
Abstract
Purpose:
We aimed to compare the movement of the median nerve within the carpal tunnel during wrist and finger motions between before and after carpal tunnel release (CTR) using transverse ultrasound in carpal tunnel syndrome (CTS) patients and to evaluate the biomechanical efficacy of CTR for CTS.
Methods:
Twenty-four patients with CTS were examined by transverse ultrasound. The location of the median nerve within the carpal tunnel was examined quantitatively as a coordinate at varied wrist positions with finger extension and flexion, respectively, before and after CTR.
Results:
We found that the median nerve moved statistically significantly more palmarly after CTR than before at all wrist positions during finger motion. The average median nerve displacement toward the palmar side at the palmar flexion position in finger flexion was the greatest among all positions. Additionally, the displacement amounts of the median nerve during finger motion at all wrist positions were statistically significantly smaller after CTR than before.
Conclusions:
The current study demonstrated the movement patterns of the median nerve in the carpal tunnel during wrist and finger motions compared before and after CTR using transverse ultrasound in CTS patients. The findings suggested that as the median nerve shifted greatly palmarly away from the tendons after CTR, the nerve avoids compression or shearing stress from the tendons. This ultrasound information could offer further understanding of the pathomechanics of CTS and provide a more accurate diagnosis of CTS and better treatment by CTR.
Keywords
Introduction
Carpal tunnel syndrome (CTS) is the most frequent peripheral compression neuropathy of the median nerve in the wrist. Moreover, carpal tunnel release (CTR) is the standard surgical treatment for CTS patients. 1 Despite the high success rate of CTR, the exact pathogenesis of CTS and the biomechanical efficacy of the CTR remain incompletely elucidated.
Recently, several studies using ultrasound have reported that the median nerve and the flexor tendons displaced transversely within the carpal tunnel at varied wrist positions during finger motion in healthy subjects and in patients with CTS. 2 –9 Additionally, some studies using transverse ultrasound have demonstrated that the median nerve moved palmarly in finger flexion and becomes compressed between the flexor tendons and the transverse carpal ligament. 2 –5,7,8 Although examining such median nerve motion may provide useful information about the pathomechanism of CTS, there has been little research comparing the transverse ultrasound displacement of the median nerve within the carpal tunnel at varied wrist positions during finger motion in patients with CTS between before and after CTR. Furthermore, in a previous study, we developed a technique to describe the detailed location of the median nerve as a coordinate within the carpal tunnel in healthy subjects and patients with CTS. 2,3 It is important to examine the location of the median nerve and its displacement amount as a coordinate to further comprehend the precise nerve position within the carpal tunnel during wrist and finger motions.
The purpose of this study was to compare the movement of the median nerve in the carpal tunnel during wrist and finger motions between before and after CTR using transverse ultrasound in patients with CTS. This information may be useful not only in further understanding of the etiology of CTS but also for a more accurate determination of the biomechanical efficacy of CTR for CTS.
Materials and methods
We recruited 24 patients with idiopathic CTS (8 men and 16 women, mean age 68.9 years with a range of 54–93 years) who were clinically diagnosed and confirmed by electrophysiological studies (mean distal motor latency 9.5 ms with a range of 5.25–13.7 ms including 8 patients with electrical silence). In all patients, open CTR with minimal incision was performed. CTS patients were excluded if they reported a history of systemic disease associated with a higher incidence of CTS, such as rheumatoid arthritis, thyroid disease, hemodialysis, amyloidosis, or traumatic injuries to the upper extremities. And, patients with CTS whose wrists were affected bilaterally were also excluded. After signed consent was obtained from all patients in this study, we proceeded with the ultrasound examination on the affected wrist of each patient before and 1 month after CTR.
The ultrasound image acquisition procedure has been described previously. 2,3 Briefly, each patient was seated with the elbow flexed, the forearm supinated, and the shoulder in neutral position. The forearm of the patient was fixed to a custom-made table with the wrist in the neutral position. An ultrasound scanner (Mylab Five; Hitachi Medical Corporation, Tokyo, Japan) provided with an LA332 3.5/12MHz Hi-Definition linear array transducer (LA332) was used. A single orthopedic surgeon performed ultrasound examination in a standardized manner. The transducer was placed at the level of the carpal tunnel with the wrist in the neutral position (Figure 1). A custom-made device with transducer fixed was strapped at the patient’s palm to maintain the transducer stable during examination. In addition, the transducer was kept perpendicular to the surface skin of the wrist regarding a protractor attached to the table to identify both the ridge of the trapezium and the hook of the hamate, without applying additional pressure to minimize compression to the carpal tunnel contents. It is easy to identify these two bony landmarks in all hands. The median nerve, the flexor pollicis longus (FPL), and the flexor digitorum superficialis (FDS) and profundus tendons (FDP) were detected by transverse ultrasound during all-finger flexion and extension.

Ultrasound examination equipment setup. The transducer (T) was fixed in a custom-made fixture during finger motion.
After obtaining a plain image, the transducer was maintained in a custom-made device at each of five study positions (neutral, 60° dorsal flexion, 60° palmar flexion, 40° ulnar deviation, and 10° radial deviation) during finger motion, respectively. Each wrist angle was measured and corrected with a goniometer (SD1-01; Suzukiiryo, Inc., Tokyo) set on the back of the hand at each of the five wrist positions. The patients moved from full extension to maximum flexion of all five fingers as a fist motion at each wrist position continuously and repeatedly. Two cycles of the flexion–extension finger motion were recorded for each wrist position.
All recorded images were examined, and the initial and final frames of the motion for each of the finger extensions and flexions at each wrist position were selected. The median nerve and the flexor tendons were identified in both the extension and the flexion positions of the fingers using these images. The coordinates of the median nerve were determined as follows (Figure 2). The reference point (P) was defined as the midpoint of the distance (A) between the apex of the ridge of the trapezium and the apex of the hook of the hamate. The distances between P and the centroid of the median nerve on the X-axis (X) and on the Y-axis (Y) were measured. The position of the median nerve was defined as a coordinate point (X mm, Y mm). Correcting for individual differences, the ratio (x) of distance (X) to distance (A) and the ratio (y) of distance (Y) to distance (A) were measured and defined as the radial deviation ratio and the dorsal deviation ratio of the median nerve, respectively. The corrected position of the median nerve was shown as a coordinate point (x, y). The radial and dorsal directions were defined as positive and the ulnar and palmar directions as negative. Therefore, the displacement of the nerve in ulnar-radial and palmar-dorsal directions could be calculated by comparing with the coordinates at the initial position of the nerve and the final ones within the carpal tunnel during finger motion.

Measurement of the median nerve location within the carpal tunnel as a coordinate. MN: the median nerve; Tm: the trapezium; HH: the hook of the hamate; FPL: the flexor pollicis longus; FDS: the flexor digitorum superficialis; FDP: the flexor digitorum profundus; distance ‘A’: the distance between the vertex of the ridge of the Tm and the vertex of the HH; point ‘P’: the reference point defined as the midpoint of the distance ‘A’; distance ‘X’: the distance between the point ‘P’ and the centroid of MN on the X-axis; distance ‘Y’: the distance between the point ‘P’ and the centroid of MN on the Y-axis.
All results were expressed as mean ± standard deviation. The averages of the three cycles were calculated. All analyses were performed by SPSS 21.0J. The displacement of the median nerve from the neutral wrist position to the other four wrist positions in full finger extension and flexion was statistically analyzed with the paired t-test. Moreover, the displacement of the median nerve between full finger extension and flexion in each wrist position was statistically analyzed with the paired t-test. Furthermore, the displacement of the median nerve between before and 1 month after CTR in each wrist position was statistically analyzed with the paired t-test, respectively. Additionally, median nerve displacement amounts from full finger extension to full flexion at each of the five wrist positions were statistically compared between before and after CTR with non-paired t-test. A p-value of less than 0.05 was considered to indicate statistical significance for finger and wrist motion differences.
Results
Location of the median nerve at varied wrist positions during finger motion before and after CTR
In the radial-ulnar direction, the median nerve was located statistically significantly (p < 0.05) more radially both at the wrist dorsal flexion ulnar deviation positions than at the wrist neutral position in full finger extension and flexion before and after CTR (Figure 3). The median nerve displacement to the radial side was statistically significantly larger (p < 0.05) at the wrist ulnar deviation position than at the dorsal flexion position. Conversely, the median nerve was located statistically significantly (p < 0.05) more ulnarly both at the wrist palmar flexion and radial deviation positions than at the wrist neutral position in full finger extension and flexion before and after CTR (Figure 3). The median nerve displacement toward the ulnar side was statistically significantly larger (p < 0.05) at the wrist palmar flexion position than at the radial deviation position.

Radial deviation ratio of the median nerve at varied wrist positions with finger motion before and after CTR. CTR: carpal tunnel release.
In the dorsal-palmar direction, the median nerve was located statistically significantly (p < 0.05) more dorsally at the wrist dorsal flexion than it was at the wrist neutral position in full finger extension and flexion before and after CTR (Figure 4). On the other hand, the median nerve was located statistically significantly (p < 0.05) more palmarly at the wrist palmar flexion, ulnar deviation, and radial deviation positions than at the wrist neutral position in full finger extension and flexion before and after CTR (Figure 4). Especially, the median nerve moved statistically significantly (p < 0.05) the most palmarly at the wrist palmar flexion position.

Dorsal deviation ratio of the median nerve at varied wrist positions with finger motion before and after CTR. CTR: carpal tunnel release.
In addition, we examined the median nerve displacement at varied wrist positions during all-finger motion. In the radial-ulnar direction, at the wrist neutral, dorsal flexion, and ulnar deviation positions, the median nerve moved statistically significantly (p < 0.05) more radially in full finger flexion than in full finger extension before and after CTR (Figure 3). On the contrary, at the wrist palmar flexion and radial deviation positions, the median nerve moved statistically significantly (p < 0.05) more ulnarly in full finger flexion than in full finger extension before and after CTR (Figure 3).
In the dorsal-palmar direction, at all wrist positions, the median nerve moved statistically significantly (p < 0.05) more palmarly in full finger flexion than in full finger extension before and after CTR (Figure 4).
Furthermore, we studied the median nerve displacement compared between before and after CTR. In the radial-ulnar direction, at all wrist positions, the median nerve displacement toward the radial side was relatively larger before than after CTR in full finger extension and flexion, but it did not reach significance.
In the dorsal-palmar direction, at all wrist positions in both full finger extension and flexion, the median nerve moved statistically significantly (p < 0.05) more palmarly before than after CTR (Figure 4). Particularly, the median nerve moved greatly palmarly beyond the original position of the transverse carpal ligament at the wrist palmar and ulnar flexion positions after CTR (Figure 4). The average displacement distances toward the palmar side of the median nerve between before and after CTR at the palmar flexion and neutral positions were 1.64 mm, 1.28 mm in full finger extension and 1.50 mm, 1.25 mm in full finger flexion, respectively (Figure 4).
The median nerve displacement amount at varied wrist positions during finger motion compared between before and after CTR
In the radial-ulnar direction, the displacement amounts of the median nerve during finger motion at all wrist positions were statistically significantly smaller (p < 0.05) after CTR than before (Figure 5). Especially, the displacement amount of the median nerve during finger motion at the wrist palmar flexion position was statistically significantly the largest (p < 0.05) among all wrist positions.

Radial displacement amount of the median nerve from finger extension to finger flexion compared between before and after CTR. CTR: carpal tunnel release.
In the dorsal-palmar direction, the displacement amounts of the median nerve during finger motion at all wrist positions were statistically significantly smaller (p < 0.05) after CTR than before (Figure 6).

Dorsal displacement amount of the median nerve from finger extension to finger flexion compared between before and after CTR. CTR: carpal tunnel release.
Concerning the motion of the flexor tendons in full finger flexion at both wrist palmar flexion and radial deviation positions before CTR, the FPL, the FDS, and the FDP moved ulnopalmarly and pushed the nerve toward the transverse carpal ligament. Conversely, the median nerve moved much to the palmar side after CTR. Therefore, the flexor tendons moved freely toward the ulnopalmar side in full finger full flexion without pushing the nerve up to the transverse carpal ligament in the carpal tunnel.
Discussion
The ultrasound examination is generally thought useful to acquire dynamic information about the median nerve and tendon movement during wrist and finger motions in vivo. 2 –9 In recent years, several studies have focused on the median nerve movement in response to active tendon motion within the carpal tunnel during finger or wrist movement using transverse ultrasound. 2 –9 Especially, some researchers reported that in transverse ultrasound examination, the median nerve moved more palmarly or ulnopalmarly in CTS patients than in healthy subjects at the wrist neutral position during finger motion. 5,7,9
Evaluation of the median nerve movement within the carpal tunnel during wrist and finger motion is helpful to understand the pathomechanics of CTS. 3,6,7 In a previous study, we demonstrated the ultrasound technique to evaluate quantitatively the median nerve movement as a coordinate in the carpal tunnel during wrist and finger motion in healthy subjects and patients with CTS. 2,3 Subsequently, we found that at wrist palmar flexion position on the affected side, the median nerve moved statistically significantly the most ulnopalmarly among all wrist positions and became compressed the most strongly against the transverse carpal ligament by the flexor tendons in active finger flexion in patients with CTS. 3
Although CTR has been generally performed for the treatment of CTS, there has been little information detailing the transverse displacement of the median nerve in the carpal tunnel during wrist and finger motions compared between before and after CTR of the same individual in CTS patients by transverse ultrasound.
In magnetic resonance imaging examination, Momose et al. reported that the median nerve and flexor tendons all shifted significantly to the palmar side in CTS patients after CTR. 10 They described that an average palmar displacement of the median nerve 3 months after endoscopic CTR was 1.7 mm, compared with before, which is in line with our study findings. 10 Moreover, Richman et al. reported that an average palmar displacement of carpal canal contents 6 weeks after CTR was 3.5 mm from its original position, and this palmar displacement persisted at the 8-month follow-up. 11 They related that there was a statistically significant 24.2% increase in carpal canal volume after CTR. 11
Both Momose et al. and Richman et al. examined the displacement amount of the median nerve only at the wrist neutral or wrist in 10° of extension position and only in finger extension. However, in our current study, the dynamic displacement patterns of the median nerve within the carpal tunnel were examined at varied wrist positions during finger motion before and after CTR in CTS patients to evaluate the biomechanical effect of CTR. Consequently, our study demonstrated that the median nerve moved statistically significantly more palmarly after CTR than before at all wrist positions during finger motion. Furthermore, the displacement distances of the median nerve at the palmar flexion position were the largest among all the wrist positions. Particularly, the average displacement distances toward the palmar side of the median nerve at the palmar flexion position were 1.64 mm in finger extension and 1.50 mm in flexion, respectively. From these findings, the carpal tunnel was enlarged in the direction of the palmar region after CTR, and sufficient enlargement of space within the carpal tunnel could be confirmed by ultrasound at varied wrist positions. From this finding, it is speculated that as the carpal tunnel widens after CTR, the median nerve shifts greatly palmarly away from the tendons, and the nerve avoids compression or shearing stress from the tendons (Figure 7).
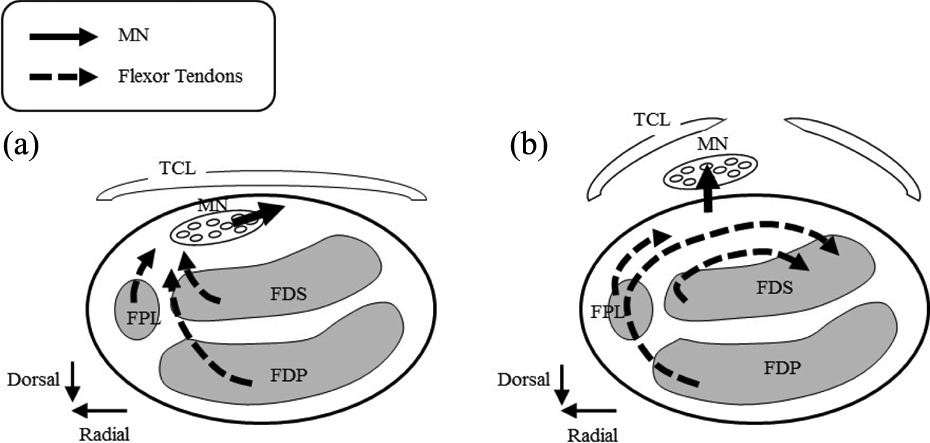
Movement of the median nerve and the flexor tendons in the carpal tunnel (a) before and (b) after CTR. MN: the median nerve; FPL: the flexor pollicis longus; FDS: the flexor digitorum superficialis; FDP: the flexor digitorum profundus; TCL: the transverse carpal ligament; CTR: carpal tunnel release.
In addition, in this study, the displacement amounts of the median nerve in the carpal tunnel from finger extension to flexion at varied wrist positions in CTS patients were compared before and after CTR. In consequence, the displacement amount of the median nerve was statistically significantly smaller 1 month after CTR, compared with before CTR at all wrist positions. Generally, the major characteristic pathological finding in CTS is thought to be noninflammatory fibrosis and thickening of the subsynovial connective tissue, which mediates movement between the nerve and tendons. 12,13 Therefore, these findings suggest that at 1 month after CTR, there still may remain adhesion among the nerve, the tendons, and the transverse carpal ligament due to the fibrosis and thickening of the subsynovial connective tissue, which could reduce the nerve mobility. Moreover, the nerve displacement amount in response to the movement of the flexor tendons would be reduced by the sufficient palmar shift of the median nerve after CTR (Figure 7).
This study has some limitations. First, we investigated a small patient group. A larger group of patients may provide more detailed conclusions to our findings. Second, a weakness of this study was the reproducibility of the ultrasound examination. A single examiner performed all examinations. Therefore, the inter-observer reliability could not be evaluated. However, in the current study, a custom-made transducer fixing device was placed on the patient’s wrist during wrist or finger motion to minimize examiner dependency.
In conclusion, in this study, the movement patterns of the median nerve within the carpal tunnel during wrist and finger motions were compared between before and after CTR using transverse ultrasound in patients with CTS. Additionally, the detailed displacement amounts of the median nerve by a coordinate system were evaluated quantitatively before and after CTR. Subsequently, this study showed that there were significant differences in the median nerve displacement direction and amount in the carpal tunnel between before and after CTR. From the current study, we found that such a median nerve displacement pattern may have the potential to visualize the decompression in CTS and to determine the efficacy of the CTR. This ultrasound information could offer further understanding of the pathomechanics of CTS and provide a more accurate diagnosis of CTS and better treatment by CTR.
Future researches will address examination of the median nerve movement during wrist and finger motion in CTS patients long-term after CTR.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.