performed. 32,33 Equal outcomes with no negative impact of biceps tenotomy on RC repair should reassure both patients and surgeons to proceed with taking down the BLHT if required or beneficial.
The strength of this study includes use of prospective registry data, standardized data collection methods, uniformed postoperative care, and standardized postoperative rehabilitation. Matching for gender and RC tear size minimized risk of confounder effect between the two groups. Strict criteria and low tenotomy rates selected only for cases with obvious biceps pathology.
We recognize the limitations of a retrospective study, which in its nature is subject to a variety of biases. The use of a single surgeon although limits variability but exposes this study to selection bias.
Conclusion
We conclude that tenotomy of the BLHT in RC repair did not affect preoperative and postoperative pain scores or functional outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.