
Abstract
Background:
Tears of the glenoid labrum are common after dislocation of the glenohumeral joint. The outcome for healing or surgical reconstruction of the glenoid labrum relies on the extent of its vascularization. This study aims to evaluate the glenoid labrum blood supply and to determine its regional vascularity.
Materials and Methods:
A total of 140 shoulders (30 male and 40 female cadavers) were examined: mean age 81.5 years, range 53–101 years. All blood vessels around the glenohumeral joint were dissected and recorded. Ten specimens with the glenoid labrum and fibrous capsule attached were randomly selected and detached at the glenoid neck and subjected to decalcification. Sections (10–20 μm) were cut through the whole thickness of each specimen from the centre of the glenoid fossa perpendicular to the glenoid labrum at 12 radii corresponding to a clock face superimposed on the glenoid. Sections were stained using haematoxylin and eosin and then examined.
Results:
The blood supply to the glenoid labrum is by direct branches from the second part of the axillary artery, subscapular, circumflex scapular and anterior circumflex humeral and posterior circumflex humeral arteries, as well as branches of muscular arteries supplying the surrounding muscles.
Conclusion:
This study shows that the glenoid labrum has a rich blood supply suggesting that, regardless of the types of the glenoid labrum lesions or their management, an excellent outcome for glenoid labrum healing and joint stability is possible. The observations also suggest that the blood supply to the glenoid labrum is sufficient, enabling its reattachment.
Introduction
Tears of the glenoid labrum result in glenohumeral joint instability, which can also occur with glenohumeral dislocation. 1 In a study of patients with their first glenohumeral dislocation and those with recurrent dislocation, Kim et al. 2 noted that those with first-time dislocations/lesions of the glenoid labrum had a Bankart lesion (24.24%, n = 8), a free anterior glenoid labrum periosteal sleeve avulsion (ALPSA; 27.27%, n = 9), a bony Bankart lesion (12.12%, n = 4) and an adhesive ALPSA (3.03%, n = 1), while those with recurrent dislocations had a Bankart lesion (61.26%, n = 68), a free ALPSA (9.09%, n = 11), a bony Bankart lesion (11.71%, n = 13), an adhesive ALPSA (14.41%, n = 16) and a disruption lesion of the articular glenoid (0.9%, n = 1). Lesions of the anteroinferior glenoid labrum observed in first-time dislocation were found to be 66.6% (n = 22) and in recurrent dislocations 98.1% (n = 109).
Several studies 3 –11 have reported a significant correlation between labral fixation and glenohumeral translation. In contrast, Kim et al. 12 reported an insignificant correlation between the extent of the labral lesion and the frequency of glenohumeral dislocation.
The glenoid labrum increases the depth of the glenoid fossa by 50%, with a Bankart lesion decreasing the depth to 50% anteriorly. 13 Based on these observations, Howell and Galinat 13 assumed that the glenoid labrum plays a role in stability. Pouliart and Gagey 14 reported that the glenoid labrum stabilizes the joint by preventing the humeral head from shifting. Smith et al. 15 and Williams 16 added that it protects the articular surface and aids joint lubrication. The glenoid labrum contributes as much as 10–20% to the concavity compression of the glenohumeral joint, 17 –20 and thus the existence of an intact glenoid labrum is important for concavity compression in joint stabilization. According to Habermeyer et al., 21 while the glenoid labrum maintains the negative intra-articular pressure inside the glenoid, it also confers joint stability.
Despite the importance of the glenoid labrum and the high incidence of associated lesions, its blood supply has been rarely reported. 22 –25 Both Cooper et al. 24 and Abrassart et al. 22 reported that the glenoid labrum was supplied by branches of teres minor and infraspinatus, as well as the suprascapular, circumflex scapular and posterior circumflex humeral arteries, together with capsular and periosteal branches, with the superior and anterosuperior labrum being less well vascularized than the remainder. It is interesting to note that no blood vessels were observed arising from the underlying bone to supply the labrum. Later, many nutrient foramina were present on the capsular circumferential ridge which supply the glenoid bone. The glenoid labrum was found to be sparsely vascularized without any particular pattern of distribution. Nevertheless, the vascularity has been suggested to decrease with increasing age. 23,25 Therefore, the aims of this study were to evaluate the blood supply to the glenoid labrum and to determine its regional vascularity.
Material and methods
One hundred and forty shoulders from 70 formalin-embalmed cadavers (30 males, 40 females: mean age 81.5 years, range 53–101 years) were examined.
Skin and the superficial and deep fascia were completely removed from the shoulder region. Anteriorly, the anterior part of deltoid and pectoralis major and minor were cleaned, detached and reflected laterally to expose the brachial plexus, brachial artery and its branches. Fibrous and fatty tissue around and between the brachial plexus and its branches, the axillary artery and its branches, and the axillary vein and its tributaries was carefully removed by blunt dissection; the brachial plexus was then removed. The short head of biceps brachii and coracobrachialis were detached from the coracoid process, reflected distally and removed. The anterior circumflex humeral artery and its accompanying veins were cleaned using blunt dissection.
A direct branch from the second part of the axillary artery (named here the ascending glenoid artery and passing under the coracoid process towards the anterosuperior and superior aspects of the shoulder joint) was dissected and cleaned from proximal to distal.
Superiorly, trapezius was removed, while the proximal attachments of the middle and posterior parts of deltoid were released, following which the clavicle was removed. A lateral incision was made in the supraspinatus tendon insertion and gently reflected medially. The suprascapular neurovascular bundle was cleaned.
Posteriorly, infraspinatus and teres minor were sectioned near their insertions and reflected medially. The branches of the suprascapular vessels were then traced into the infraspinous fossa.
Following abduction of the upper limb, teres major and the superolateral aspect of subscapularis were removed. The posterior circumflex humeral artery and its branches and the accompanying veins and the axillary nerve were cleaned as they passed around the surgical neck of the humerus inferior to the shoulder joint. The lateral head of triceps was then removed and the long head was cleaned.
The subscapular artery and its branches and the subscapular vein and its tributaries were cleaned from proximal to distal. The circumflex scapular vessels and their branches and tributaries were traced and cleaned.
Ten specimens with the glenoid labrum and fibrous capsule attached were randomly selected, detached at the glenoid neck and subjected to decalcification: this enabled the tissues to be sectioned and stained using standard techniques utilizing paraffin wax embedding. Each specimen was decalcified using either a decalcifier containing hydrochloric acid (10%) for 4 months or a rapid decalcifier (10% of formic acid in distilled water) for 48 h. The tissue was then washed in phosphate buffered saline and embedded in paraffin wax using standard techniques. Sections (10–20 μm thickness) were cut through the whole thickness of each specimen from the centre of the glenoid fossa perpendicular to the glenoid labrum at 12 radii corresponding to a clock face superimposed on the glenoid. This resulted in a triangular-shaped section of tissue with the glenoid labrum and fibrous capsule attachment at the periphery. Sections were stained using haematoxylin and eosin.
Results
The blood supply to the glenoid labrum was observed and noted during the dissection of all 140 shoulders. The labrum receives its blood supply from: The ascending glenoid artery (Figure 1), a branch arises from the first, second and third parts of the axillary artery in 1.80% (n = 2), 92.50% (n = 130) and 5.70% (n = 4) of specimens, respectively: it was observed as a single branch in 91.40% (n = 128), two branches in 7.9% (n = 11) and three branches in 0.70% (n = 1) of specimens, with the branches supplying subscapularis, the superior and anterosuperior aspects of the fibrous capsule, the glenohumeral ligaments, the superior and anterosuperior aspects of the glenoid labrum (Figure 2), glenoid neck, coracoid process, both heads of biceps brachii tendons and their origin, coracobrachialis and the rotator cuff muscle tendons. The inferior glenoid artery, present in 82.85% (n = 117) of specimens arising from the posterior circumflex humeral (29.9%, n = 35), circumflex scapular (54.7%, n = 64) and subscapular (15.4%, n = 18) arteries (Figures 3 and 4). Ascending branches of the anterior circumflex humeral artery supplying the fibrous capsule and surrounding structures, contributing indirectly in supplying the glenoid labrum through its attachment to the joint capsule and adjacent bone (Figure 1). Capsular branches of the posterior circumflex humeral artery, which in all specimens passed through the fibrous capsule from its anteroinferior, inferior, posteroinferior and posterior aspects running through the fibrous capsule for variable distances before entering the joint. These capsular branches also supplied subscapularis, the glenohumeral ligaments and fibrous capsule: As they passed medially through the fibrous capsule, the branches supplied the anteroinferior, inferior, posterior and posteroinferior aspects of the glenoid labrum. The circumflex scapular artery which gave (a) capsular branches, seen in all specimens, supplying the anteroinferior, inferior and posteroinferior parts of the fibrous capsule and glenoid labrum, as well as the long head of triceps, subscapularis and teres minor; and (b) a branch present in 74.42% (n = 104) of specimens, named an ascending branch arising from the circumflex scapular artery 30 mm from its origin, at the lower border of the origin of the long head of triceps, ascending superomedially posterior to the origin of the long head of triceps and grooving the bone for a short distance accompanied by two veins (sometimes one), which passed towards the inferior aspect of the spinoglenoid notch, then curved medially to run in the infraspinous fossa inferior to the root of the spine of the scapula terminating as several superior and inferior branches supplying infraspinatus and teres minor and as capsular branches supplying the posteroinferior, posterior, posterosuperior and superior aspects of the fibrous capsule, the glenoid rim and the glenoid labrum. The suprascapular artery, which gave (a) an articular branch in the supraspinous fossa running laterally posterior to the root of the coracoid process parallel to the anterior aspect of the supraspinatus tendon passing through the distal aspect of supraspinatus and the superior aspect of the fibrous capsule to supply the superior region of the glenoid labrum and the origin of the long head of biceps, giving periosteal branches to the superior aspect of the glenoid neck and nutrient branches to the superior aspect of the glenoid neck and the posterior part of the root of the coracoid process: this branch was present in 85% (n = 119) of specimens; and (b) two or more branches were given in the spinoglenoid notch, which pierced the joint capsule from the posterosuperior and posterior aspects and supplied the posterior aspect of the supraspinatus tendon, fibrous capsule and glenoid labrum.

Anterolateral view of the left shoulder injected with coloured silicone showing branches of the ACHA. This shoulder was injected with coloured silicone as part of another study. ACHA: anterior circumflex humeral artery.

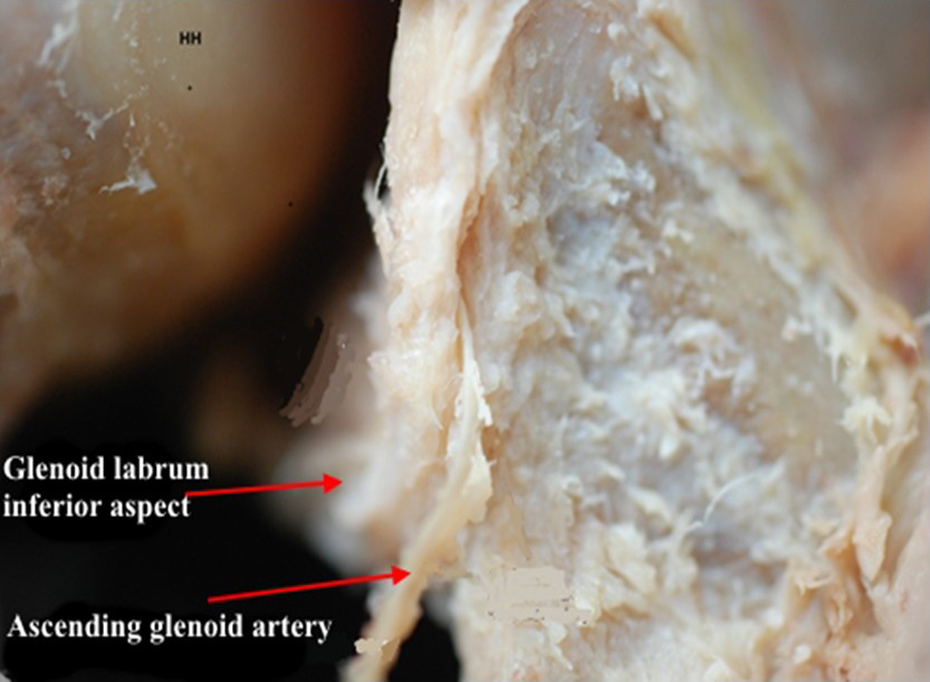
Lateral view of the right shoulder showing branches of the ascending glenoid artery supplying the superior and anterosuperior aspect of the glenoid labrum, the LHBT and the surrounding structures. LHBT: long head of biceps tendon.

Lateral view of the right shoulder showing the first branch (inferior glenoid branch) arising from CSA entering the inferior fibrous capsule and the glenoid labrum at the 6 o’clock position. CSA: circumflex scapular artery.
Inferior view of the right shoulder shows the first branch (inferior glenoid branch) arising and entering the glenoid labrum at the 6 o’clock position.
A summary of the regional blood supply to the glenoid labrum is shown in Figure 5.

Summary of the blood supply to the glenoid labrum. The circle represents the glenoid labrum. The blue region is supplied by ascending glenoid artery, the green region is supplied by anterior circumflex humeral artery, the red region is supplied by posterior circumflex humeral artery, the purple region is supplied by suprascapular artery and the yellow region is supplied by the subscapular and circumflex scapular arteries.
Histology
The glenoid labrum was fibrocartilaginous, being more fibrous at its free margin. It attached to the articular surface of the glenoid fossa centrally and glenoid bone peripherally. Some labral fibres also attached to the underlying glenoid bone, reaching as far as the bone marrow. In some regions, the fibrous capsule splits into an internal part, covering the internal aspect of the glenoid labrum, and an external part, covering the external aspect. The glenoid labrum was vascular with a variable distribution in the number and size of blood vessels in each region. Blood vessels were observed in the periphery with those from the fibrous capsule piercing the glenoid labrum (Figure 6).

(a) Low-magnification micrograph of the GL and fibrous capsule at the 10 o’clock position on the right side. (b) and (c) High-magnification micrograph showing BV. GL: glenoid labrum; BV: blood vessels.
Discussion
The blood supply to the glenoid labrum has been rarely reported. 22 –25 This study set out to address this and to determine whether there were regional differences in vascularity. Based on gross dissection, the current study indicated that (i) the superior and anterosuperior regions of the glenoid labrum receive an arterial supply from the ascending glenoid artery, articular branches of the suprascapular artery, periosteal branches of the circumflex scapular artery and muscular branches of subscapularis; (ii) the anteroinferior and inferior regions receive an arterial supply from periosteal branches of the circumflex scapular artery, muscular branches of triceps and subscapularis and the inferior glenoid artery, which itself can arise from either the posterior circumflex humeral, circumflex scapular or subscapular artery; and (iii) the posteroinferior and posterosuperior regions receive an arterial supply from periosteal branches of the suprascapular artery, muscular branches of teres minor and infraspinatus and occasionally an ascending branch of the circumflex scapular artery through periosteal branches, as well as direct branches to these regions: branches of the anterior and posterior circumflex humeral arteries pierce the capsule anterosuperiorly, anteroinferiorly, inferiorly and posteroinferiorly supplying the anatomical neck, some of which also supply the fibrous capsule and glenoid labrum.
Histologically, Abrassart et al. 22 and Cooper et al. 24 reported that the anterosuperior region of the glenoid labrum was less vascular compared to other regions. The current study observed that the anterosuperior region of the glenoid labrum was rich in blood vessels, suggesting that it cannot be less vascular than other regions. Prodromos et al. 25 are of the view that the glenoid labrum is sparsely vascularized but reported no particular pattern of distribution.
The histological findings of the current study found that the glenoid labrum was anchored to the periosteal layer of the glenoid bone, which is known to be rich in blood vessels, therefore it would be expected that the glenoid labrum would have a blood supply from both the periosteal layer and the bone. Yoneda et al. 26 reported that the management of Superior Labral tear from Anterior to Posterior (SLAP) type II lesions by debridement of the detached glenoid labrum and abrading the glenoid rim until it bleeds, then fixing the glenoid labrum by staples, produced excellent or good results in 80% of patients.
It could be questioned if the blood supply to the glenoid labrum is sufficient to enable its reattachment. DaSilva et al. 27 reported the management of SLAP type II lesions is by debridement of both the superior glenoid labrum, using a shaver, and the bony bed, using a burr until it bleeds: Interestingly, this procedure has been critical because it provides an optimal healing environment at the bone-labral junction, which is anchored by a non-absorbable suture. According to Ok et al., 28 double anchor sutures for SLAP type II lesions provide better restoration and stability. A double-looped corkscrew anchor procedure has shown encouraging results for SLAP type II lesion. 29 Open Bankart repair with suture anchors associated with the capsular shift procedure was more effective in small Bankart lesions compared to large ones. 30 Kamath et al. 31 reported that two double-loaded suture anchors were better or equal to three single-loaded suture anchors because it needed fewer anchor holes in the glenoid bone, thus decreasing the incidence of postsurgical glenoid fracture. In patients who underwent an arthroscopic bony Bankart bridge to treat a Bankart lesion, there was an average glenoid bone loss of 29% (n = 14): Millett et al. 32 observed that successful joint stability was achieved in 93%. The current study has shown that the glenoid labrum has a rich blood supply, which supports the excellent outcomes of glenoid labrum healing and joint re-instability observed, regardless of the types of the glenoid labrum lesions or their management. 33 –37,10 It is suggested that the blood supply to the glenoid labrum is thus sufficient to enable its reattachment. On the other hand, it could be questioned how and why incomplete or non-healing of labrum injuries occurs, leading to recurrent shoulder instability and poor blood supply to the glenoid labrum, such as in diabetic patients, which could impair healing of the glenoid labrum. 38
As this study was done on cadaveric shoulders and due to lack of medical history, only shoulders with completely attached glenoid labrum were subjected to histological investigation; therefore, this study was unable to investigate the blood supply in detached glenoid labrum due to shoulder pathologies. Further studies are recommended to investigate the blood supply in detached glenoid labrum.
It could be argued if there was any variation of the blood supply pattern that supply the glenoid labrum has been observed. The ascending glenoid artery which supplies the superior and anterosuperior aspects of the glenoid labrum showed anatomical variations in its origin and determined whether it was a single or multiple branches. It was observed to arise from the first, second and third parts of the axillary artery in 1.80%, 92.50% and 5.70% of specimens, respectively: it was observed as a single branch in 91.40%, two branches in 7.9% and three branches in 0.70% of specimens. The inferior glenoid artery which supplies the inferior aspect of the glenoid labrum was present in 82.85% of specimens arising from the posterior circumflex humeral (29.9%), circumflex scapular (54.7%) and subscapular (15.4%) arteries. Few shoulders were injected with coloured silicone aiming to evaluate the variation pattern in arterioles and venules that supply the glenoid labrum, but the coloured silicone could not reach to these small blood vessels due to their narrow diameters.
Conclusion
The blood supply to the glenoid labrum can be summarized by dividing the glenoid labrum into six regions: superior, anterosuperior, anteroinferior, inferior, posteroinferior and posterosuperior. The superior and anterosuperior regions receive a blood supply from the ascending glenoid and suprascapular arteries as well as muscular branches of subscapularis and supraspinatus. The anteroinferior and inferior regions receive a blood supply from periosteal branches of the circumflex scapular and inferior glenoid arteries as well as muscular branches of triceps and subscapularis. The posteroinferior and posterosuperior regions receive a blood supply from periosteal branches of the suprascapular artery, muscular branches of teres minor and infraspinatus and occasionally an ascending branch of the circumflex scapular artery as well as branches of the anterior and posterior circumflex humeral arteries which pierced the capsule anterosuperiorly, anteroinferiorly, inferiorly and posteroinferiorly supplying the anatomical neck, some of which also supplied the labrum through the fibrous capsule. The glenoid labrum also receives a blood supply from the underlying glenoid bone. The current study suggests that, regardless of the types of the glenoid labrum lesions or their management, an excellent outcome of glenoid labrum healing and joint re-instability is possible. In conclusion, the blood supply to the glenoid labrum is sufficient to enable its reattachment.
Footnotes
Authors’ note
All authors have participated in the research for this article.
Acknowledgements
The authors express their thanks to donors and their families, without them this study would not have been possible. They especially thank both the Centre of Anatomy and Human Identification at the University of Dundee and the Department of Anatomy at the University of Zawia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.