
Abstract
Purpose:
The cerclage passer instrument was introduced for aiding percutaneous reduction in spiral femur fractures, thereby overcoming the risk of devascularization of the fracture ends commonly associated with traditional open cerclage wiring techniques. This may, however, predispose to iatrogenic vascular injuries owing to the proximity of the vessels and several other factors. We report four cases with femoral artery (superficial and deep) injuries caused by the cerclage passer in proximal femur and distal femur shaft fractures and incidence of these injuries in our institution.
Methods:
Retrospective analysis of hospital records of femoral fractures from 2011 to 2015. All cases of femoral fractures and periprosthetic femoral fractures with cerclage wiring done using the standard or the Synthes® cerclage passer were included. Cases with wiring done for trochanteric fractures and other locations were excluded.
Results:
Incidence of vascular injuries due to the cerclage passer in proximal femur shaft fractures was 1.59%, whereas in distal femur shaft fractures it was 7.14%. There were two patients with a deep femoral artery (DFA) system injury and two with a superficial femoral artery (SFA) injury caused by the cerclage passer (Synthes) in two proximal femur shaft and two distal femur shaft fractures, respectively. End-to-end anastomosis for the SFA and ligation for DFA system injuries were used, with an uneventful postoperative period in all patients.
Conclusion:
Caution and accuracy is imperative to avoid vascular injuries while using the cerclage passer in femur fractures, and strict vigilance is essential for early identification and prompt management.
Keywords
Introduction
Cerclage wiring is occasionally used to aid in the reduction of long spiral fractures of the femur for enhanced stability and to ensure maximum contact surface of fracture ends for rapid bone healing. 1,2 It is, however, associated with the risk of injury to the adjacent neurovascular structures, namely the perforator and the main branches of the deep femoral artery (DFA) and the superficial femoral artery (SFA). 3,4 These vascular injuries can be devastating and pose risk to both life and limb of the patient. 5,6 They may present as acute bleeding owing to laceration of the vessels or have a delayed presentation with a slowly progressive or recurrent swelling, persistent pain, and a fall in hematocrit pointing to a pseudoaneurysm. 5 Regardless of the presentation, they require immediate identification and urgent intervention by a vascular surgeon.
To the best of our knowledge, there are only four reported cases of vascular injury caused by occlusion of the femoral artery due to cerclage wires. 6 –9 All of these were detected postoperatively, as a pale and cool limb with absent pulses, and two of these used the standard wire passer instrument.
A percutaneous cerclage wiring technique using the cerclage passer (Synthes) instrument had been introduced for femoral fractures to overcome the disadvantage of extensive surgical dissection associated with open cerclage procedures, which tends to disrupt the blood supply at the fracture site. 2,9 –11 Cadaver injection studies have shown it to be a relatively safe technique 2 and there are some reports at present implicating it in femoral vascular injuries. 9
This is a comprehensive report of a series of vascular injuries in our institution caused by the cerclage passer (Synthes) along with incidence, management, and an extensive review of the available literature.
Materials and methods
A retrospective analysis of hospital records of femoral fractures from January 1, 2011, to December 31, 2015, managed in a high-volume tertiary care trauma center was done. All patients with femoral fractures and periprosthetic femoral fractures who had cerclage wiring done, using the standard or the Synthes (Depuy Synthes, Switzerland) cerclage passer instrument, in addition to the definitive implants were included. Cases with wiring done for trochanteric fractures were excluded. Written informed consent was obtained from the patients to publish their information and images.
The cerclage passer (Synthes; Figure 1) was introduced in our center in November 2013 and it has been used following the standard technique. 9,11 First, a tunnel was made subperiosteally on the anterior and posterior surfaces of the bone using a 60-mm tunneling device. Then the dorsal followed by the ventral half of the cerclage passer was inserted with a trocar (Figure 1(a) and (b)). Once the two halves of the instrument were engaged and clamped together (Figure 1(c)), the trocar was removed and a stainless steel (SS) wire was passed through the instrument. The two halves were then detached and removed, and the wire was tightened. We used a 60-mm (large) cerclage passer for both proximal and distal femoral shaft fractures as per recommendation. 9,11
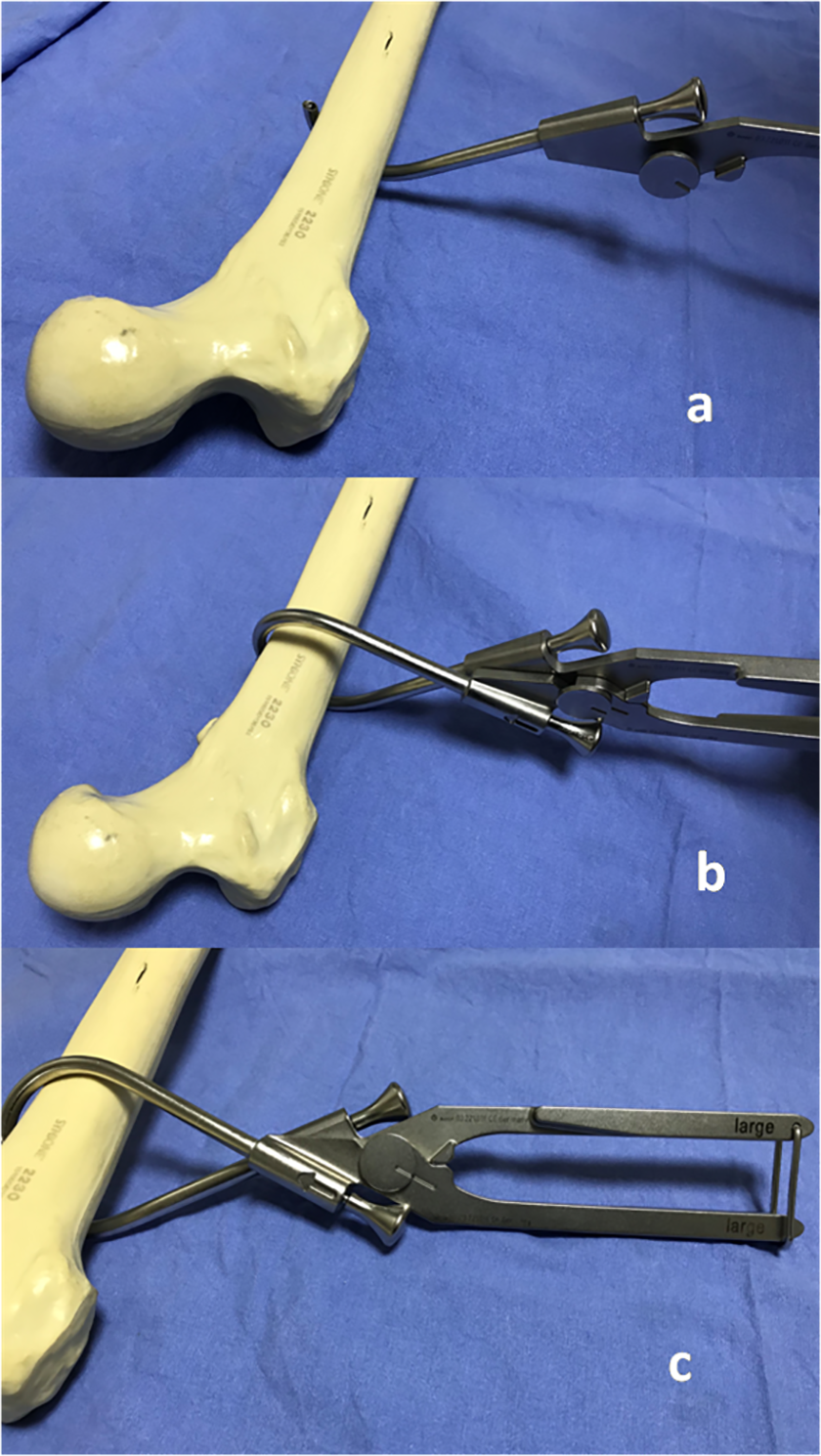
(a) Dorsal half of the cerclage passer inserted after pathway created with tunneling device, (b) ventral half inserted, and (c) two halves of the cerclage passer engaged and clamped.
Results
Over this 5-year period, we operated on 1783 proximal femur shaft fractures and 1401 distal femur fractures (inclusive of periprosthetic fractures). Among the proximal femur shaft fractures, 203 required open reduction, of which 126 had cerclage wiring done using the cerclage passer (Synthes). Of the 1401 distal femur shaft fractures, however, only 28 patients had cerclage wiring. Of these patients, two with proximal femur shaft and two with distal femur shaft fractures sustained vascular injuries due to the cerclage passer (Synthes). Incidence was calculated at 1.59 (2/126) vascular injuries per 100 patients with proximal femur shaft fractures using cerclage wires and 7.14 (2/28) per 100 patients with distal femur shaft fractures that had cerclage wiring done.
Distal femur shaft fracture
Patient 1
A 75-year-old lady presented to us following a slip and fall in the bathroom with a right-sided comminuted long spiral distal femur fracture (33-A1.2; Figure 2). Following spinal anesthesia, she was positioned supine on the operating table with a square pillow under her right leg. We do not use tourniquet for distal femoral fracture fixation. Via a lateral approach (15-cm incision), the fracture site was exposed, reduced, and held with reduction clamps. To maintain reduction, cerclage wiring was planned approximately 13 cm proximal to the adductor tubercle. The cerclage passer (Synthes) was used as per the standard procedure. As soon as the two halves were fitted together and clamped shut, torrential bleeding was noted from the medial aspect of the fracture. The instrument was removed, manual compression applied, and vascular surgeon was called. Through a separate medial approach, a double puncture was identified in the SFA. With the fracture alignment being held with reduction clamps, the injured segment was resected and end-to-end anastomosis was done. Following this, the fracture was fixed using a distal femur locking compression plate and the wounds were closed over suction drains (Figure 2).

Elderly patient with distal femur shaft fracture attempted for cerclage wire fixation using the cerclage passer (Synthes®) and had a superficial femoral artery puncture treated by end-to-end anastomosis. Note: Ligaclips (arrow) in the location of vessel repair. Circle denotes the location of vascular injury in the magnified image.
Patient 2
A 67-year-old male with a right-sided comminuted distal femur fracture (33-A1.2). Bleeding was noted in this patient also when the two halves were clamped shut (about 14 cm proximal to the adductor tubercle) and in a similar sequence, the injured vessel was found to be the SFA (double puncture) requiring resection of the injured segment and end-to-end anastomosis.
Proximal femur shaft fractures
Patient 3
A 22-year-old male presented to us following a road traffic accident with a comminuted long spiral left-sided proximal femur shaft fracture (32-C1; Figure 3). Closed reduction was attempted on the fracture table with boot traction by traction, adduction (20°), and internal rotation (10°) of the extremity, which was, however, unsatisfactory. So the fracture site was opened via a lateral approach (5-cm incision) and reduction was achieved using reduction clamps. Cerclage wiring was attempted using the standard technique at a level just distal to the lesser trochanter. The two halves were clamped, trocars were removed, and the wire was passed. As soon as the two halves were disengaged, a spurt of bleeding was noted from the medial side of the fracture site. Vascular surgeon was called and in the meantime, the SS wire was removed, manual compression was applied to the bleeding, and fracture was fixed with a proximal femoral nail with two cephalic screws and two distal screws. The traction was then released and the limb was abducted. Through a separate anteromedial incision in the proximal thigh, the bleeding was localized to a rent in the DFA and was controlled by ligation of the vessel using Ligaclips (Figure 3). Wounds were closed over drain after ensuring hemostasis.

Proximal femur shaft fracture treated with a reconstruction nail had a deep femoral artery injury while attempt was made for passing cerclage wire with the cerclage passer (Synthes®). Note: Ligaclips (arrow) at the site where vessel was ligated. Circle denotes the location of vascular injury in the magnified image.
Patient 4
A 44–year-old male who came to us with a long spiral comminuted subtrochanteric fracture (32-B1.1) experienced a similar series of events. Following open reduction of the fracture and cerclage passer application just distal to the lesser trochanter, undue bleeding was encountered as soon as the two halves were clamped together. Vascular exploration following fracture fixation with a proximal femoral nail revealed a rent in the perforator branch of the DFA, which was managed by ligating the perforator.
All patients presented with normal pre-op vascularity. All had a sudden fall in blood pressure when vascular injury occurred, necessitating urgent vascular intervention, as a result of which intraoperative images were not possible.
Postoperatively, all patients were observed for a day in intensive care. No re-exploration was needed since there was no leak, blow out, or failure of the anastomosis. There were no post-op complications and all fractures healed uneventfully. All four patients had satisfactory outcomes at the end of 1-year follow-up.
Discussion
Femoral shaft blood supply is derived from three parallel arterial pathways, including the SFA, the DFA or profunda femoris artery, and the collateral pathway via the perforators 2,12 (Figure 4). An additional path is also available by way of the descending branch of the lateral femoral circumflex artery. 2 The DFA is composed of three separately numbered perforator branches and a terminal branch which is often termed as the fourth perforator. The perforating arteries (PFAs) sequentially anastomose with adjacent perforators along the linea aspera, posterior to the femur. 2 They provide the primary arterial supply to numerous muscles of the thigh, particularly in the medial and posterior compartments, and a large nutrient artery to the femoral shaft (typically from the second perforator). 2
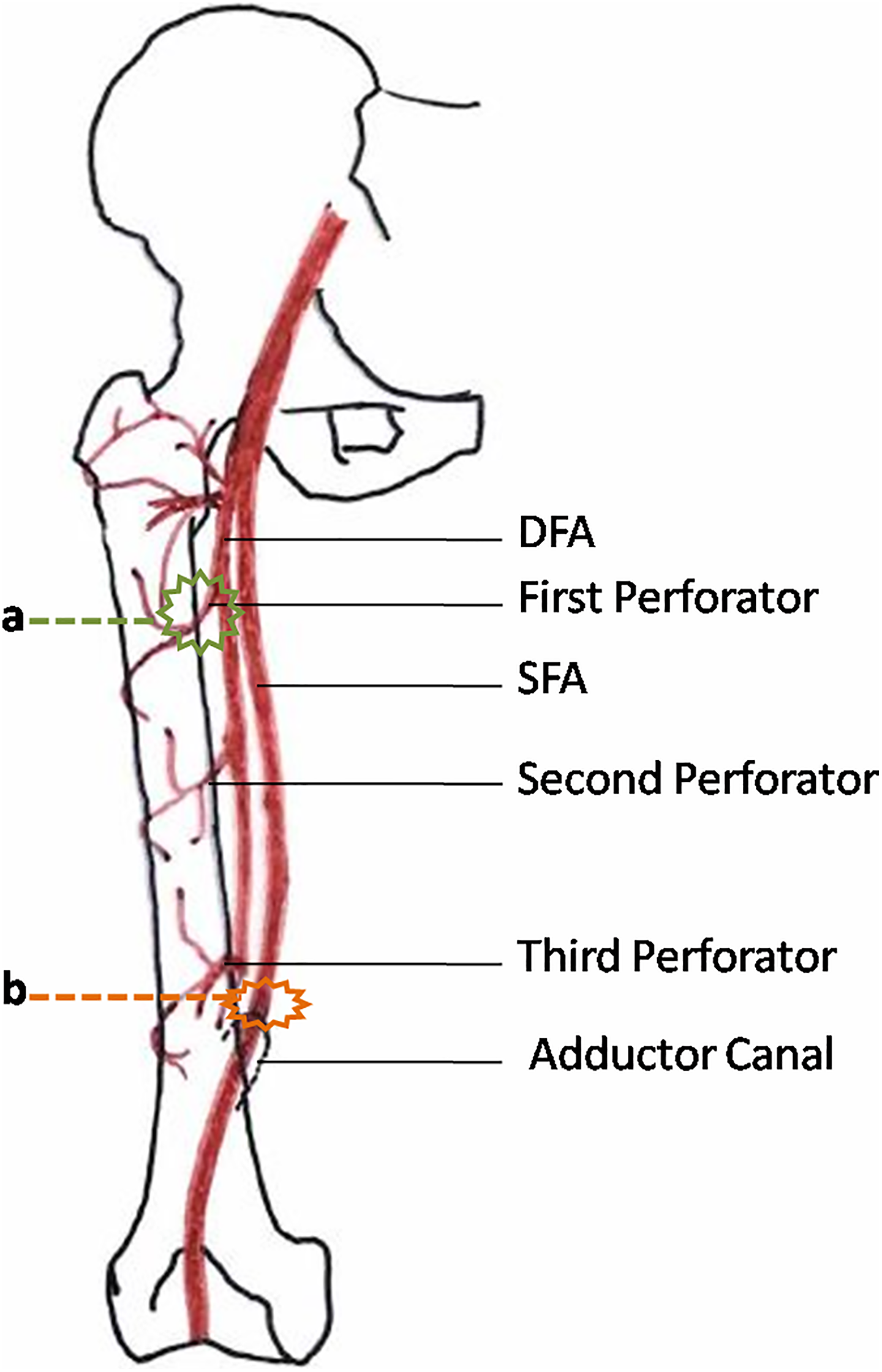
Vascular anatomy and sites of injury. (a) Green wireframe shows the site injury of DFA and PFA by cerclage passer (Synthes®) in the proximal femur shaft. (b) Orange wireframe shows the injury of SFA by cerclage passer (Synthes) in the distal femur shaft.
The etiology of vascular injuries in femoral fractures may be roughly divided into iatrogenic and non-iatrogenic. The latter includes sharp bone fragments, scar tissue, and direct trauma (open injuries), whereas the former consists of insertion plate screws or locking bolts of intramedullary nails, and also malpositioned retractors, plunging drill bits, and the movements of fragments during reduction procedures. 13,14 Manner et al. emphasized that traction on a fracture table tightens the femoral muscles and additionally reduces the local mobility of the DFA. 15 Yang et al. demonstrated the influence of the extremity’s position on the fracture table on the distances between femoral vessels and the medial femoral cortex. The mean distance between the SFA and the bone diminished significantly when the leg was brought into adduction of 20° on a traction table (reduction position) from 20.2 mm to 11.8 mm and even to 9.4 mm with an additional internal rotation of 20°, thus predisposing it to injury. 16 The DFA is more vulnerable in the proximal femur owing to its proximity to the femoral diaphysis and reduction in mobility due to the fixing perforators as they pierce the intermuscular septum. 14 The SFA on the other hand is further away from the bone in the proximal femur and it is more mobile. The SFA moves closer to the femur in the distal shaft and has a fixation point in the adductor canal limiting its mobility. 2,3 In our cases, all injuries occurred during cerclage passer application, two involving the DFA system in comminuted long spiral proximal femur shaft fractures (both positioned in boot traction with adduction of 20° and internal rotation of 10°) and two involving the SFA in comminuted long spiral distal femur shaft fractures.
Mehta and Finn 8 and Aleto et al. 7 reported occlusion of the SFA by cerclage during revision total hip arthroplasty at the mid-shaft and middle-distal shaft junction, respectively. Both cases were detected postoperatively due to the presence of pale, cool extremity and absence of distal pulses. Both authors had used standard wire passer, and intraoperatively wire application was uneventful. Mehta and Finn’s 8 patient recovered with the release of the fascia tethering, the SFA, and ligation of the femoral vein, while Aleto et al.’s 7 patient required a thrombectomy, endovascular stent, and removal of the offending wire. All of our patients, however, presented with torrential bleeding intraoperatively, either when the two halves of the cerclage passer were clamped together (patients 1, 2, and 4) or when the two halves were disengaged (patient 3). Won et al. reported a completely missed occlusion of the SFA by cerclage wire at the level of the mid-shaft of the femur following nailing of the long spiral fracture of the femur, which ultimately led to a below knee amputation despite removal of the offending wire and reconstruction of the injured vessel. 6
Management depends on the type and location of vascular injuries. They may be evident immediately in the form of increased bleeding following vessel laceration or puncture or may present later as persistent or recurrent swelling and pain, with a gradual fall in hemoglobin pointing toward a pseudoaneurysm. 5 Management options range from conservative treatment to percutaneous endovascular procedures such as coil embolization and stenting to ligation, repair and excision, and anastomosis. 14 The DFA and perforators may be ligated due to anastomosis in the posterior part of the proximal femur providing collateral circulation from the medial femoral circumflex artery, inferior gluteal artery, and first perforator. 2 Patients 1 and 2 with double puncture of the SFA were managed with resection and end-to-end anastomosis, while the remaining were treated with ligation of the DFA and PFA.
The incidence of vascular injuries in femur fractures is reported to be approximately 2%. 6,17 With the increasing rate of operative interventions for the femur, hip, and knee, this incidence is likely to escalate. We report an incidence of 1.59% for cerclage-induced vascular injuries in proximal femur shaft fractures. However, the same for distal femur shaft fractures was an alarming 7.14% in our center. We feel that this large incidence may be attributed in part to the difficulty we experienced in maintaining the cerclage passer (Synthes) close to the bony surface all the way around the femur, because the inner curvature of this instrument did not match the axial circumference of the femur in our patients and this was more pronounced in the distal femur. Mehta and Finn showed that the tethering of the fascia surrounding the femoral artery can also occlude femoral blood flow without direct injury to the femoral artery itself. 8 Narulla and Kanawati illustrated a danger zone for the SFA extending from 239.6 ± 39.8 mm to 172.5 ± 40.9 mm proximal to the adductor tubercle and a safe zone 172.5 mm 40.9 mm proximal to the adductor tubercle. 3
Though both our passes in the distal femur shaft fell into the outer range of the danger zone, we recommend that the cerclage passer (Synthes) must be applied with extreme precautionary measures to avoid iatrogenic vascular injuries in any femur fracture (particularly distal femur shaft). In a recent CT angiography study by Apivatthakakul et al., the authors recommended meticulous use of the cerclage passer (Synthes®), keeping its tip close to the posteromedial cortex when used between the mid-shaft and the distal three-fourth of the femur shaft and keeping the tip close to the posterior cortex when used below the distal one-fourth of the femur shaft to avoid injury to the SFA. 10 It is imperative to stay in close contact with the bone surface while passing the instrument and also to maintain the position of the dorsal half of the cerclage passer (Synthes) against the bone while bringing and engaging the ventral half to it. 9 Other precautionary measures could include reducing the amount of traction 15 as well as the amount of adduction and internal rotation 16 and also restricting the number of passes 4 in order to safeguard the vasculature during this procedure. We recommend strict vigilance for any undue bleeding particularly when the two halves of the cerclage passer (Synthes) are clamped together or when the two halves are disengaged and being removed. We would also recommend the use of alternate reduction methods in long spiral distal femoral fractures.
Conclusion
Correct surgical technique is essential while using the cerclage passer (Synthes), particularly around the proximal and distal femur shaft. Knowledge of the danger zones, fewer passes, limiting traction, and bringing the limb to neutral position during this procedure may reduce the risk of iatrogenic vessel injury. Strict vigilance and urgent vascular intervention are imperative to avoid life- and limb-threatening complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Ganga Orthopaedic Research and Education Foundation. The funding was to the institution and not directly paid to any author.