
Abstract
Purpose:
Adhesive capsulitis of the hip (ACH) is not a well-defined disease entity. We evaluated the change in the clinical features of patients whose chief complaint was inability to sit cross-legged on the floor. All patients had painful limitation in hip joint motion. Based on the diagnosis of ACH, active stretching exercise (ASE) was recommended.
Methods:
In February 2013 and June 2014, a total of 44 patients (50 hips), who visited outpatient clinic in 2011, were evaluated by telephone interviews. Recovery of hip motion was analyzed according to compliance with ASE and abnormalities found on plane radiographs and magnetic resonance (MR) images.
Results:
There were 27 women and 17 men with mean age of 51.7 years. In the first telephone interview, 40 patients (45 hips) reported improvement in hip motion but 4 patients (5 hips) reported absolutely no improvement. Compliance with ASE did not affect recovery of motion (p = 0.225). On plain radiographs, 10 patients (22.7%) had abnormal finding in both hips. Those abnormal findings were not correlated with symptom and did not show adverse effect on motion recovery. Sixteen patients took MR images outside, and abnormal findings such as round ligament or labral tear were observed in nine patients. Those abnormal findings neither correlated with the symptom nor affected motion recovery adversely. In the second telephone interview, nine hips of further improvement and two hips of recurrence were identified.
Conclusions:
Most cases showed improvement in the range of motion with or without ASE. Surgical treatments including arthroscopy seemed to be unnecessary for these patients.
Keywords
Introduction
Since Caroit et al. introduced the concept of adhesive capsulitis of the hip (ACH) in 1963, 1 less than 20 articles have reported on this condition. 1 –13 All of them were case reports or case series of small numbers of patients and included many cases secondary to underlying conditions like marked degenerative arthritis in addition to primary cases. Primary or idiopathic ACH is characterized by a painful limitation in active and passive hip motions without concomitant pathology or antecedent trauma in the hip joint. 2 –4,12 The reported cases showed very variable prognosis with variable treatments.
At some time, a group of patients with decreased hip motion started to be recognized in outpatient clinic. Their chief complaint was “I cannot sit on the floor” or “I cannot take tailor’s position” (Figure 1). The symptom arose suddenly without any trauma. There was no difficulty in walking or running, but sudden rotation involving pivoting on the affected leg could produce sharp pain. All patients had painful limitation in hip joint rotation, usually more in external rotation and abduction. No remarkable abnormalities were detected on plain radiographs except for mild degenerative changes. In early cases, bone scintigrams were taken, but no abnormal findings were detected in most cases. Magnetic resonance (MR) imaging was done rarely without any significant findings. Under the diagnosis of ACH, patients were recommended to do active stretching exercise (ASE) to increase the rotation and abduction of the affected hip. In this study, the characteristics of the patients and their clinical course were analyzed retrospectively.

A 49-year-old woman complaining of inability to sit cross-legged on the floor.
Materials and methods
This study was performed with the approval of the institutional review board of our hospital (H-1306-005-493). During 2011, a total of 44 patients visited our outpatient clinic with the aforementioned chief complaint. One patient was lost to follow-up and 44 patients (50 hips) were included in the final analysis. All patients had no antecedent event for the sudden onset of the disability. All patients had no problem in usual walking and running. Many patients remembered that they had sharp hip pain when turning to a direction with the affected leg bearing weight; this pain was evident from the beginning and decreased gradually. On physical examination, the motion of the affected hip was limited in external rotation and abduction with pain at the conclusion of the motion. There was also some limitation in internal rotation with end pain. However, there was no limitation in flexion and extension without any flexion contracture. Plane radiographs demonstrated no remarkable abnormalities except mild degenerative changes. Patients were recommended to do ASE, pushing down the affected knee in the tailor’s position as much as possible. Patients were followed up every 6 weeks.
In February 2013, patients were evaluated by telephone interview concerning the recovery of hip motion. The recovery of the hip motion was expressed in percentage by the patient. The compliance of patients to the ASE was graded as good for exercise done 2 times or more a day, fair for exercise done once a day, and poor for no exercise. The results of the recovery in hip motion were analyzed with respect to the compliance to stretching exercise and abnormalities found on plane radiographs and MR images. In June 2014, another telephone interview was done to evaluate further improvement or recurrence.
Results
There were 27 women and 17 men with a mean age of 51.7 years (range: 30–74). Four patients were in their 30s, 11 in their 40s, 21 in their 50s, 6 in their 60s, and 2 in their 70s (Table 1). Affected side was the right in 21 patients, left in 17, and bilateral in 6.
Age-group and sex distribution of patients.

In the first telephone interview, 40 patients (45 hips) reported improvement in hip motion but 4 patients (5 hips) reported absolutely no improvement. Twenty-eight patients (32 hips, 64%) had a recovery of more than 80%. In these patients, recovery took 15 months on average (range: 0.3–18) after the onset of the symptom. Among them, 19 patients (22 hips, 44%) had complete recovery in an average of 9.8 months after the onset of the symptom.
Compliance to the stretching exercise was good in 21 patients, fair in 12, and poor in 11. The compliance did not affect the recovery in motion (p = 0.225, Kruskal–Wallis test). On plain radiographs, 10 patients (22.7%) had abnormal finding in both hips. Those include acetabular spur in four patients, bump in the femoral neck in two patients, and both in four patients. In only one patient, symptomatic hip showed more severe change and in the other nine patients, only one hip was symptomatic, or the symptomatic hip showed less severe change suggesting no relationship between the radiographic abnormal finding and symptom (Figure 2). Acetabular spur or femoral neck bump did not show adverse effect on motion recovery (p = 0.286 and 0.667, respectively).
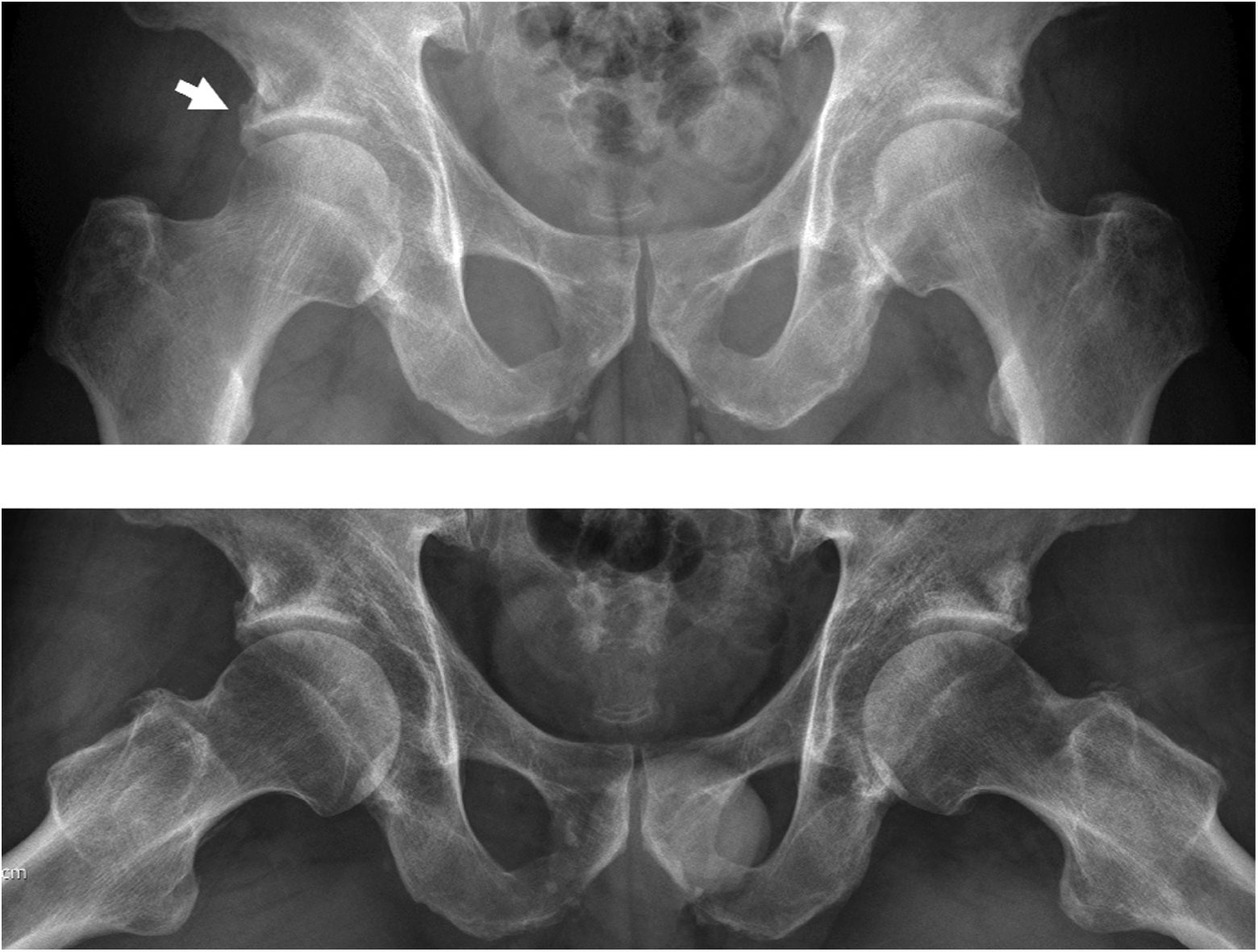
A 53-year-old man with limitation of motion in the left hip. Plain radiographs show mild degenerative spur change in both hips but more severe in asymptomatic right hip (arrow).
Sixteen patients took MR images elsewhere and abnormal findings were observed in nine patients. These included round ligament abnormality in five patients, round ligament abnormality with capsular hypertrophy in one patient, labral abnormality in two patients, and iliofemoral ligament hypertrophy in one patient. In two patients, MR abnormal findings were observed in asymptomatic side (Figure 3). Of seven patients in which MR abnormal finding was observed in symptomatic hip, five patients had round ligament abnormality. However, this abnormality did not show adverse effect on motion recovery (p = 0.147, Mann–Whitney test). In the second telephone interview done more than 2 years after the first visit, further improvement was reported in nine hips and recurrence reported in two hips.

A 43-year-old woman with limitation of motion in the right hip. No abnormal finding is observed in plain radiographs. Coronal magnetic resonance image shows round ligament tear in the asymptomatic left hip (arrow).
Discussion
The range of hip motion improved remarkably in most patients of this study group without surgical treatment or manipulation. The clinical course of this patient group was quite similar to that of adhesive capsulitis of the shoulder. 14,15 Arthroscopic surgery had been recommended to large number of patients in other hospitals under the diagnosis of femoroacetabular impingement (FAI). However, the clinical features and image findings were not consistent with FAI and only the ASE was recommended. Until the last interview, no patient underwent any surgery and even the patients with persistent symptom did not want any surgical treatment.
ACH is not a well-established disease entity. 11,12 There have been small number of articles, with most being case reports or small case series. Primary ACH occurs without underlying pathology and antecedent trauma like the cases of this study. For early cases of this study, bone scintigraphy was done routinely to rule out intra-articular pathology like synovial chondromatosis. At that time, we experienced a case of synovial chondromatosis of the hip in which no remarkable abnormality was identified on plain radiographs. MR imaging or computed tomography was planned if abnormal findings were detected on bone scintigraphy, but very few cases showed abnormality on bone scintigraphy. Therefore, now bone scintigraphy is taken only in cases with persistent symptoms.
In previous reports, most ACH patients were middle-aged, but there was no sexual predominance. 11 According to our clinical experience, ACH occurred most commonly in middle-aged women. This impression was well matched with the data of this study (Table 1).
Main disability of our patients was limitation of hip motion, especially rotation and abduction, with pain at the end of motion. Most patients had full flexion and extension without any flexion contracture and had no limitation in walking and running. Many patients had sudden sharp pain with a giving way sensation when turning with the affected leg fixed on the ground, but the pain decreased or disappeared with time. Therefore patients’ main disability was inability to sit cross-legged on the floor; this is a big problem in this country because of lifestyle.
Byrd and Jones observed some intra-articular abnormalities arthroscopically in some cases, but they did not describe the relationship between the symptom and intra-articular abnormalities concretely. 8 In some patients of this study, abnormal findings in labrum, ligamentum teres, or capsular ligament were detected on MR images, but they were not interpreted to be related with the symptoms and prognosis.
In most patients, the range of motion improved markedly. After the report of Byrd and Jones, 8 we recommended ASE. However, there was no evidence that the exercise induced earlier or more recovery of hip motion. A few patients had persistent limitation, but they did not undergo any surgical treatment. As was recommended by Byrd and Jones, manipulation under anesthesia can be applied to those recalcitrant cases.
There were some limitations in this study. For the diagnosis of adhesive capsulitis, it might be necessary to confirm the decreased cavitary volume of hip joint or the pathological findings in joint capsule. 3,4,11,12 In no patient, arthrography or synovial biopsy was tried. The improvement in the range of hip motion was not evaluated by direct examination but by telephone interview. Patients were recommended to be followed up every 6 weeks but no patients took follow-up examination more than three times. The validity of self-assessment of the range of hip motion was uncertain. It might be inaccurate numerically but it was not thought to affect the results remarkably. The criteria of the compliance with the stretching exercise were set arbitrary, because no good reference was found.
This study is the largest case series of ACH with the longest follow-up so far. The incidence of ACH was higher than expected. It might be the result of the lifestyle, sitting on the floor, in this country. In most patients of this study, the range of the hip motion improved spontaneously usually within 2 years. This clinical course suggested that the pathophysiology of this patient group was identical to that of adhesive capsulitis of the shoulder in high possibility and ACH might be a correct terminology for this condition.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant (no. 06-2003-063) from the Institution Research Fund.