
Abstract
Purpose:
This study assessed the levels of soluble tumor necrosis factor–like weak inducer of apoptosis (TWEAK) and matrix metalloproteinase 1 (MMP-1) in the synovial fluid from osteoarthritic knees to determine their role as well as the relationship between these levels and the severity of osteoarthritis (OA).
Methods:
Synovial fluid was obtained from 44 knees of 40 patients. The Kellgren–Lawrence (KL) grade was measured using radiograph. The concentration of TWEAK and MMP-1 in the synovial fluid was assessed by enzyme-linked immunosorbent assay. The underlying inflammatory factors (erythrocyte sedimentation rate and C-reactive protein) were also measured. We analyzed the correlation between the factors measured. In addition, the samples were subdivided into three groups according to OA severity using the KL grade, and the differences in TWEAK and MMP-1 levels between groups were analyzed.
Results:
The TWEAK and MMP-1 levels in the synovial fluid showed a positive correlation with each other. The TWEAK and MMP-1 levels were compared between the three groups according to the KL grade, and the levels showed a significant difference. A post hoc test demonstrated that the group with advanced OA showed a lower concentration of both factors when compared to groups with early OA.
Conclusion:
The concentration of TWEAK and MMP-1 in the synovial fluid were relatively high in the early stage of OA, and the levels decreased as the OA progressed.
Keywords
Introduction
Osteoarthritis (OA) is a common disease and is an important cause for physical impairment in older populations worldwide. 1 It mainly invades joints that bear appreciable weight such as knees, hands, feet, and vertebrae, or those that are excessively used, and causes pain, stiffness, and hypofunction. 2 OA is primarily caused by gradual loss of cartilage in joints and associated secondary changes. While OA is simply considered a part of the aging process, various inflammatory changes have been observed in cartilage with OA, and inflammatory reactions are increasingly thought to be involved in pathogenesis. 3 Moreover, as various substances that damage cartilage are found in joints with OA, researchers studied the correlation between these substances and the onset of disease and symptoms. 4,5
Although the etiology of cartilage damage in OA has not been clearly identified, it is believed that destruction of the extracellular matrix (ECM) by inflammatory cytokines secreted from cartilage cells causes joint inflammation, cartilage damage, and destruction of cartilage cells, contributing to OA. If the production of ECM including type 2 collagen, proteoglycan, and aggrecan decreases, and ECM decomposition is accelerated by matrix metalloproteinase (MMP) as a result of change in and destruction of cartilage cells, the basic structure of cartilage may be destroyed, thereby becoming unable to support the joint load. 6,7
Progression of OA is largely divided into three stages. In the first stage, the cartilage cells react to mechanical stimulation and the moisture content changes. The second stage occurs when the cartilage cells detect damage to or change in the tissues, increasing both anabolism and catabolism and inducing the action of various enzymes. In the third stage, the healing and reformation processes fail, causing progressive loss of cartilage, decreases in anabolism, and proliferation of cartilage cells take place. 8
In particular, the second stage involves various inflammatory mediators including cytokines; if their expression or action can be regulated during this stage, it can be assumed that the disease progression can be suppressed or reversed. 8 Substances identified as inducing catabolism include interleukin 1 (IL-1) and tumor necrosis factor alpha (TNF-α); these are assumed to induce increases in levels of various MMPs (MMP-1, -2, -3, -9, and -13), aggrecanase, IL-8, prostaglandin E2 (PGE2), and nitric oxide (NO), which contribute to cartilage destruction. 9 –12 In particular, MMPs, which include the enzymes collagenase, stromelysin, gelatinase, and others, are secreted by cartilage cells, synovial fluid, and synovial cells and play a role in the destruction of aggrecan and collagen in cartilage. 13
We attempted to identify the roles of various inflammatory mediators that may influence the pathogenesis of OA. Specifically, we tried to assess the relationship between TNF-like weak inducer of apoptosis (TWEAK) and the pathogenesis of OA. It was recently understood that TWEAK contributes to inflammatory arthritis, such as rheumatoid and psoriatic arthritis, thereby suggesting its potential usefulness as a monitor of disease activity or as a drug.
TWEAK, as a member of the TNF ligand superfamily, performs various biological functions through interaction with its receptor, fibroblast growth factor-inducible 14 (Fn14). 14 –16 According to recent research, TWEAK induces the formation of inflammatory cytokines and is involved in angiogenesis, apoptosis, and tissue recovery and regeneration. 17,18 It accelerates the generation of various cytokines such as MMP-1, IL-6, IL-8, and regulated on activation, normal T-cell expressed and secreted (RANTES) in synovial cells and fibroblasts and induces the generation of intercellular adhesion molecule 1 (ICAM-1) as well as E-selectin, IL-8, and monocyte chemoattractant protein 1 (MCP-1) by endothelial cells. 19
In particular, TWEAK accelerates the formation of MMPs in inflammatory joint disease and damages cartilage and bones via angiogenesis in synovial membranes and osteoclastogenesis. It is also known to be involved in suppressing the differentiation of precursors of osteoblastic and cartilage cells, thus interfering with intrinsic repair mechanisms. However, the role of TWEAK as a cause of OA has not yet been clarified, nor has there been any report regarding the expression of TWEAK within a joint according to the severity of OA.
Therefore, in this study, the concentration of TWEAK, and of MMP-1 induced by TWEAK, within synovial fluid in patients with OA were measured, in order to examine the expression of the two substances according to the severity of OA, and to investigate the relationship between TWEAK and OA.
Materials and methods
Materials and collection of samples
Synovial fluid was obtained from 44 knees of 40 patients at the time of knee arthroscopy or total knee replacement surgery. Patients with inflammatory arthritis, such as rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis, or underlying diseases including infectious diseases, malignant tumors, chronic renal failure, and liver failure, were excluded. Clinical data were collected before the surgery.
In order to examine the status of underlying inflammation before surgery, the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level were measured in each subject using the Westergren and standard nephelometric methods, respectively. Synovial fluid obtained during arthroscopy or total knee replacement was immediately centrifuged to remove cells and floating matter and isolate the supernatant, which was then frozen and stored at −70°C. This study was approved by our institutional review board, and all patients provided written informed consent.
Radiographic examination
Standard radiography was performed on knee joints with weight bearing, and osteoarthritic change in the knee joints was assessed using the Kellgren–Lawrence (KL) grade. The knee joints were classified into KL grade 0 (normal) to 4 (very severe): grade 0 = normal, grade 1 = possibility of osteophyte only, grade 2 = clear possibility of osteophyte and narrowing of articular cavity, grade 3 = medium-size osteophyte and/or clear narrowing of articular cavity, and grade 4 = large osteophyte, severe narrowing of articular cavity, and/or presence of bone sclerosis.
Measurement of concentration of TWEAK and MMP-1 in synovial fluid
TWEAK was measured by the DuoSet enzyme-linked immunosorbent assay (ELISA) development system (R&D Systems, Minneapolis, MN, USA) according to the manufacturer’s instructions. MMP-1 was measured in accordance with the method provided by the manufacturer, based on MMP-1 human ELISA kit (Abcam, Cambridge, UK).
Statistical analysis
For statistical analysis, SPSS (IBM SPSS Statistics version 21, Chicago, IL, USA) was used. First, Pearson’s coefficient was used to examine the correlation between expression of TWEAK and MMP-1, wherein MMP-1 was determined by TWEAK in OA patients. Second, Pearson’s coefficient was used to examine the correlations between ESR and CRP, which are indicators of underlying inflammation, and the main study factors (TWEAK and MMP-1). Third, one-way analysis of variance (ANOVA) was used to examine the mean difference of ESR, CRP, TWEAK, and MMP-1 in groups classified based on OA severity. A post hoc test was performed according to Scheffe’s method. Statistical significance was set as p < 0.05.
Results
Clinical characteristics
Of the 44 subjects, 14 (31.8%) were males and 30 (68.2%) were females, and the average age was 55.1 ± 19.7 years. The 44 knees were classified according to KL grade: 10 cases (22.7%) belonged to grade 0; 3 (6.8%) to grade 1; 8 (18.2%) to grade 2; 3 (6.8%) to grade 3; and 20 (45.6%) to grade 4. We reclassified knees into three groups according to OA severity: group A—mild OA (KL grade 0 or 1), group B—moderate OA (KL grade 2 or 3), and group C—severe OA (KL grade 4). The reclassification according to the KL grades resulted in group A with 13 cases (29.5%), group B with 11 cases (25.0%), and group C with 20 cases (45.5%).
Correlation between concentration of TWEAK and MMP-1 in synovial fluid
The average concentration of TWEAK and MMP-1 in synovial fluid were 438.6 ± 350.9 pg/mL and 1017.4 ± 443.6 pg/mL, respectively, and showed a positive correlation, with r = 0.460; p < 0.05 (Figure 1). In other words, increase in TWEAK was linked to MMP-1 increase. Scatterplot (TWEAK × MMP-1). TWEAK: tumor necrosis factor-like weak inducer of apoptosis; MMP-1: matrix metalloproteinase-1.
Correlation between indicators of underlying inflammation (ESR and CRP) and the main study factors (TWEAK and MMP-1)
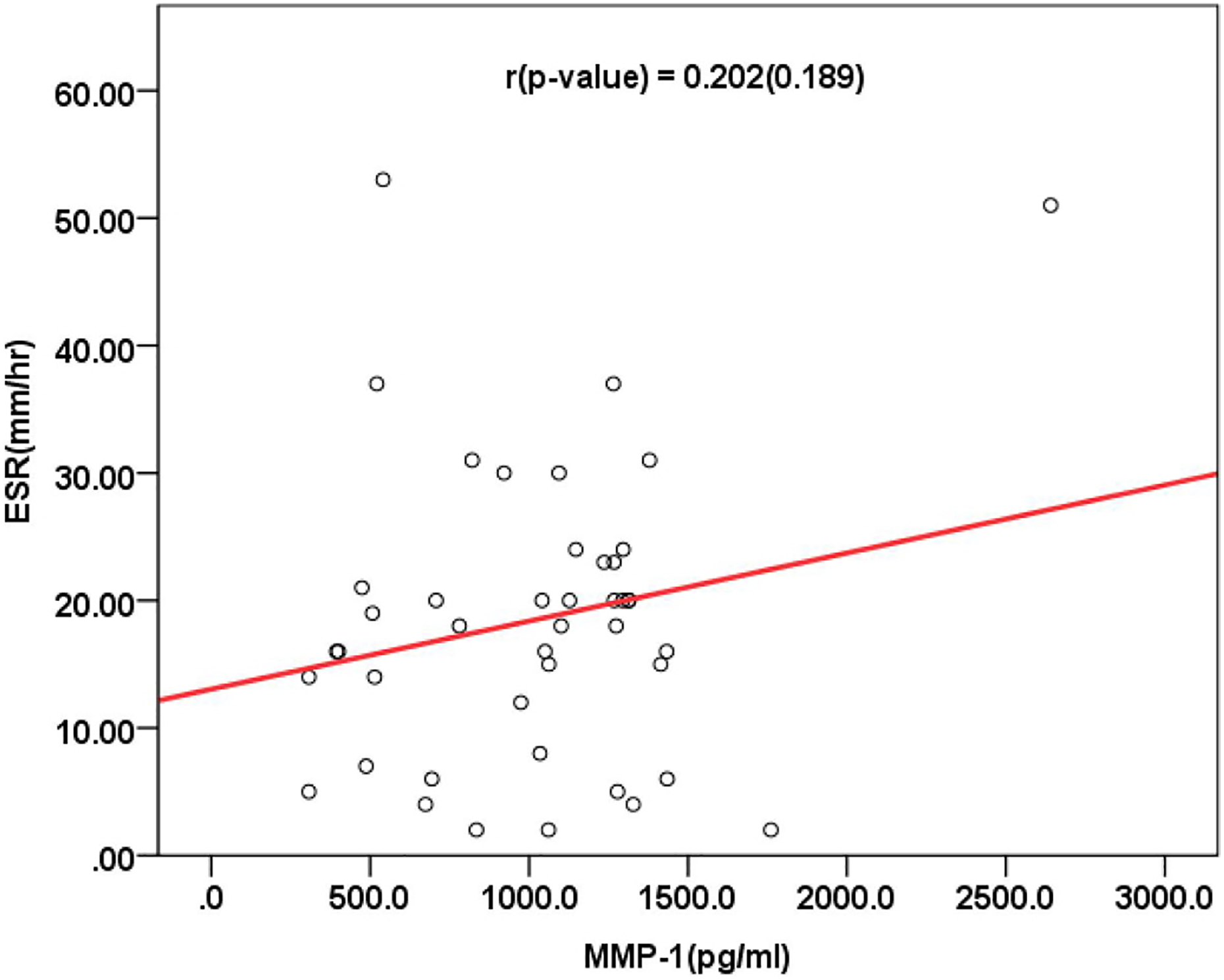
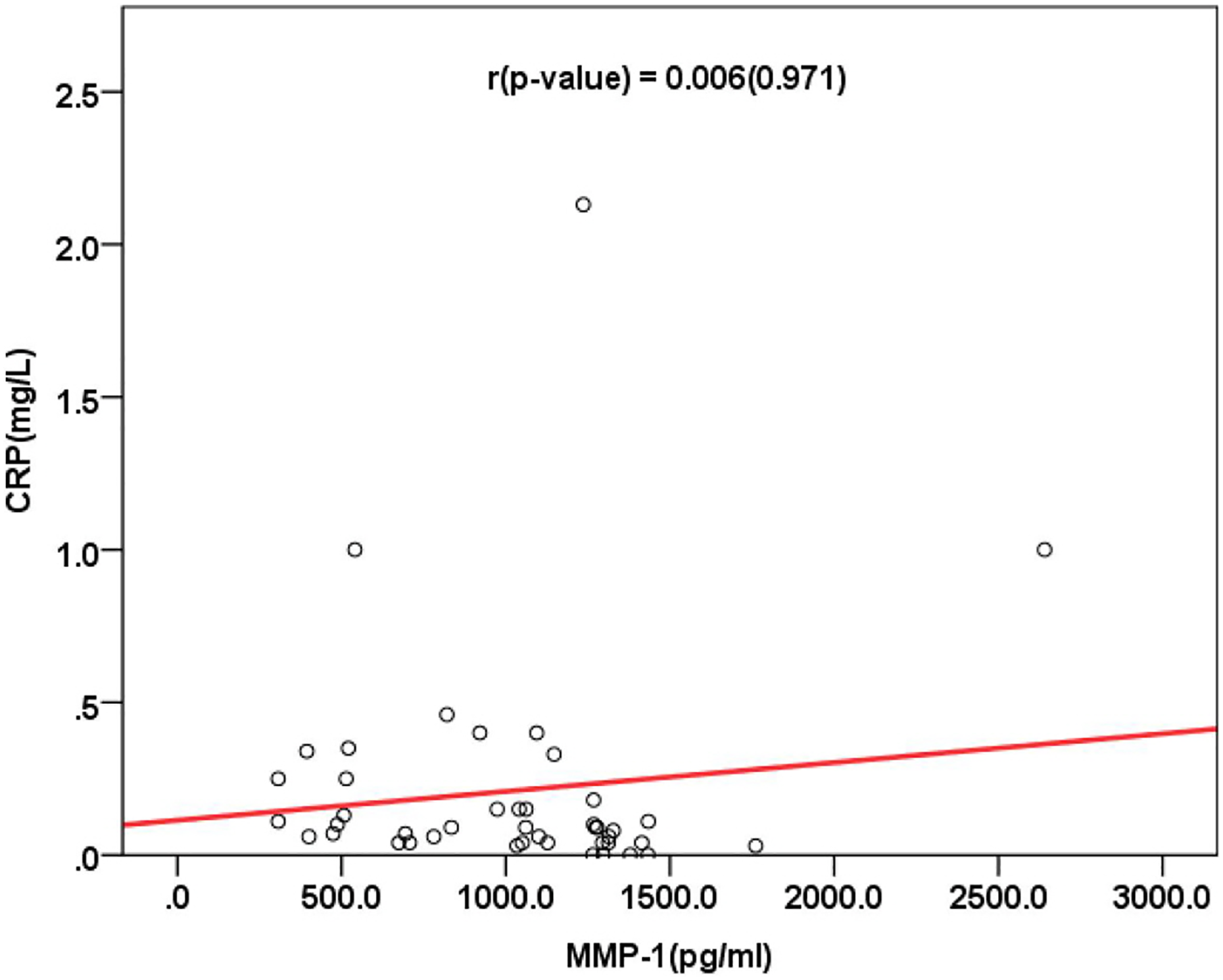
The coefficients of correlation between TWEAK and ESR (r = −0.167; p > 0.05), and between TWEAK and CRP (r = 0.006; p > 0.05) showed no statistical significance. In addition, there was no statistically significant correlation between ESR and CRP and MMP-1, with r = 0.202; p > 0.05, and r = 0.114; p > 0.05 (Figures 2
–5). Scatterplot (TWEAK × ESR). TWEAK: tumor necrosis factor-like weak inducer of apoptosis; ESR: erythrocyte sedimentation rate. Scatterplot (TWEAK × CRP). TWEAK: tumor necrosis factor-like weak inducer of apoptosis; CRP: C-reactive protein. Scatterplot (MMP-1 × ESR). MMP-1: matrix metalloproteinase-1; ESR: erythrocyte sedimentation rate. Scatterplot (MMP-1 × CRP). MMP-1: matrix metalloproteinase-1; CRP: C-reactive protein.

Mean difference in indicators of underlying inflammation (ESR and CRP) by OA severity
The average ESR in group A was 14.4 ± 8.3 mm/h, group B was 24.2 ± 11.7 mm/h, and group C was 18.0 ± 12.9 mm/h, suggesting no significant difference between the groups (p > 0.05). The average CRP in group A was 0.3 ± 0.6 mg/dL, group B was 0.1 ± 0.3 mg/dL, and group C was 0.3 ± 0.5 mg/dL, suggesting no significant difference between the groups (p > 0.05).
Mean difference in TWEAK and MMP-1 by OA severity
The average TWEAK concentration in group A was 731.6 ± 457.8 pg/mL, group B was 507.4 ± 224.4 pg/mL, and group C was 210.3 ± 59.1 pg/mL. In the post hoc test, the average was lower in group C compared to groups A and B, with more severe OA. The average MMP-1 concentration of group A was 1121.4 ± 391.9 pg/mL, group B was 1347.4 ± 466.8 pg/mL, and group C was 768.3 ± 312.8 pg/mL, suggesting a significant difference between the groups. In the post hoc test, the average was lower in group C compared to groups A and B, with more severe OA (Table 1; Figures 6 and 7).
Comparison of means of TWEAK and MMP-1 by group.

TWEAK: tumor necrosis factor-like weak inducer of apoptosis; MMP-1: matrix metalloproteinase-1.

Comparison of means of TWEAK by group. TWEAK: tumor necrosis factor-like weak inducer of apoptosis.

Comparison of means of MMP-1 by group. MMP-1: matrix metalloproteinase-1.
Discussion
OA is characterized by cartilage destruction due to apoptosis in cartilage and damage of ECM and involves pathological signs such as osteophyte formation, subchondral sclerosis, and microfracture as well as minor inflammation in synovial membranes. Homeostasis of joint cartilage relies on the balance between anabolism and catabolism, and the change in this balance leads to joint destruction. 20 OA progresses from damage caused by physical stimulation, to cartilage cell reactions, and then to expression of various cytokines in an attempt to maintain the balance between these factors. 8
It has been assumed that OA is caused by various cytokines and the imbalance between MMPs and their inhibitors. In other words, various cytokines secreted by cartilage cells increase the expression of MMPs and thereby destroy ECM, leading to apoptosis and destruction of cartilage and thus contributing to OA. 4 Many studies investigated the action of cytokines in synovial fluid in relation to OA and reported that OA progression of OA depends on various cytokines. In particular, IL-1, TNF-α, and other cytokines that destroy cartilage are reported to play an important role in the disease onset by increasing the secretion of MMP-1, -2, -3, -9, and -13; aggrecanase; IL-8; IL-6; PGE2; NO; and other factors. 9 –12 Moreover, IL-1 and TNF-α increase the rate of glycoprotein destruction as well as the catabolism of cartilage substrate, suppress resynthesis, and prevent the supplementation of matrix components. IL-1 and TNF-α also accelerate the production of PGE2, which is related to OA symptoms. Among the factors induced by IL-1 and TNF-α, both MMPs and NO play an important role; the latter acts on cartilage cells, suppressing synthesis of proteoglycan and collagen and activates MMPs; subsequent upregulation by MMPs further accelerates the destruction of cartilage. In addition, NO accelerates the synthesis of PGE2 and cyclooxygenase 2 and also significantly contributes to the destruction of cartilage cells. Furthermore, many cytokines are found to play various roles in the onset and progression of OA; much research is being conducted in order to identify cytokines and their action mechanisms as related to OA. 5,21 –24
We aimed to investigate the correlation between TWEAK and OA; TWEAK has been reported to contribute to joint destruction in rheumatoid arthritis, but its action mechanism in OA has not been identified. According to research, TWEAK induces cytokines prior to inflammation, regulates immune responses and angiogenesis, and controls apoptosis stimulation as well as tissue recovery and reformation. TWEAK is known to induce the production of ICAM-1, E-selectin, IL-8, and MCP-1 in endothelial cells as well as many inflammatory substances including MMP-1, IL-6, IL-8, and RANTES in synovial cells and fibroblasts. 17 –19 TWEAK performs its biological function by reacting to the receptor Fn14, which is widely present in various tissues and whose expression substantially decreases in damaged, inflammatory, or regenerated tissues. 8,25 When Fn14 is combined with TWEAK, it activates various signal transduction processes involving nuclear factor-κβ (NF-κβ), mitogen-activated protein kinases. In particular, NF-κβ induces the formation of various cytokines and MMPs. 23,26 TWEAK not only induces the formation of MMPs in cartilage cells but is also known to suppress chondrogenesis and osteogenesis in an in vitro model, which implies the possibility of TWEAK being involved in OA pathogenesis. 19 Chicheportiche et al. reported that TWEAK induces MMP-1 in dermal fibroblasts of healthy individuals and synovial membrane cells of patients with rheumatoid arthritis and OA as well as inflammatory cytokines and chemokines including PGE2, IL-6, IL-8, and RANTES. In the same study, TWEAK was found to strengthen pro-inflammatory responses of TNF and IL-1β and accelerate angiogenesis. 27 In summary, the TWEAK/Fn14 pathway is assumed to be involved in the pathology of joint diseases through various mechanisms such as deposition of pro-inflammatory cells as a result of formation of chemokines and cytokines and proliferation of progenitor cells required for angiogenesis acceleration and tissue recovery. However, the actions of TWEAK in joint tissue regeneration or recovery are complex. While TWEAK stimulates precursor cells and accelerates tissue regeneration, continuous expression of TWEAK/Fn14 in chronic arthritis such as rheumatoid arthritis leads to excessive production of chemokines, cytokines, and MMPs. As a result, it destroys joint tissues and interferes with the differentiation of precursor cells, suppressing tissue regeneration.
In order to investigate whether TWEAK plays a part in inducing cytokines as in inflammatory arthritis, we simultaneously measured MMP-1 expression, which is one of the cytokines induced by TWEAK.
There are various studies on the correlation between MMP-1 and OA. According to Vincenti and Brinckerhoff, MMP-1 is produced in cartilage cells, osteoblastic cells, and synovial cells and causes decomposition of type 1, 2, and 3 fibers in ECM as well as destruction of cartilage, thus contributing to OA progression. 28 MMP-1 expression remains low in normal cells and enables the regeneration of healthy cartilage. However, the expression increases in pathological conditions, causing substantial destruction of connective tissues. In other words, the expression level of MMP-1 is higher in cartilage cells with OA than in normal cartilage cells. Researchers suggested that when TWEAK is expressed and MMP-1 is induced, TWEAK may play a part in OA progression. In this study, synovial fluid of patients with OA was extracted to investigate the correlation between TWEAK and MMP-1, and a positive correlation was found. Therefore, we assume higher levels of TWEAK lead to higher expression of MMP-1, and that this can contribute to OA progression.
The levels of TWEAK and MMP-1 were high in the early stages (groups A and B) of OA and decreased in later stages (group C). In other words, OA progression due to TWEAK and MMP-1 takes place in the relatively early stage of the disease. However, based on the comparison of TWEAK and MMP-1 between groups, groups A and B did not show a difference in TWEAK in the post hoc test. Although there was no statistically significant difference, the average concentration of MMP-1 was higher in group B than in group A. We believe this is due to the relatively small sample size, and further research involving a larger sample will be needed to investigate the difference in expression levels according to the disease stage.
In this study, to investigate the OA stage in which TWEAK has an effect, synovial fluid was collected and classified using KL grades according to OA severity, and concentration of TWEAK and MMP-1 were analyzed. Both TWEAK and MMP-1 were highly concentrated in early stages (groups A and B) but decreased in later stages (group C) of OA. As described above, many cytokines are active during the second stage of OA, and it is assumed that TWEAK and MMP-1 become active when both anabolism and catabolism are active. Then, as cartilages are destroyed, cartilage cells and anabolism decrease and the concentration of TWEAK and MMP-1 may also decrease.
Although this study demonstrated that concentration of TWEAK and MMP-1 are relatively higher in early stages, it failed to identify whether group A (grade 0, 1), with almost no arthritis changes, or group B (grade 2, 3), with an intermediate level of arthritis, had higher expression of TWEAK and MMP-1. The average TWEAK concentration was higher in group A, and that of MMP-1 was higher in group B. However, there was no significant difference. We believe this is due to the small sample size in groups A and B, and that future research is needed to include larger samples for the analysis as well as for comparison between the subgrades (grades 0–4). Moreover, the distribution of the three OA stages based on KL grades was not known; further research will be needed to identify the KL grade that has the highest cytokine activity, which is found in the second stage of OA. If the action of cytokines in OA based on the KL grade can be identified, radiography can be used to guide treatment by controlling cytokines.
Conclusion
Concentration of both TWEAK and MMP-1 were high in the early stages of OA, which decrease as the disease progresses. This suggests that both factors play an important role in the early stages of OA and that their contribution decreases as the disease progresses. Further research will be needed to identify the specific pathogenic action mechanisms in OA and the correlations of TWEAK and MMP-1.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Ulsan University Hospital (Biomedical Research Center Promotion Fund, UUH-2014-06).