
Abstract
Introduction:
This report describes the first known sternoclavicular joint (SCJ) replacement with a custom-made prosthesis.
History:
A 42-year-old male who presented post left medial clavicular excision with significant pain and limited range of motion impeding his daily activities and ability to work. The patient subsequently underwent a left SCJ arthroplasty with a custom-made prosthesis. Postoperatively, the patient suffered an anterior dislocation of the prosthetic joint which was successfully rectified and stabilized with soft tissue reconstruction, creating a pseudo-capsule from adjacent tissues of the joint. Thereafter, the patient required a final procedure to remove prominent sutures.
Results:
Currently, the patient has regained full range of motion and is pain free during most activities and has now returned to work, with a plan to review his progress in 1 year. These initial promising results post SCJ replacement with the custom-made prosthesis could potentially lead SCJ reconstruction in an exciting new direction.
Discussion:
More research should be encouraged regarding this nascent operative option, in order to identify the indications, parameters, and effectiveness of SCJ arthroplasty.
Keywords
Introduction
The majority of sternoclavicular joint (SCJ) pathologies are managed conservatively owing to difficult access and poor/lack of studies regarding this topic. However, when the pain adversely affects a person’s ability to function, and conservative management is proving ineffective, then surgery becomes an option to consider. 1 Up till now, efforts for SCJ reconstruction have provided mixed results. The SCJ is structurally classed as a saddle-type synovial joint, known as a double plane joint, and functionally classed as a diarthrotic joint. 2 It is composed of the medial aspect of the clavicle which articulates with the superior and lateral border of the manubrium (clavicular notch of manubrium sterni) and the cartilage of the first rib.
The SCJ is the only attachment of the upper limb to the axial skeleton. 3 There are several ligaments and structures which stabilize it, including the anterior sternoclavicular ligament anteriorly, the costoclavicular ligament laterally and inferiorly, the interclavicular ligament superiorly and medially, the posterior sternoclavicular ligament posteriorly, as well as the articular capsule and disk within the joint itself. 4
The articular surface of the clavicle has a greater area and thicker layer of cartilage than that of the clavicular notch on which it articulates. 3 The SCJ moves in three planes: predominantly the anteroposterior and vertical planes, and to a lesser extent, there is rotational movement. This allows for elevation, depression, and circumduction of the SCJ. There is no direct action of muscles on the joint; however, almost all shoulder (girdle and/or scapula) movement will indirectly shift the position of the SCJ. 5
A double-hinged articular disk between the clavicle and the manubrium facilitates various movements segmentally. Elevation and depression of the scapula is assisted by articulation between the clavicle and the disk, while protraction and retraction of the scapula is enabled by motion between the clavicular notch on the sternum and the disk. 5
Common complications of the SCJ include joint dislocation which could potentially compromise mediastinal structures if the dislocation were posterior. SCJ dislocations account for 3% of all shoulder girdle injuries, 95% of which are unilateral and the majority are anterior owing to the weaker anterior sternoclavicular ligament. 6 There can be SCJ degeneration and less commonly septic arthritis of the SCJ. 7
While there is some literature discussing reparation of dislocations and joint resection for SCJ pathology, there is no literature describing the use of an SCJ prosthesis. SCJ repairs to date have included Kirschner wire fixation, screws, and plating; however, the majority of all hardware required removal after 3 months. Furthermore, two studies reported Kirschner wires were associated with intracardiac migration resulting in lethal complications. 8,9 Screws were associated with less hardware migration, though 50% required removal. 10,11 One study regarding plate fixation, of 10 SCJ dislocations, had good outcomes, though was described as bulky. 12 A case of a policewoman in 2010 had an anterior dislocation of her SCJ and also had a good outcome post Open Reduction Internal Fixation (ORIF), where fixation involved two bony anchors with two Hi-Fi strings. 13
Variations of soft tissue reconstruction of the joint have been described since 1951 by Burrows, who carried out a subclavius tenodesis with a capsulorrhaphy 14 and the sternocleidomastoid (SCM) tissue, and have been found effective to a certain extent. 8,15,16 Attempts to attach the medial clavicle to the first rib 14,15,17,18 and wrapping the SCM around the first rib 19 provided moderate success. Armstrong AL and Dias JJ, 2008, freed the SCM proximally, leaving it attached at the sternum, while using the free SCM to recreate an anterior capsule, however this resulted in varying degrees of subluxations. 20
Suture fixation of the first rib to the sternum also resulted in subluxation complications. 21 Manubrial suture anchors showed promise; however, one of five patients was left permanently disabled and unable to work. 15 Although Deren et al. noted the effectiveness of suture anchors with regards to stability whilst other studies suggested potential complications of bone erosion and impaired biomechanics as compared with less flexible fixations. 7
Figure-of-eight soft tissue graft reconstruction, which uses a free semitendinosus graft, proved to be more stable and less restrictive; however, it was also prone to failure usually by clavicular or sternal fracture. Some studies also found some patients remained with limited range of motion and instability. 22 –25
Generally, there is little literature on SCJ fixation and the results are conflicting with low numbers of cases, making it difficult to draw conclusions as to what surgical treatments are most appropriate for SCJ pathologies.
Regardless of fixation technique, soft tissue structures have been reported as important for joint stabilization. 26 Rockwood et al. (1997) investigated the effectiveness of resection arthroplasty of SCJ to treat pain and concluded that keeping the costoclavicular ligament intact was key to a successful outcome. 16 Extrapolating from this article, one can surmise that the congruity of SCJ ligaments is essential for a stable and functional joint.
History
A 42-year-old male presented to the orthopedic upper limb clinic September 13, 2011 with left SCJ pain post partial excision of the medial aspect of the left SCJ in September 2010. Despite ongoing physiotherapy and analgesia, the patient reported significant left SCJ pain with associated decreased range of motion, impeding his daily activities and work. On examination, the patient had full range of movement (ROM), though, due to the previous excision of the medial aspect of the clavicle, the joint was evidently unstable (Figure 1).
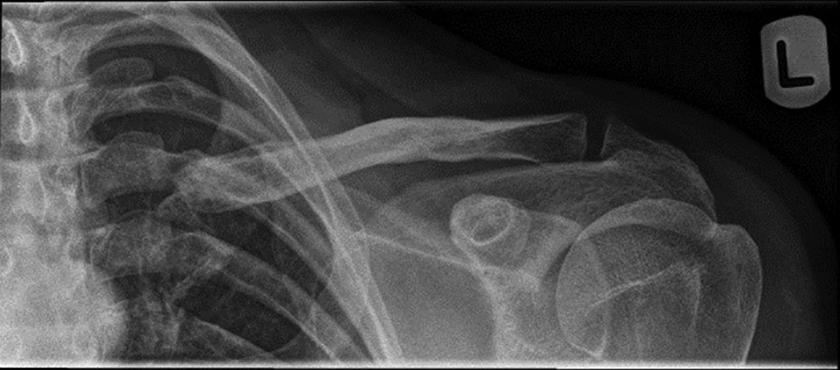
This figure is a radiograph of the left sternoclavicular joint.
During the following 2 years, the patient was reviewed four times while awaiting the custom prosthesis. At each appointment, the patient reported substantial pain and limited left shoulder ROM, causing him to be seen earlier than his scheduled appointments on two occasions. On examination, the patient remained clinically stable and his ROM remained unchanged throughout the preoperative phase. Two pain assessments (DASH and Oxford scores) were carried out. The patient continued with physiotherapy and analgesia until the scheduled operative date.
Arthroplasty operation
On July 15, 2013, the patient underwent a left SCJ arthroplasty with a custom-made prosthesis. The patient was in the beach chair position and was given a prophylactic dose of cefuroxime 1.5 g on induction. The incision was made over the initial transverse incision just anterior to the left SCJ joint and extended at both ends, after which the surgeon proceeded to incise the platysma while protecting the sternal part of the SCM muscle. On observation, there was a gap of 2 cm between the head of the clavicle and the left proximal end of the sternum. The procedure entailed preparation of the left sternal proximal edge, followed by drilling and fitting of the custom-made prosthesis. Drilling of the medial end of the clavicle was done through a custom-made guide and the stemmed clavicular prosthesis was fixed with cement, while the sternal component was prepared with the custom-made guide and then press fitted without cement. Good congruity was observed. The joint immobilized with a sling in theater. (Figures 2 to 10).

This figure shows the prosthetic components: different sizes to choose from for the medial clavicular replacement, a short stem which gets screwed to the clavicular component, and the PEEK (Polyether ether ketone, a thermoplastic polymer) sternal component.

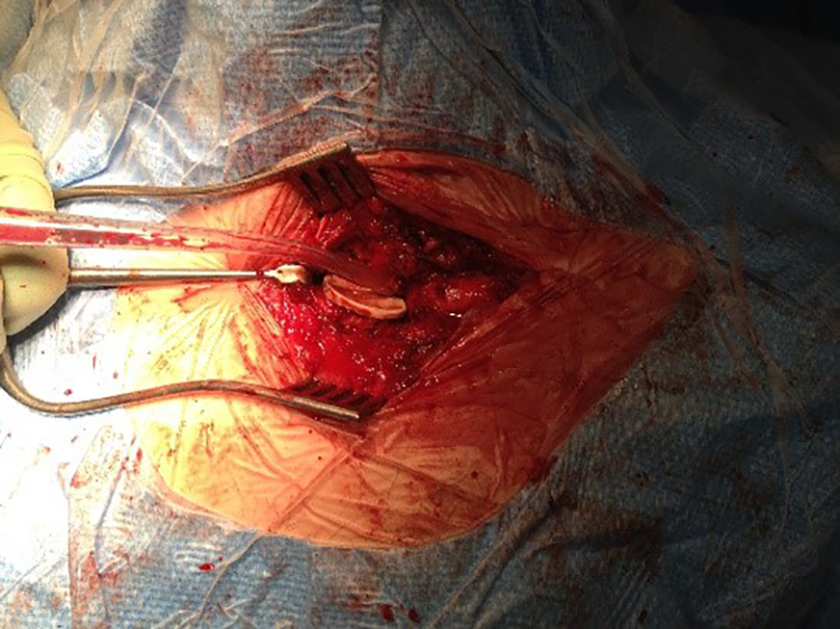
This figure shows the sternoclavicular joint exposed. Note that the medial clavicle was previously excised hence it is short, not in contact with the sternum and its canal is almost obliterated.

This figure shows the custom-made jig used to prepare the sternum side of the replacement.

This figure shows the sternum side being drilled in preparation for the insertion of the sternal polyethylene component.
This figure shows the sternal component inserted cementless.
This figure shows the clavicular side custom-made jig.

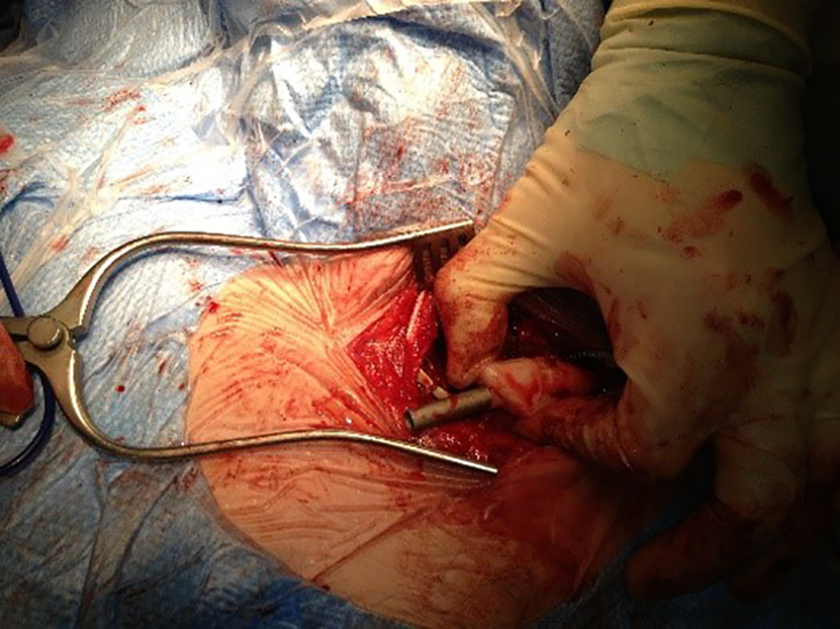
This figure shows the clavicular medulla being drilled in preparation for the insertion of its corresponding stemmed component.

This figure shows the insertion of the clavicular component.

This figure shows the SCJ components in place: an uncemented sternal component with a cemented clavicular component. SCJ: sternoclavicular joint.
Postoperatively, analgesia was delivered as appropriate. Venous thromboembolism (VTE) prophylaxis included one dose of Fragmin 2500 units 6 h postoperatively with early mobilization of the patient out of bed. Postoperative day 1, the patient's Left Upper Limb (LUL) was abducted by 30 degrees and X-rayed (Figure 11). The patient was discharged with instructions to wear the sling for 8 weeks and to not weight lift for 12 weeks.
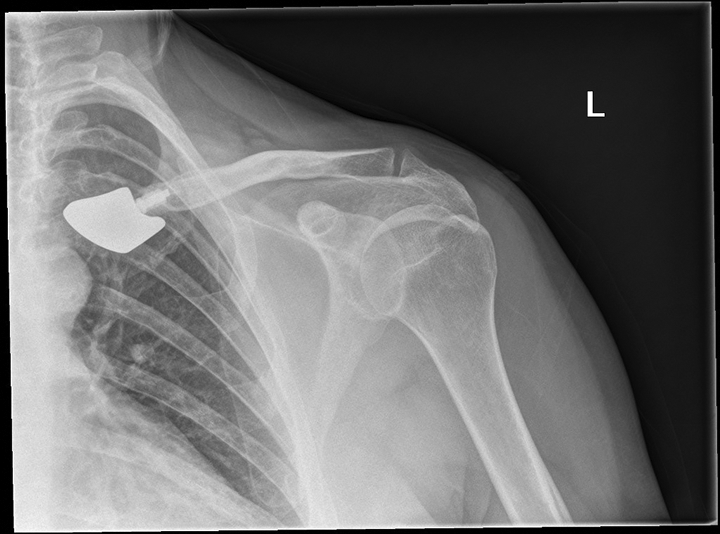
This is a figure of a postoperative radiograph of the left sternoclavicular joint with arthroplasty.
Anterior dislocation complication
On July 30, 2013, the patient was reviewed early secondary to severe left shoulder pain. On examination, it appeared that the shoulder girdle was sinking backward, therefore the abduction splint was repositioned to bring the left arm further forward. The wound was observed to have healed well; however, there was still some residual swelling around the SCJ. Of note, the patient reported that he had an increased ROM of the neck and that his previous headaches had significantly improved.
However, on September 24, 2013, again the patient presented early due to left shoulder and SCJ pain, which he described as sharp in nature and associated with cramping and noise on left shoulder movement. On examination, the patient had limited ROM secondary to pain, tenderness on palpation on the lateral aspect of the prosthesis stem inside the clavicle, and subjective displacement of the joint. Six weeks later, a computer tomography (CT) confirmed the patient’s impression, showing an anterior and inferior dislocation of the medial end of the clavicle. The patient was then planned for a left SCJ prosthesis revision for stabilization and implant retention.
Stabilization operation
On October 13, 2014, the patient was placed in beach chair position, under general anesthesia and with prophylactic antibiotics on induction.
The procedure began with an incision of the previous scar. Once the SCJ was exposed, the clavicular and sternal components were both found to be solidly fixed to their respective places. Subsequently, these were not disturbed and were retained, therefore only a soft tissue reconstruction was undertaken in order to stabilize the SCJ. Adjacent tissues were enveloped around the joint and then sutured over it, with anterior buttressing of the tissues using fiber wire stitches. After tissue reconstruction, the joint was stable.
Postoperatively, the patient was placed in an abduction splint for 6 weeks, X-ray (XR) of the left shoulder post-op day 1 was reviewed, no physiotherapy was indicated, and VTE prophylaxis involved early mobilization of the patient out of bed. A follow-up in 2 weeks on discharge was organized.
Minor complications
On November 4, 2014, the patient continued to report less pain and was satisfied with the outcome of the reconstruction. The wound appeared to have healed well other than a prominent absorbable suture which was removed directly.
Postoperatively, the patient reported significantly less pain and was keen to start work again, for which he was given permission but instructed to avoid heavy lifting and to continue wearing the abduction splint for another 2 weeks, and was encouraged to mobilize his elbow three to four times a day. A follow-up appointment with CT on arrival was made for in a month.
Three months later, the patient reported increased ROM and residual pain in the order of 5–6/10. On examination, there was tenderness over the surgical scar. The left shoulder ROM included forward flexion of 120°, abduction of 110°, internal rotation up to T12, and external rotation up to 80°. A local steroid injection was administered for localized scar pain.
Finally, on May 19, 2015, the patient’s pain was determined to be due to prominent bulky internal stitches. The patient was therefore listed for theater for removal of internal stitches, which were removed on September 5, 2015.
Progress
Six weeks postoperatively, the patient appeared to be doing well; however, in the last few weeks, the shoulder had become more painful after excessive swimming with front crawl. The patient was pain free with all other activities. Therefore, the patient was advised to stop doing front crawl. The patient will be reviewed in a year post this last appointment.
Discussion
The first reported use of a custom-made SCJ prosthesis is a unique new treatment direction and a new avenue of therapy for patients with refractory SCJ pathologies not responding to conservative management. The case of our patient, who underwent medial clavicular resection, had significant pain, headaches, and limited range of motion affecting his daily function and was therefore determined to require surgical intervention in an attempt to restore the function of the SCJ and alleviate his pain.
The most common complications of both tissue and bone SCJ surgeries occurred almost immediately postoperatively, namely dislocation of the SCJ and bulky suture discomfort. These were successfully rectified with a soft tissue graft strengthening the prosthetic joint, thereby facilitating its function, followed by removal of internal sutures.
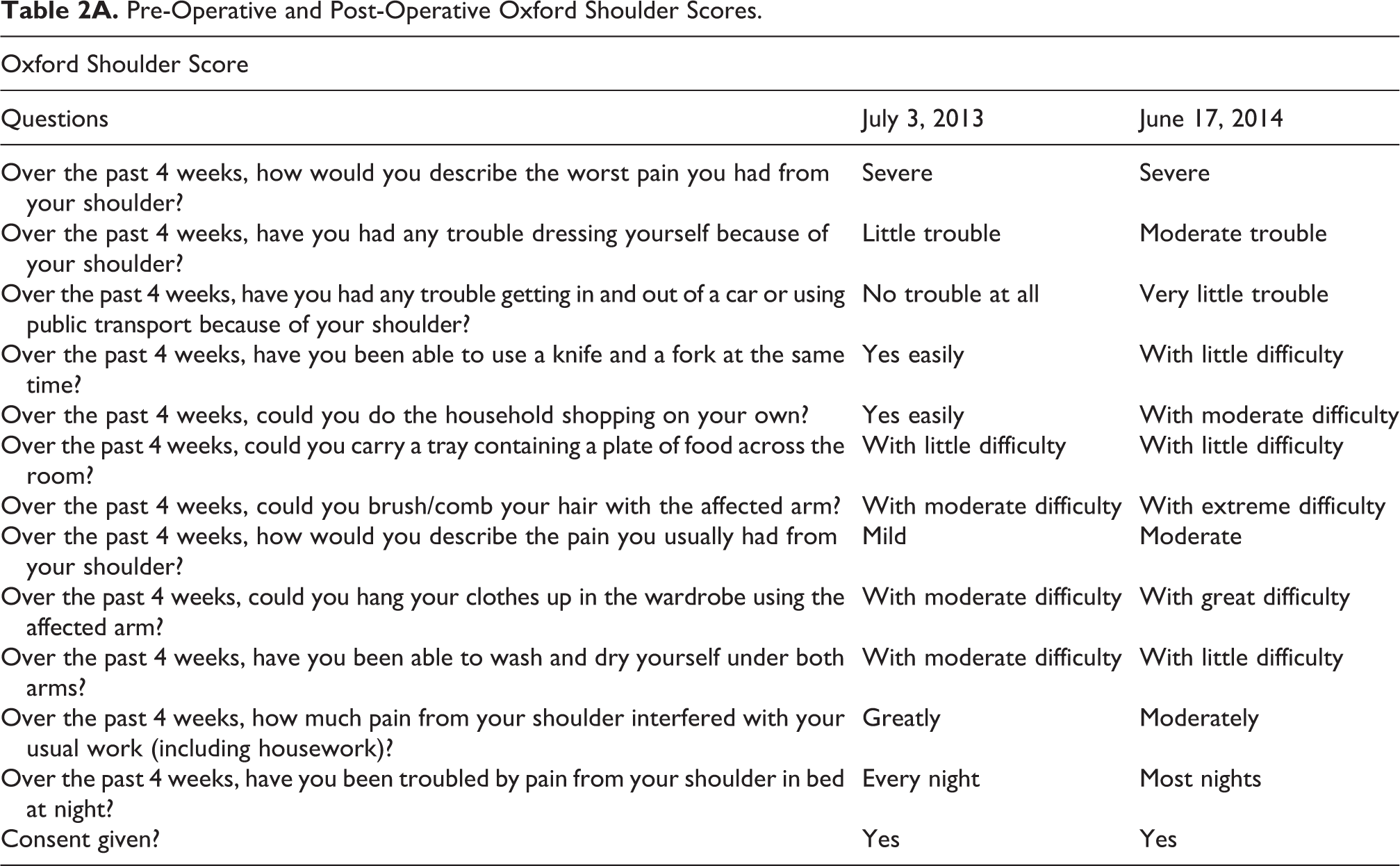
Preoperative and postoperative DASH scores were 50 and 52.5, and Oxford scores were 28 and 23 (see Tables 1A and 2A of Appendixes 1 and 2—DASH and Oxford scores). This demonstrates that preoperative pain was significant and that postoperative pain prior to stabilization of the joint and suture removal was similar. However, after both revisions, the patient is now currently pain free and has been able to resume most activities, including his work.
For now, SCJ prosthetic arthroplasty shows a potential ability to effectively restore joint function and offer pain relief. More research will be required to explore the full potential of this intervention. Further cases would help define eligibility criteria regarding which patients would most benefit from such an intervention, refine parameters regarding prosthesis and operative technique, and finally assist in determining the effectiveness of a SCJ prosthetic arthroplasty intervention.
Conclusion
SCJ fixation is an uncommon intervention with mixed outcomes and variable degrees of complications ranging from bulkiness to patient demise. With a custom-made prosthesis, this patient was able to return to work after several years of unemployment, resume the majority of his daily activities painlessly, and regain most of his left shoulder function with increased ROM in his neck. This case report demonstrates the potential utility and effectiveness of such an intervention and encourages further research to be undertaken in order to determine its effectiveness and refine the technique while limiting risks of complications. Prosthetic arthroplasty therefore warrants further investigation as a promising surgical intervention for refractory SCJ pain with instability.
Footnotes
Appendix 1
Pre-Operative and Post-Operative DASH Scores.

| DASH Score | ||
|---|---|---|
| Questions | July 3, 2013 preoperatively | June 17, 2014 postoperatively |
| How difficult is it to open a tight/new jar? | Mild difficulty | Mild difficulty |
| How difficult is it to do heavy household chores (wash floors)? | Severe difficulty | Moderate difficulty |
| How difficult is it to wash your back? | Moderate difficulty | Moderate difficulty |
| How difficult is it to use a knife to cut food? | Moderate difficulty | No difficulty |
| How difficult is it to do recreational activities? | Severe difficulty | Severe difficulty |
| During the past week (as a result of your arm, shoulder, or hand problem), interfered with normal social activities | Quite a bit | Extremely |
| During the past week (as a result of your arm, shoulder, or hand problem), limited your work or other regular daily activities | Very limited | Very limited |
| During the past week (as a result of your arm, shoulder, or hand problem), rate the severity of pain in your arm, shoulder, or hand | Moderate | Severe |
| During the past week (as a result of your arm, shoulder, or hand problem), rate the severity of tingling pins and needles | None | Mild |
| During the past week (as a result of your arm, shoulder, or hand problem), difficulty sleeping because of pain | Moderate difficulty | Moderate difficulty |
| Consent given? | Yes | Yes |
Appendix 2
Pre-Operative and Post-Operative Oxford Shoulder Scores.
| Oxford Shoulder Score | ||
|---|---|---|
| Questions | July 3, 2013 | June 17, 2014 |
| Over the past 4 weeks, how would you describe the worst pain you had from your shoulder? | Severe | Severe |
| Over the past 4 weeks, have you had any trouble dressing yourself because of your shoulder? | Little trouble | Moderate trouble |
| Over the past 4 weeks, have you had any trouble getting in and out of a car or using public transport because of your shoulder? | No trouble at all | Very little trouble |
| Over the past 4 weeks, have you been able to use a knife and a fork at the same time? | Yes easily | With little difficulty |
| Over the past 4 weeks, could you do the household shopping on your own? | Yes easily | With moderate difficulty |
| Over the past 4 weeks, could you carry a tray containing a plate of food across the room? | With little difficulty | With little difficulty |
| Over the past 4 weeks, could you brush/comb your hair with the affected arm? | With moderate difficulty | With extreme difficulty |
| Over the past 4 weeks, how would you describe the pain you usually had from your shoulder? | Mild | Moderate |
| Over the past 4 weeks, could you hang your clothes up in the wardrobe using the affected arm? | With moderate difficulty | With great difficulty |
| Over the past 4 weeks, have you been able to wash and dry yourself under both arms? | With moderate difficulty | With little difficulty |
| Over the past 4 weeks, how much pain from your shoulder interfered with your usual work (including housework)? | Greatly | Moderately |
| Over the past 4 weeks, have you been troubled by pain from your shoulder in bed at night? | Every night | Most nights |
| Consent given? | Yes | Yes |
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.