
Abstract
Rationale
Viscosupplementation (VS) with hyaluronic acid is widely used in the management of knee osteoarthritis. There is no clear recommendation on the decision-making to achieve VS.
Design
Based on extensive research of the literature and expert opinion, the members of the EUROVISCO (European Viscosupplementation Consensus Group) task force were asked to give their degree of agreement with 60 issues, using a Delphi method.
Results
The expert panel achieved unanimous agreement in favor of the following statements: It is recommended to assess pain on a visual or 10-point numeric scale before considering VS. VS can be considered for patients with pain scores between 3 and 8. A standard x-ray must be obtained before the decision of VS. If the x-ray is normal, osteoarthritis must be confirmed by MRI or computed tomography (CT) arthrogram before considering VS. The aims of VS are relieving pain, improving function, and reducing non-steroidal anti-inflammatory drug (NSAID) consumption. The use of VS must not be considered for treating an osteoarthritis flare. VS can be envisaged as a first-line pharmacological treatment in patients having a contra-indication to NSAIDs or analgesics. VS can be considered in patients with contra-indications to arthroplasty. In the case of severe comorbidities (diabetes, hypertension, gastrointestinal disorders, renal failure), VS can avoid the use of potentially dangerous treatments. VS can be considered in patients receiving antiplatelet agents, vitamin K antagonists, and direct factor Xa or thrombin inhibitors. Five other statements obtained a high level of consensus.
Conclusion
These recommendations, illustrated in a decision algorithm, have been established to help practitioners in the decision-making of knee VS.
Introduction
Osteoarthritis (OA) of the knee is an extremely frequent disorder in patients aged above 50 years, 1 but it can occur in younger subjects, notably in the case of post-traumatic OA. 2 The frequency of knee OA is constantly increasing due to population aging and the increasing numbers of overweight subjects, in particular in Western countries. 3 Treatment of knee OA is multidisciplinary and designed to reduce painful phenomena and also to maintain a functioning joint for as long as possible. It is based mainly on nonpharmacological measures (weight loss in the case of overweight, regular and appropriate exercise, lifestyle change) that can be associated with pharmacological measures. 4 Of these, topical non-steroidal anti-inflammatory drugs (NSAIDS) and analgesics are proposed as first-line treatment, or in the case of nonresponse to the latter and in the absence of contra-indication, oral NSAIDs are used.5 -8 Under certain conditions, symptomatic slow-acting drugs for OA and food supplements can be helpful to manage long-term symptoms and reduce the consumption of analgesics and the potentially more dangerous NSAIDs. 9 To reduce the use of systemic potentially harmful treatments, intra-articular injections (AI) are recommended. 10 Corticosteroids are indicated in the case of OA flares with a joint effusion. 6 Viscosupplementation (VS) by hyaluronic acid (HA) injection is indicated in mild to moderate forms of knee OA to reduce pain and improve joint function in periods devoid of inflammatory flares. 6 Used for more than 30 years, VS is recommended by numerous learned societies,6,7,11 -14 sometimes under certain conditions.8,15 Various expert groups have proposed a profile of patients that VS is particularly expected to benefit.16,17 Despite this, however, a few societies still do not recommend the use of HA injections, mainly due to a level of evidence considered insufficient. They maintain that the heterogeneity of the studies fails to provide unquestionable evidence in favor of VS. 18 The heterogeneity of the results may be related to differences in the efficacy of products containing HA, 19 likely due to wide differences between one product and another in terms of molecular weight, concentration, volume injected, intra-articular residence time, and viscoelasticity. The profile of the patient population may also greatly influence the result of VS as in the case of obesity and advanced radiological grade, which have both been identified as independent factors for poor response to VS. 20 At the last line of the manuscript the European Viscosupplementation Consensus Group, EUROVISCO, therefore examined the individual factors that may influence the decision to perform VS in a patient consulting for painful OA of the knee. Before making a therapeutic decision, the practitioners must consider the ability of the patient to comply with the physician’s recommendations. Before prescribing any treatment, they must take into account the patient’s needs and expectations (in this case, pain relief, doing recreational or competitive sport, professional commitments, postponing surgery), and also their fears (fear of becoming disabled, fear of surgery, fear of AIs, fear of conventional treatments, etc.), as well as their preferences and beliefs. For the physician who has to make the therapeutic decision, the level of pain and disability, imaging results, pain and functional scores, 21 and potential contra-indications related to concomitant medication and/or comorbidities are all parameters that may influence the decision-making.
The aim of this work was therefore to assess the relative importance of each of these items in the decision-making process of whether to perform VS in patients consulting for OA of the knee and to formulate recommendations for daily practice.
Methods
The EUROVISCO working group that met in Lyons on September 16 and 17, 2021, was composed of 10 members from 6 European countries (Belgium, France, Germany, Italy, Spain, and Turkey). This was a multidisciplinary panel of practitioners specializing in musculoskeletal system disorders. Seven of them were rheumatologists and there were 1 orthopedic surgeon and 2 rehabilitation medicine specialists. All were experienced in clinical research, cumulatively authoring more than 600 PubMed-referenced publications concerning OA. All have a clinical practice and had been performing VS and/or research on VS for more than 15 years. At each meeting since 2014, one member of the group was appointed chairman: They direct the debate and act as a moderator in case of divergence of opinion between group members. Due to the health crisis, 3 members of the group participated remotely via videoconference.
Six domains concerning the physician and 3 concerning the patient were discussed ( Fig. 1 ). The domains concerning doctors were the doctor’s objectives (10 questions), pain and handicap assessment (19 questions), knee OA imaging (15 questions), comorbidities (12 questions), concomitant medications (25 questions), and contra-indications (7 questions).
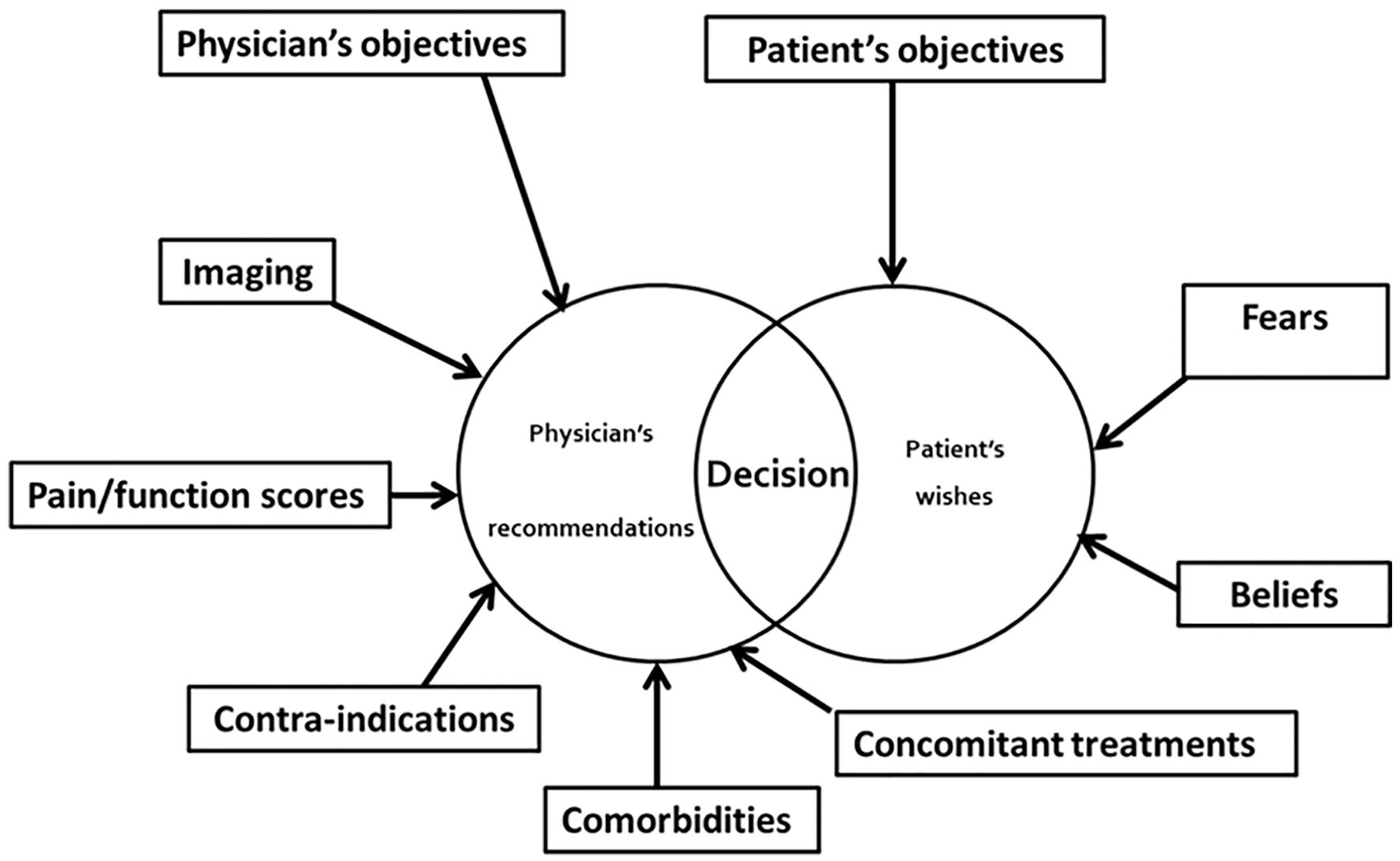
Factors influencing the decision-making for knee viscosupplementation.
Those concerning patients were the patient’s objectives (6 questions), fears (6 questions), and beliefs (8 questions). Finally, 4 questions were related to the follow-up of patients receiving VS for the first time.
The 112 questions were debated during working sessions, and for each, the members of the working group had to evaluate their degree of agreement with the question using the 9-point Likert scale. Scores 1 to 3 indicated “I disagree,” scores 4 to 6 “I agree under certain conditions only” and score 7 to 9 “I agree.” The vote was conducted using interactive software (Quizzbox©, Clermont-Ferrand, France), via voting handsets for those in-person or by smartphone for those participating online. Results of the vote were therefore available in real time for the group as a whole and for each member. The software generated a median agreement score for each question. The agreement or strength of recommendation was scored STRONG if the median score was 9 or 8, moderate for a score of 7, and low for a median score of 6. The degree of consensus was calculated from the number of experts giving a score ≥7 to the question asked. It was classified as UNANIMOUS if 10 out of 10 experts agreed with the proposal; it was classified as HIGH if 9 or 8 experts agreed with the proposal, and finally it was considered as MODERATE and LOW if 7 and 6 experts, respectively, agreed with this proposal. After each question, the result was discussed by the group, each member presented their opinions (conflicting or not), and a joint position was sought if possible. The items that received both a “strong” agreement and “unanimous, strong, or moderate” consensus are presented here in 2 formats: 18 general principles or recommendations.
Results
The general principles/recommendations that received full or partial consensus are displayed in Table 1 .
EUROVISCO Good Practice Recommendations for a First Viscosupplementation in Patients with Knee Osteoarthritis.
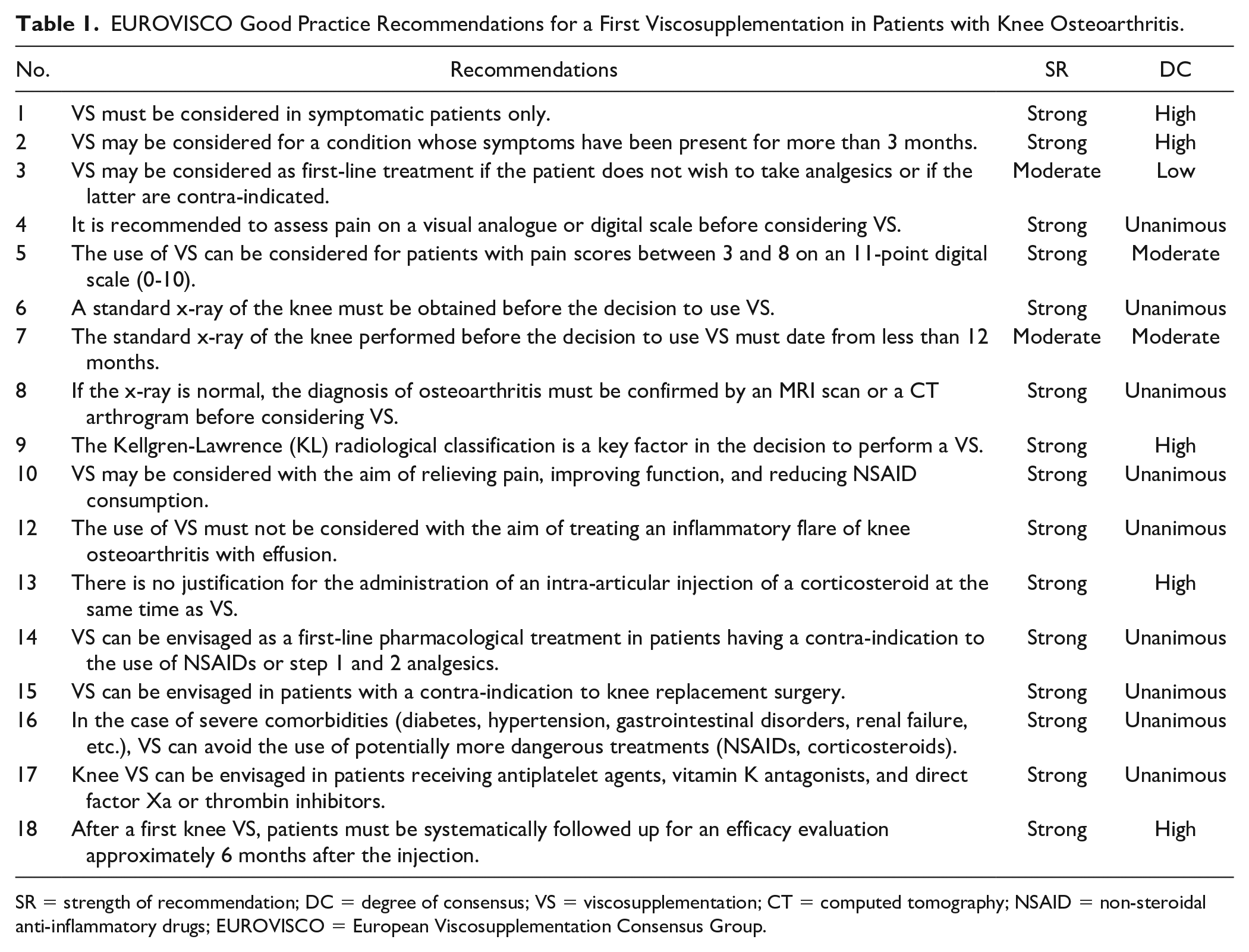
SR = strength of recommendation; DC = degree of consensus; VS = viscosupplementation; CT = computed tomography; NSAID = non-steroidal anti-inflammatory drugs; EUROVISCO = European Viscosupplementation Consensus Group.
1. VS must be considered in symptomatic patients only.
Strength of recommendation: Strong. Degree of consensus: High.
Eight out of 10 members agreed with this statement, but only 4 of them gave a score of 9/9 (mean 7.4 ± 1.4; median 8). Two considered that in certain situations the fortuitous discovery of knee OA, even if this was asymptomatic, could make VS worth considering, either because it had been symptomatic in the past (to avoid painful recurrence) or with the aim of chondroprotection, in particular in professional athletes.
2. VS may be considered for the condition whose symptoms have been present for more than 3 months.
Strength of recommendation: Strong. Degree of consensus: High.
Seven out of 10 members considered that the interval between the onset of symptoms and the VS should be at least 3 to 6 months, 1 expert recommended between 6 and 12 months, and the last 2 were against fixing a delay and for treating patients in the first month with the aim of optimizing the possibility of success of the VS.
3. VS may be considered as first-line treatment if the patient does not wish to take analgesics or if the latter are contra-indicated.
Strength of recommendation: Moderate. Degree of consensus: Low.
Only 6 members fully agreed with this recommendation. Four others gave their conditional agreement (contra-indication to analgesic treatments). One spoke about facilitating physical activity in case of failure of nonpharmacological modalities or in association with nonpharmacological treatment. The discussion revealed that the choice of the patient to take analgesics or not should be considered as a key parameter in the therapeutic decision, with the proviso that they had been clearly informed of the benefit and risks of the various therapeutic options available in their case.
4. It is recommended to assess pain on a visual analogue or digital scale before considering VS.
Strength of recommendation: Strong. Degree of consensus: Unanimous.
All members approved this recommendation but without making this evaluation compulsory. The principal argument in favor was to obtain a baseline pain value, thus permitting the greatest possible objective measurement of treatment efficacy during follow-up visits. In contrast, the working group did not recommend the systematic use of composite scores (Western Ontario and McMaster Universities Arthritis Index [WOMAC], Knee injury and Osteoarthritis Outcome Score [KOOS], Lequesne index) in everyday practice due to the long and fastidious nature of these questionnaires which are not suitable in that context.
5. The use of VS can be considered for patients with pain scores between 3 and 8 on an 11-point digital scale (0-10).
Strength of recommendation: Strong. Degree of consensus: Moderate.
The total consensus was obtained for considering the use of VS in patients claiming moderate pain scored 5 or 6/10 (mean 7.9). Eight experts out of 10 recommended VS in case of pain scored 7 or 8 and 6 experts in case of less intense pain scored 3 or 4. On the other hand, in case of minimal (0-2) or major (9-10) pain, the majority of voters only recommended VS under certain conditions (patient’s choice, failure, or contra-indication to other therapeutic options, contra-indication to surgery).
6. A standard x-ray of the knee must be obtained before the decision to use VS.
Strength of recommendation: Strong. Degree of consensus: Unanimous.
All members approved this recommendation; 6 of them have given the maximum score. Concerning the recommended x-ray view, the experts preferred a weightbearing anteroposterior view (unanimity), whereas 6 out of 10 favored lateral or skyline Merchant view of the patella and only half of them favored the posteroanterior view with flexion.
7. The standard x-ray of the knee performed before the decision to use VS must date from less than 12 months.
Strength of recommendation: Moderate. Degree of consensus: Moderate.
Seven experts considered that the x-ray should be less than 12 months old, even less than 6 months for the strictest. This is due to the fact that an old x-ray can underestimate the anatomical severity of the knee OA and result in a VS performed at an overlate stage, leading to therapeutic failure and prejudice for the patient. While the x-ray should ideally be as recent as possible, experts emphasize that it is not justified, except when there is a clinical reason to suspect rapidly progressing OA (major pain, recurrent or constant effusion) to repeat an x-ray if the patient has images dating from less than 12 months, essentially to limit patient exposure to ionizing radiation and also to limit the cost of the treatment.
8. If the x-ray is normal, the diagnosis of OA must be confirmed by an MRI scan or a computed tomography (CT) arthrogram before considering VS.
Strength of recommendation: Strong. Degree of consensus: Unanimous.
The response to this question was unanimous because the diagnosis of OA of the knee must be confirmed before the indication of VS is decided. The experts considered that if the x-ray is normal the 2 most relevant imaging examinations for the diagnosis of early OA of the knee are MRI and, in certain cases, CT arthrography.
9. The Kellgren-Lawrence (KL) radiological classification is a key factor in the decision to perform a VS.
Strength of recommendation: Strong. Degree of consensus: High.
With the exception of one expert, all the others said they based their decision for VS treatment on the radiological grade. This decision does not imply that early or late stages are not indications for VS. However, most experts consider that the physician’s duty to clearly inform the patient on their chances of treatment success and failure implies the need to base this information on the radiological grade. The fact is that all studies suggest that there are a lower percentage of responders in patients with KL grade III and especially grade IV.20,22,23,24 The experts were unanimous in approving the use of VS in grades II and III. Fewer of them considered the treatment conditional in grade I (5 experts out of 10). In grade IV cases, all experts recommend the use of VS conditionally, in particular in pauci-symptomatic forms, with the aim of delaying surgery by a few months or in case of the impossibility of a knee replacement (refusal from the patient or contra-indication).
10. VS may be considered with the aim of relieving pain, improving function, and reducing NSAID consumption.
Strength of recommendation: Strong. Degree of consensus: Unanimous.
A consensus was obtained on all 3 points; clinical trial data and the working group members’ personal experiences were all in agreement.
11. VS may be considered with the aim of delaying knee replacement surgery
Strength of recommendation: Strong. Degree of consensus: Moderate.
Seven out of 10 members considered that VS may be considered with the hope of postponing knee replacement surgery, as suggested by some studies conducted on health insurance databases.25 -28 Three other experts agreed with this proposal only under certain conditions (patient’s wish, temporary contra-indication to a knee replacement, need for substantial weight loss before surgery, etc.). On the other hand, the experts disagreed on the chondroprotective effect of HA (lack of consensus). While HA undoubtedly possesses a chondroprotective effect in vitro and in some animal models, 29 this effect has never been formally demonstrated in humans, despite studies suggesting an effect.30 -33
12. The use of VS must not be considered with the aim of treating an inflammatory flare of knee OA with effusion.
Strength of recommendation: Strong. Degree of consensus: Unanimous.
All members questioned concluded that VS was not recommended to treat a flare of knee OA. In their opinion, the flare of OA must be treated with NSAIDs or an AI of corticosteroids; HA lacks sufficient anti-inflammatory effect. The presence of large-volume effusion has been identified as a factor in the failure of VS. 24
13. There is no justification for the administration of AI of a corticosteroid at the same time as VS.
Strength of recommendation: Strong. Degree of consensus: High.
Nine out of 10 experts did not recommend the administration of an IA injection of corticosteroid at the same time as VS, and 1 considered that it could be envisaged under certain conditions. In contrast, in patients with knee OA with effusion, an IA injection of corticosteroid is justified to reduce the volume of effusion and related pain but must be performed before the VS (the experts recommend 3-4 weeks). Although we strongly discourage administering together steroid and HA mixed by the physician for the occasion, it is possible to inject products combining HA and triamcinolone approved by the regulatory agency for this purpose in the right indication. 34
14. VS can be considered as a first-line pharmacological treatment in patients having a contra-indication to the use of NSAIDs or step 1 and 2 analgesics.
Strength of recommendation: Strong. Degree of consensus: Unanimous.
All the experts approved the fact that, given its excellent safety and its analgesic effect, VS is the treatment of choice in subjects with a contra-indication to pain-relieving treatments (NSAIDs and step 1 and 2 analgesics) in case of insufficient benefit from nonpharmacological measures.
15. VS can be considered in patients with a contra-indication to knee replacement surgery.
Strength of recommendation: Strong. Degree of consensus: Unanimous.
All the experts agreed with this proposal but emphasized the fact that VS is not a substitute for a knee replacement. It is worth trying in patients with late-stage disease for whom surgery is contra-indicated, on the condition that the patient is fully informed of the risk-benefit ratio of VS, with little chance of long-lasting relief.
16. In the case of severe comorbidities (diabetes, hypertension, gastrointestinal [GI] disorders, renal failure, etc.), VS can avoid the use of potentially more dangerous treatments (NSAIDs, corticosteroids).
Strength of recommendation: Strong. Degree of consensus: Unanimous.
All the experts agreed with this proposal, the literature data confirming the excellent systemic tolerance of VS in comparison with NSAIDs and corticosteroids.
17. Knee VS can be envisaged in patients receiving antiplatelet agents, vitamin K antagonists, and direct factor Xa or thrombin inhibitors.
Strength of recommendation: Strong. Degree of consensus: Unanimous.
In patients treated with an anticoagulant drug, VS may be envisaged. The knee is not considered to be a “deep” joint and an AI may be performed without the need to temporarily withdraw anticoagulant treatment.35,36 HA, in contrast to the NSAIDs, does not induce an increased risk of bleeding, and therefore VS may be considered safe in these patients. The patient must, however, be warned of the risk of a skin hematoma at the point of injection. The use of a fine needle (21-23G) and ultrasound guidance are recommended by the experts to ease injection and limit the risk of bruising.
18. After a first knee VS, patients must be systematically followed up for an efficacy evaluation approximately 6 months after the injection.
Strength of recommendation: Strong. Degree of consensus: High.
All patients treated with VS must be followed up for evaluation of treatment efficacy. The authors all agree, as suggested in the literature, that the “treat-to-target” approach must be applied in the case of OA of the knee, as is done in the management of chronic inflammatory rheumatisms. In the opinion of the working group, this follow-up visit enables the next visit to be scheduled 6 months later in case of a good result and, if the result is insufficient, to change therapy by intensifying treatment or by deciding on surgery. The mean time of 6 months was selected, but in the opinion of 6 experts out of 10, this interval should be reduced to 3 months in case of severe OA and increased to 9 months in case of incipient forms.
The members of the working group then discussed the knowledge, expectations, fears, and beliefs of patients to whom VS is proposed for the first time. These comments are from the literature but are the fruit of their own long experience as VS practitioners through what patients say to them. Data are summarized in Table 2 .
What Patients Expect from Viscosupplementation of the Knee.
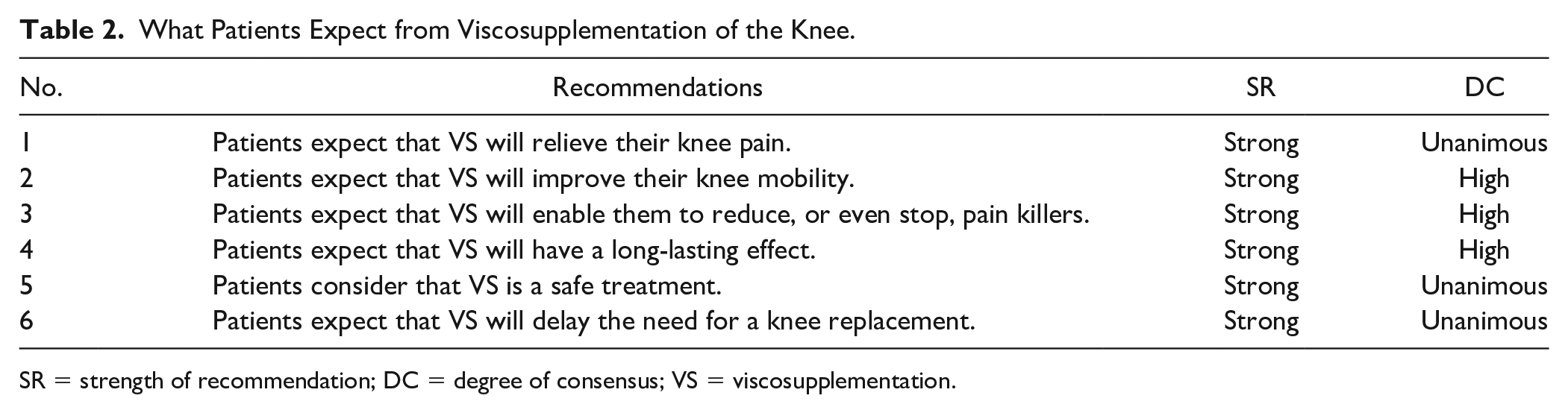
SR = strength of recommendation; DC = degree of consensus; VS = viscosupplementation.
1—Patients expect that VS will relieve their knee pain.
Level of approval: Strong. Degree of consensus: Unanimous.
2—Patients expect that VS will improve their knee mobility.
Level of approval: Strong. Degree of consensus: High.
3—Patients expect that VS will enable them to reduce, or even stop, pain killers.
Level of approval: Strong. Degree of consensus: High.
4—Patients expect that VS will have a long-lasting effect.
Level of approval: Strong. Degree of consensus: High.
5—Patients consider that VS is a safe treatment.
Level of approval: Strong. Degree of consensus: Unanimous.
According to the working group, VS is a treatment that most patients have heard of, because it has been performed in Europe since the mid-1990s. Before consulting a specialist in musculoskeletal disorders, they have heard information about VS from friends or family, their general practitioner (GP), or the media. It is therefore unsurprising that a strong level of approval and a high degree of consensus were obtained for these 5 points.
6—Patients expect that VS will delay the need for a knee replacement.
Level of approval: Strong. Degree of consensus: High.
Discussion
Here, the EUROVISCO group proposes 18 recommendations and a decision-making algorithm ( Fig. 2 ) for performing the first VS in naive patients consulting for knee OA. These recommendations take into account the clinical and radiological severity of knee OA, the objectives, comorbidities, and treatments, and especially the patient’s needs and wishes. For example, for personal reasons that are unknown by the practitioner, the patient may refuse to take any analgesic or anti-inflammatory treatment or undergo surgery.
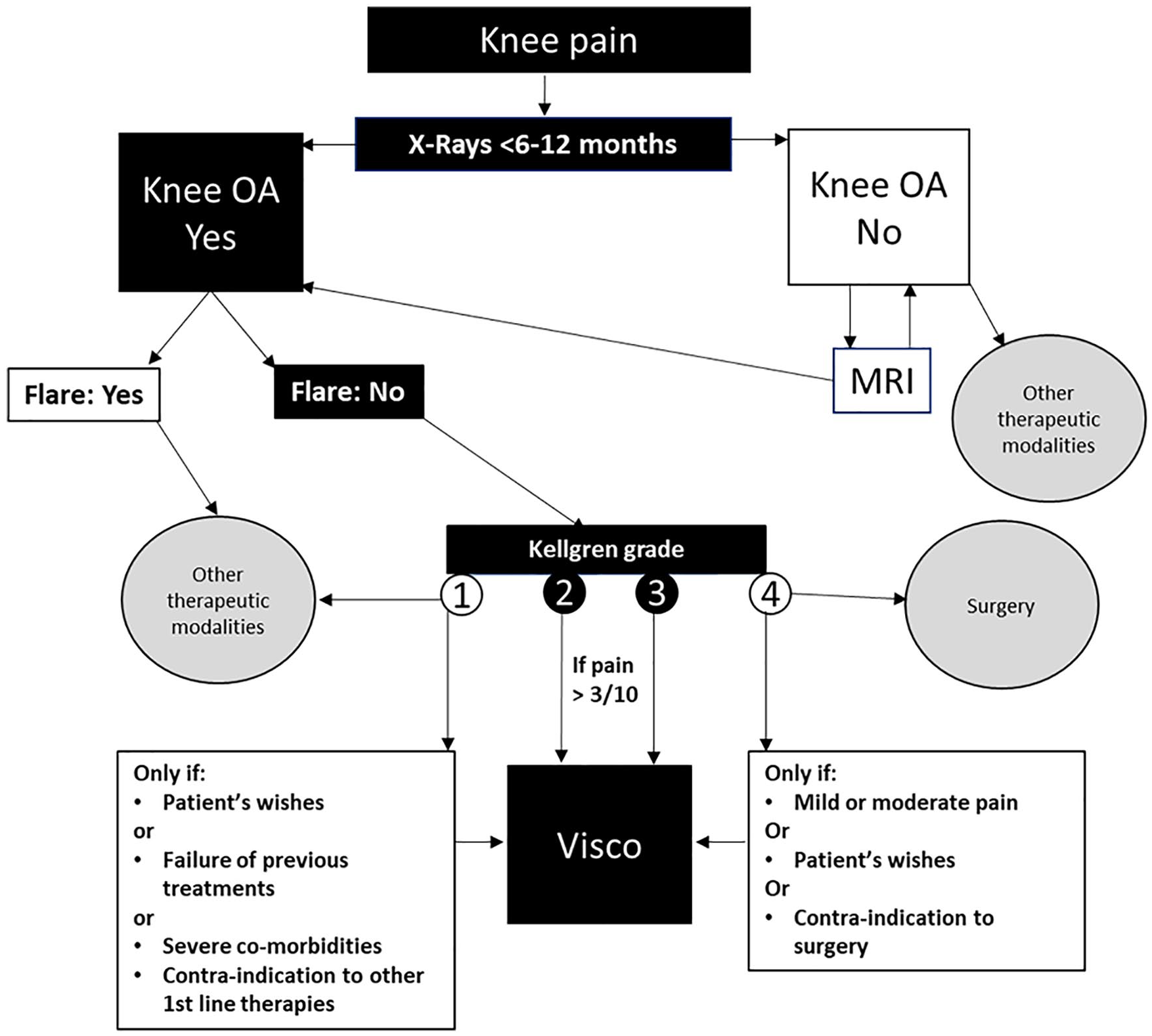
Decision algorithm for a first viscosupplementation in patients with chronic knee pain. OA = osteoarthritis; Visco = viscosupplementation.
The experts agreed on the fact that VS must be proposed to patients with symptomatic knee OA with a pain evaluated >3 on a 10-point scale, which is largely equivalent to the PASS threshold, 37 a level of pain that the subject considers unacceptable. For the working group, a minimum of 3 months of pain seems necessary before considering VS, corresponding to the minimum time required to judge if first-line noninvasive treatments are not efficient enough or no longer efficient. Nevertheless, as the patient’s opinion is an essential part of the therapeutic decision, recommendation number 3 stipulates that VS can be envisaged as the first pharmacological treatment if the patient refuses oral or nonpharmacological treatments. The same is true in the case of contra-indication to NSAIDs or analgesics. To determine that the pain level is sufficient and above all to assess any improvement, it is recommended to perform a pain assessment with a visual analogue scale or a digital scale, simpler and quicker than a complex composite score, which is essential during clinical trials but unsuitable for daily medical practice. In the experts’ opinion, a high level of pain (9 or 10 out of 10) justifies the discussion of other therapeutic measures (IA corticosteroids, step 2 or 3 analgesics, surgery in some cases). This is because the long onset of action (usually 4-8 weeks) does not make it the treatment of choice in hyperalgesic patients. A strong consensus was found concerning the need to recommend knee imaging before any decision to use VS. A standard x-ray, frontal, standing appears to be the simplest and least costly tool to confirm the diagnosis of OA and to assess its severity and extent. As some cases of knee OA can progress rapidly, an x-ray dating from less than 12 months (ideally less than 6) appears essential. In some cases of early OA, not yet visible radiologically, an MRI or CT arthrogram must be performed to be certain of the diagnosis of OA and to eliminate other joint pathologies not detectable on a standard x-ray (meniscus pathology, inflammatory or villonodular synovitis, synovial chondromatosis). Ultrasound examination is helpful for evaluating the presence of an effusion and synovial hypertrophy, 2 characteristics of OA of the knee, but is not mandatory for the diagnosis. As the radiological grade is a crucial element in the response to VS, the experts consider that the treatment must be prescribed in priority in grades II and III, for which the best results have been reported. They also recommend discussing patients with grade IV OA on a case-by-case basis. Indeed, we have observed some patients with very advanced stage disease who showed a spectacular response to VS. 38 The same observations were reported for obese patients. While some studies suggest a smaller percentage of responders in obese patients, 20 others failed to confirm these data.22,23 As obese individuals often have several comorbidities, such as diabetes or hypertension, VS is a safe alternative that must not be neglected, although the patients must be warned that the odds of success are lower than in normal body weight patients. The members of EUROVISCO also underlined the benefit of VS in patients in whom certain analgesics, NSAIDs, and/or corticosteroids are contra-indicated due to comorbidities (diabetes, hypertension, renal failure, GI tract disorders, etc.) and/or due to the treatments received for these.
The experts were unanimous in their opinion that the main aim of VS was to reduce pain and functional disability of the knee while reducing analgesic and anti-inflammatory treatments. In this respect, their experience confirms the literature data. All the clinical trials performed with currently licensed products have demonstrated these 3 effects, although the magnitude of the response can vary from one to another. 19 They were also of the opinion that due to its analgesic effect it could delay surgery without being able to arrest the degenerative process and prevent surgery in the long term.
VS is not a treatment for knee OA flares; the treatment for these is based on NSAIDs and IA injections of corticosteroids. 39 The latter two must not be given at the same time as VS but preferably a few weeks beforehand. In vitro studies have shown that corticosteroids have a damaging effect on the HA molecule, 40 radically impairing its rheological properties. However, clinical studies failed to show a difference at 6 months between HA alone or combined with a corticosteroid34,41 although at 1 and 3 weeks after injection the combination was significantly better than HA alone for most endpoints. The working group followed published recommendations on intra-articular techniques in patients treated with anticoagulants or antiplatelet agents. As the knee is a joint considered “superficial,” no specific precaution is necessary for VS, except for clearly informing the patient about the risk of skin hematoma. It is common sense to choose the finest possible grade needle and to use ultrasound or fluoroscopic guidance in difficult cases, for example, in obese individuals. In patients treated with vitamin K, an IA injection is not recommended if the INR (International Normalized Ratio) is over 3.
Finally, the experts underlined the importance of a follow-up. Numerous practitioners tell patients to consult only when significant pain has returned, but the working group recommends scheduling an appointment approximately 6 months after a first VS, the interval being related to the initial severity of the disease as recommended by the French Rheumatology Society. 6 This provides strict control of the disease as is systematic in the management of numerous chronic diseases (diabetes, rheumatoid arthritis, ankylosing spondylitis, etc.). If the target is not reached, treatment can be intensified and loss of opportunity for the patient is avoided. Moreover, one working group has insisted on this point to optimize the management of knee OA. 42
The practitioners’ responses, based on their clinical experience concerning the expectations, fears, and beliefs of the patients, show that the latter appear rather well informed about VS, with respect to both the expectations (pain relief, improved mobility, fewer pain killers, delaying need for surgery without precluding it) and their concerns (safe treatment). This is probably due to the fact that VS has been used in Europe for more than 25 years with a rapidly growing market expected to be maintained for several years. The result is that most patients know personally or have heard of people who have received this treatment, and are well informed of the methods of administration and benefits and risks of IA injections of HA.
In summary, these new guidelines of the EUROVISCO group, the fifth edition since 2015, 43 aim to help practitioners to make the decision to treat with VS or not, their symptomatic patients naive to treatment with HA injection for their knee OA. They review the basic principles of the decision-making process, based on clinical and imaging findings of knee OA, but also on comorbidities and concomitant medication with the potential to affect treatment efficacy and safety. Finally, they place the patient’s opinion at the core of the therapeutic decision. These new recommendations are in line with and complement those from other working groups published recently.43-45
Footnotes
Author Contributions
All authors participated in the meeting, answered the questions, and discussed all issues. TC analyzed the database.TC and YH wrote the draft of the manuscript. All authors read, commented on, and suggested appropriate changes and then approved the final manuscript.
Acknowledgments and Funding
The authors thank the Laboratoire de Rhumatologie Appliquée (Lyon, France) for organizing and handling all the logistics of the meeting. They thank the HNFC clinical research unit and Charlotte Bourgoin for writing assistance.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
Ethical Approval
This review did not require an ethical board approval because patients were not involved in the design or conduct or reporting or dissemination plans of this research.
Patient Consent for Publication
Not required.