
Abstract
Rotating platform total knee replacement implants have been marketed to allow more precise approximation of normal knee kinematics and enhance patella tracking. At liberty of rotation, the distinct mobile polyethylene insert design does have its pitfalls in spite of purported merits. We report a case of lateral knee pain following rotating platform total knee replacement, attributable to iliotibial band impingement by the rotating polyethylene insert. Prompt treatment via arthroscopic release circumvented a traumatic and costly revision procedure.
Keywords
Introduction
While total knee replacement is often deemed the definitive treatment option for patients suffering from knee osteoarthritis, it has been reported that 20% of patients encounter persistent knee pain following surgery. 1 This has fueled the ongoing refinement and evolution of total knee implants, including the advent of mobile-bearing implants, which, in their attempt to improve patient satisfaction, 2 have also manifested issues unique to their construct. We report a case of iliotibial band impingement in a patient presenting with lateral knee pain following rotating platform total knee replacement, relieved via arthroscopic iliotibial band release.
Case report
A 68-year-old lady with 10-year history of bilateral knee pain presented to our unit with bilateral knee osteoarthritis. Fixed-bearing total knee replacement (PFC® Sigma®, Depuy Synthes, Raynham, Massachusetts, USA) was performed for her left knee, and, following satisfactory results, sequential total knee replacement for her right knee was performed 2 years later, this time with a rotating platform system (PFC Sigma Rotating Platform, Depuy Synthes). The femoral and tibial components used were sizes 2 and 1.5, respectively. The preoperative mechanical tibiofemoral angle for her right knee was 1° valgus (Figure 1).
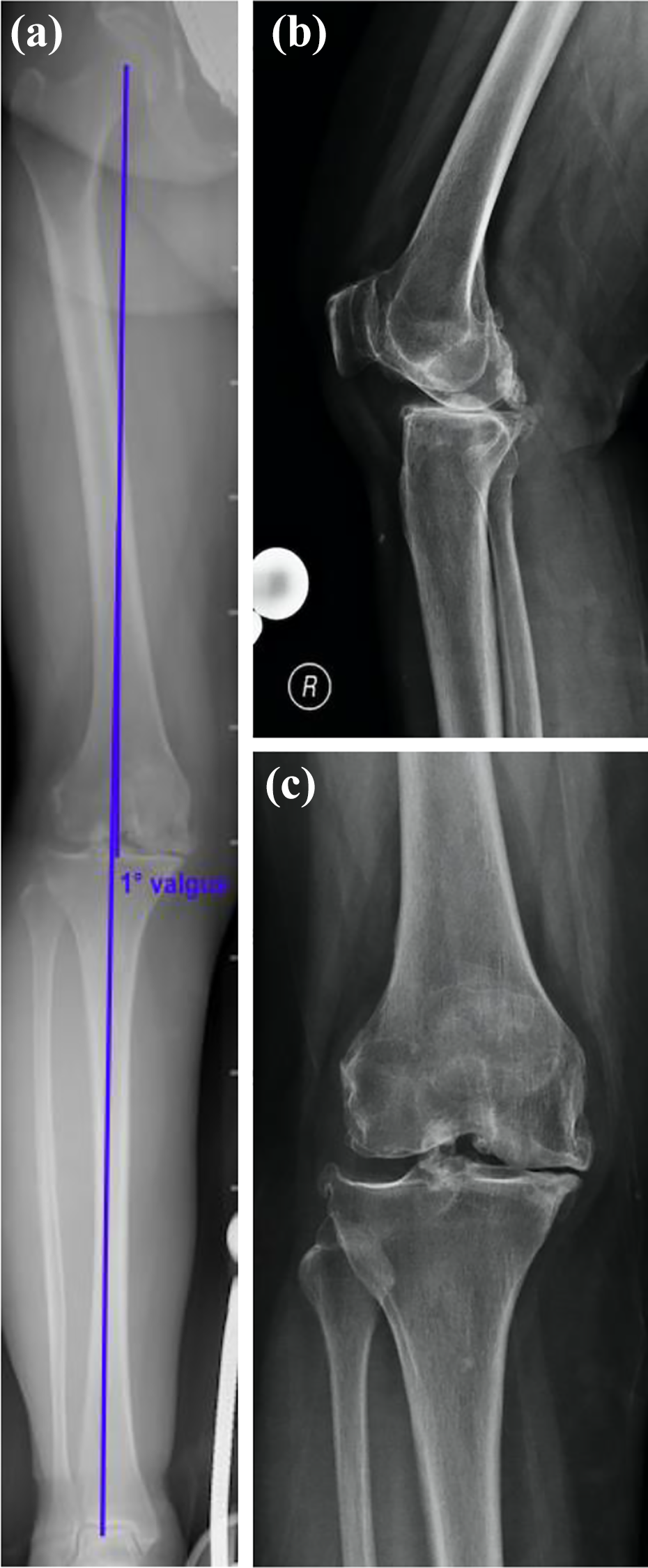
Preoperative X-rays of the right knee: (a) preoperative tibiofemoral alignment 1° valgus, (b) lateral view, and (c) AP view. AP: anteroposterior.
She presented with pain over the lateral aspect of her right knee 3 months postoperatively. Physical examination demonstrated tenderness over Gerdy’s tubercle. There was no knee effusion, and the range of motion of her knee was 0–125°, with crepitus felt at Gerdy’s tubercle on knee flexion and extension. Noble’s test was also found to be positive, during which the patient was noted to have tenderness over the Gerdy’s tubercle on extension of the flexed knee reproduced at 30° flexion. Iliotibial band impingement was suspected as a result of her clinical presentation. Inflammatory markers were normal. X-Ray and plain computed tomography did not show evidence of loosening. Rotation of the tibial tray was 7° external rotation with respect to Akagi’s line 3 (Figure 2(b) to (d)). The postoperative mechanical tibiofemoral angle was 6° valgus (Figure 2(a)). Injection of 2% lignocaine over Gerdy’s tubercle prompted transient improvement in pain, which reinforced our clinical impression of iliotibial band impingement.
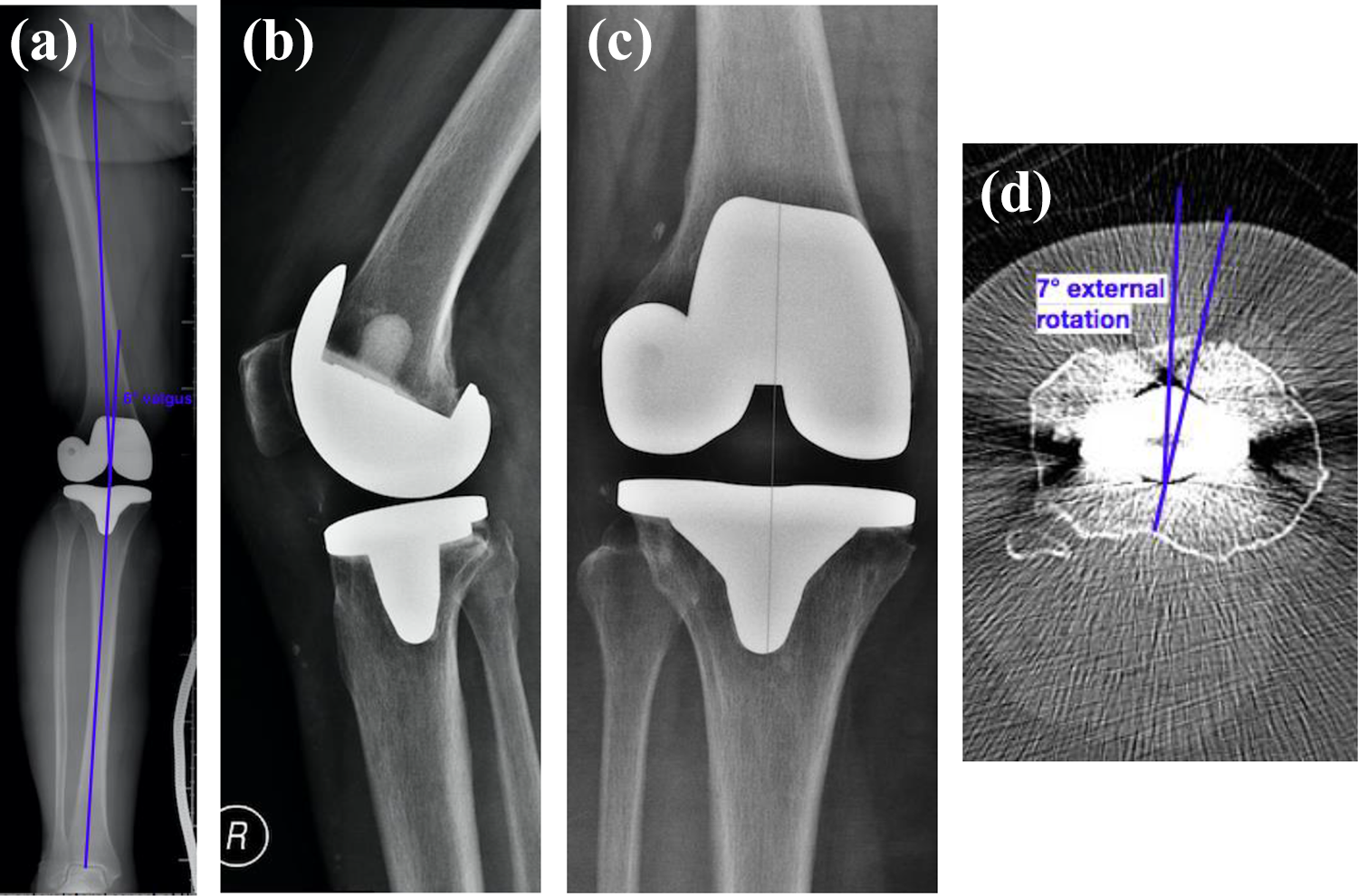
Postoperative images of the right knee: (a) postoperative tibiofemoral angle of 6° valgus, (b) lateral view of X-ray, (c) AP view of X-ray, and (d) tibial tray rotation was 7° external rotation with respect to Akagi’s line. AP: anteroposterior.
We endeavored to manage the patient’s iliotibial band impingement over a period of 6 months with a trial of physiotherapy, focusing on iliotibial band stretching and hip abductor strengthening. She was also provided with analgesia in the form of nonsteroidal anti-inflammatory drugs, as well as steroid injection to Gerdy’s tubercle, to satisfactory but unsustainable effect. In light of failure of conservative treatment, arthroscopic iliotibial band release was performed.
The knee was entered via anteromedial and anterolateral portals. Arthroscopic examination allowed for direct visualization of dynamic iliotibial band impingement, during which the iliotibial band was observed to be impinged on terminal knee extension by the anterolateral aspect of the rotating polyethylene insert (Figure 3(a) and (b)). The patient was also found to have significant synovitis with in-folding of synovium between the implant and insert, as well as thickening over the anterolateral area of the tibial tray (Figure 3(c)). The iliotibial band was released by means of radiofrequency ablation via VulcanTM probe (Smith & Nephew, Andhover, Massachusetts, USA), with which multiple horizontal cuts were created (Figure 3(d)). Synovectomy throughout the knee joint was also performed.
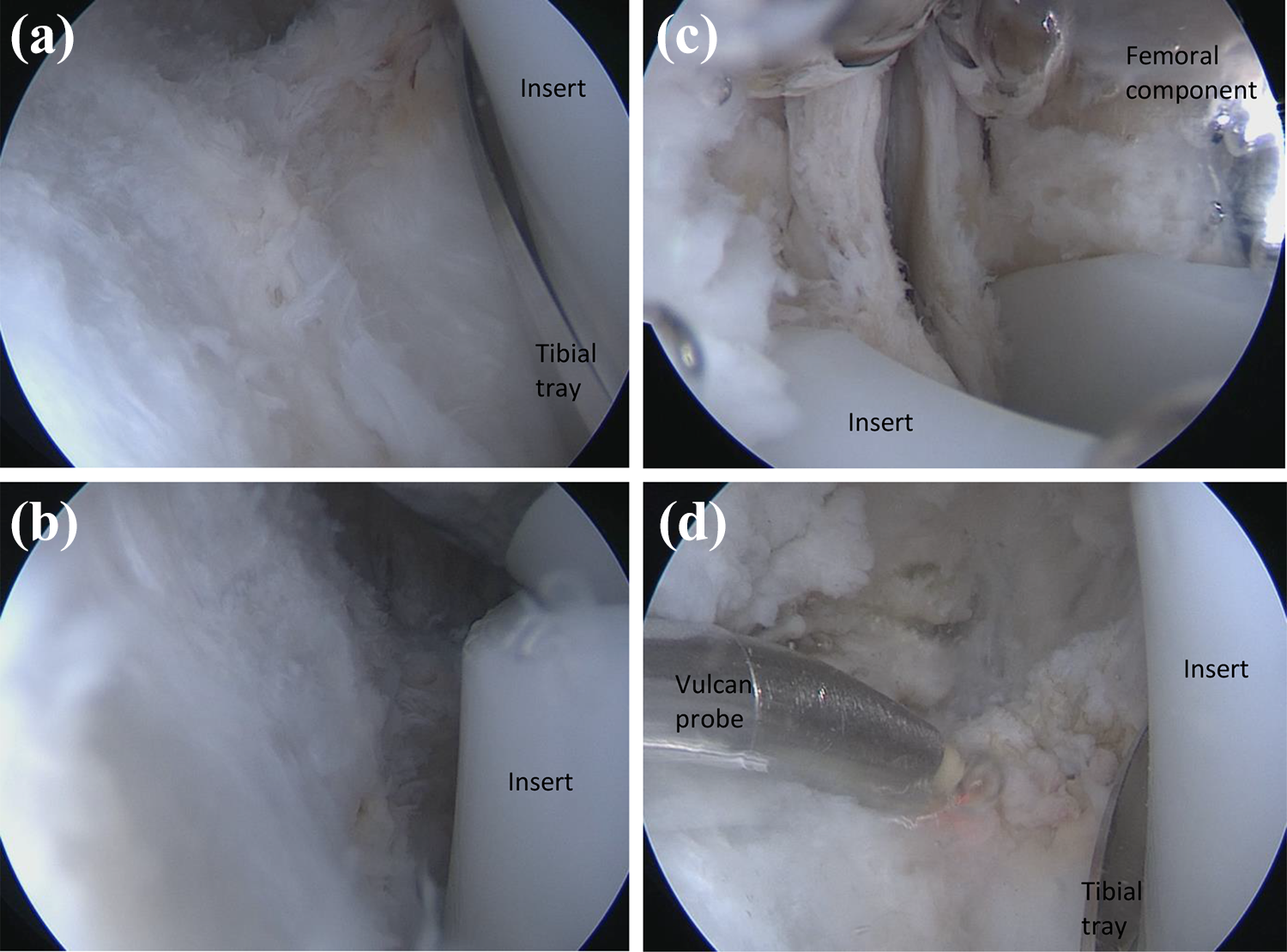
Arthroscopic findings: (a) anterolateral aspect of polyethylene insert with knee flexed, (b) iliotibial band impingement by anterolateral aspect of polyethylene insert with the knee fully extended, and (c) significant synovitis with in-folding of synovium between the insert and the implant, and (d) iliotibial band release via Vulcan probe.
Full weight-bearing, active and passive range of motion exercises were initiated immediately postoperation. The patient was last seen 19 months postoperatively. She revealed a significant reduction in pain. The range of motion of her right knee was 0–110° (Figure 4(a) to (c)). The left knee remained symptomatic all along.

Postoperative clinical photos: (a) anterior aspect of the knee showing good wound healing, (b) knee on full active extension, and (c) knee on full active flexion.
Discussion
The mobile-bearing rotating platform total knee replacement emerged in the 1970s, pioneered at the time by those in pursuit of a design that would be more akin to normal knee kinematics, consequently reducing polyethylene wear and component loosening. The ambition was to establish improved mobility and congruity in the tibiofemoral-bearing surface, with ensuing lower contact stress and constraint force in the implant. It was also postulated that the implant’s capacity to autocorrect rotational malalignment of tibial and femoral components via compensatory rotation at the polyethylene insert and tibial tray interface would improve patella tracking (Figure 5). Survivorship has been reported to be up to 98% at 20 years. 4 Bearing mobility, however, also renders it susceptible to dislocation, with bearing spinout rates identified to range from 0% to 2.2% at up to 20 years postoperatively. 5 –9 Stipulated advantages of the mobile-bearing system also appear to be conceptual only thus far, with several systematical reviews finding no statistical differences when compared to fixed-bearing systems in terms of clinical performance (clinical scores, range of motion, component alignment) as well as revision rates or adverse events. 10 –15

Rotating platform total knee replacement model demonstrating rotation at the polyethylene insert and tibial tray interface.
Iliotibial band impingement following total knee replacement is not a novel occurrence. However, to the best of our knowledge, our case is the first in the reported literature to occur in the rotating platform total knee replacement. Luyckx et al. previously reported a case series of iliotibial band impingement following a cruciate retaining, guided motion prosthesis (Journey®, Smith and Nephew, Memphis, Tennessee, USA), where an asymmetrical cam and post mechanism resulted in excessive anterior translation and internal rotation of the tibia, and therefore eccentric loading of the iliotibial band, causing pain. 16 Kwok et al. also noted a case of iliotibial band impingement but attributable to an overhanging tibial tray (Genesis II®, Smith and Nephew) provoking direct impingement. 17 In this case, we observed that the iliotibial band was impinged on the terminal extension of the knee, during which the external rotation of the tibia, as maintained by the “screw-home” mechanism of the knee, brought about anterolateral overhanging of the polyethylene insert. 18
This posed as a diagnostic challenge on account of the radiolucency of the offending polyethylene insert. The impingement was also compounded by an element of insert oversizing, as the prosthesis dictated sizing of the polyethylene insert according to that of the femoral component, which was sized larger than the tibial component in this case. We also speculate that compensatory relative internal rotation of the polyethylene insert, in its attempt to autocorrect documented 7° external rotational malalignment of the tibial tray, exacerbated impingement symptoms due to perpetual anterolateral overhang of the insert (Figure 6). Lastly, the postoperative mechanical tibiofemoral angle of 6° valgus also aggravated symptoms, as resulting hip adduction is expected to stretch the iliotibial band.
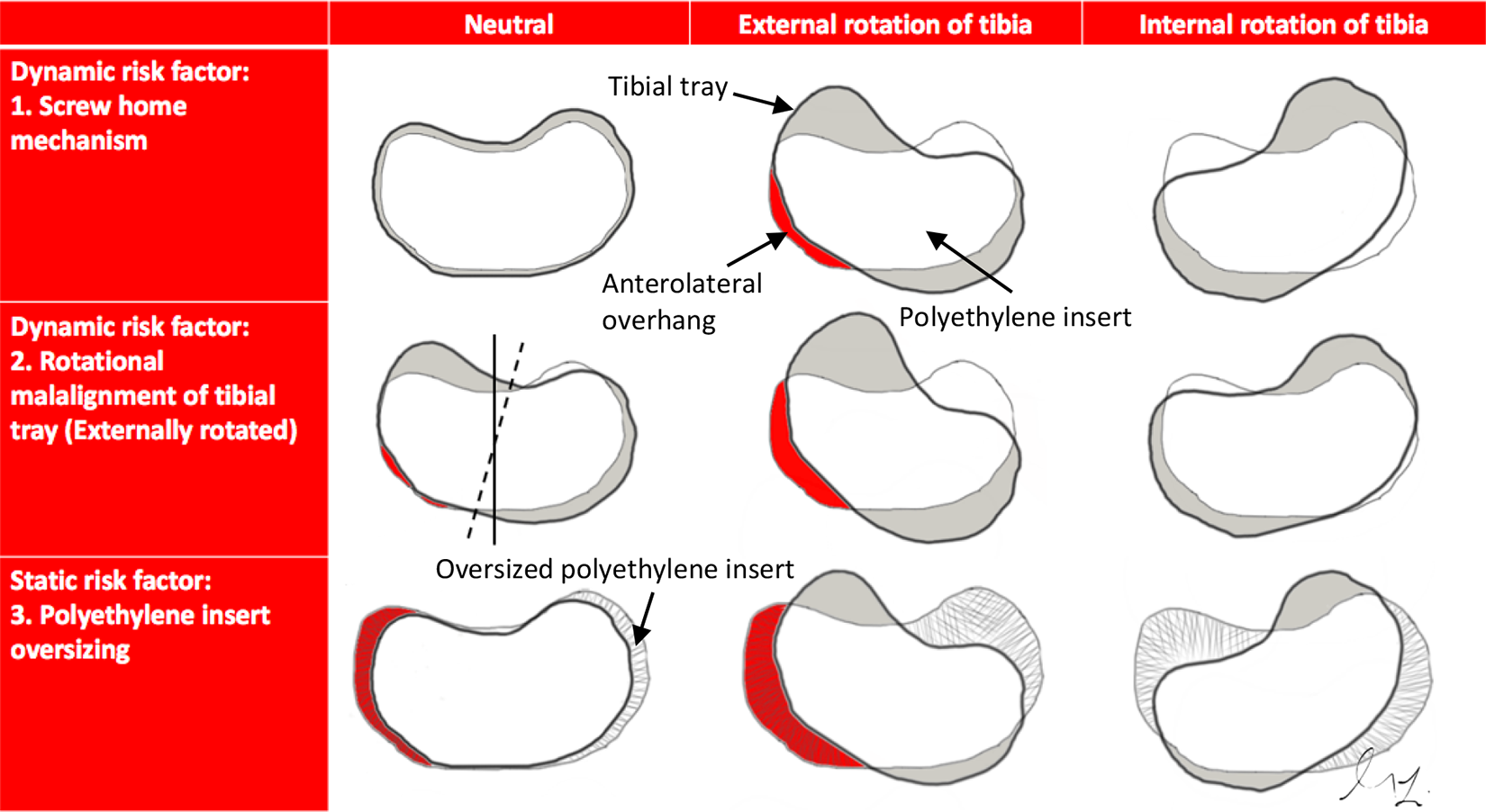
Table illustrating dynamic and static risk factors contributing to iliotibial band impingement unique to rotating platform total knee replacements.
It is postulated that iliotibial band impingement arises from friction generated in the iliotibial band due to repetitive motion against the lateral femoral condyle, culminating in underlying soft tissue compression and bursal inflammation. Arthroscopic treatment of iliotibial band impingement refractory to conservative management via resection of the lateral synovial recess has been previously established. 19 Kwok et al. also reported complete symptomatic relief via an augmented arthroscopic approach with combined mini-open release of the iliotibial band in their experience with iliotibial band impingement following total knee replacement. We found that an arthroscopic technique conferred diagnostic value in allowing direct visualization of the impingement as well as offered the potential for identifying concurrent soft tissue pathology if present. It also permitted exhaustive debridement of the knee to optimize symptom relief and maintained joint capsule integrity to minimize the risk of ensuing periprosthetic infection. The controlled release provided by arthroscopic means however, is unlikely to alter any mechanical malalignment.
Conclusion
In conclusion, we reported a case of lateral knee pain due to iliotibial band impingement following rotating platform total knee replacement, treated via arthroscopic iliotibial band release. We were able to attribute the impingement to an overhanging rotating polyethylene insert and identify both dynamic and static factors that acted as a basis for the impingement, namely normal knee kinematics maintained by the screw home mechanism, rotational malalignment of the tibial tray, oversizing of the polyethylene insert, and valgus tibiofemoral alignment. The case offers a humble yet intriguing contribution to the ongoing debate attempting to define superiority between fixed and mobile-bearing total knee replacements, which will warrant larger scale studies with longer follow-up, for the establishment of a consequential conclusion. We also recommend a high index of suspicion for iliotibial band impingement following rotating platform total knee replacement, seeing as, while easy to be overlooked owing to dynamic impingement and polyethylene radiolucency on imaging, timely diagnosis can prevent traumatic and costly revision procedures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.