
Abstract
Purposes:
To evaluate the feasibility of using the single-joint Hybrid Assistive Limb® robot (HAL) to assist with shoulder flexion-extension in healthy adults, and to assess the capacity of the HAL to analyze the bioelectrical signals of muscle activity for shoulder flexion-extension.
Methods:
This cross-sectional feasibility study included six healthy adult men with no impairment in shoulder motion. The single-joint HAL was fixed to a custom-designed platform and upper arm attachment, and aligned 3 cm below the acromion process. Vital signs, shoulder fatigue, and shoulder pain were evaluated before and after the shoulder elevation exercise performed with and without the HAL. Activity of selected muscles of the shoulder was recorded using a wireless superficial electromyography device. Shoulder movement was captured using a three-dimensional motion analysis system.
Results:
The HAL supported smooth flexion-extension of the arm at the shoulder joint, with no negative effects on vital signs, shoulder fatigue, and shoulder pain. The HAL decreased muscle activity levels, with a 55% decrease in trapezius muscle activity. The upward rotation angle of the scapula was significantly lower with the HAL at 120° of shoulder flexion.
Conclusion:
The single-joint HAL provided safe and effective assistance to scapular plane shoulder flexion-extension among healthy adults.
Introduction
The shoulder complex comprises the glenohumeral and scapulothoracic (shoulder girdle) joints. Stability and mobility at both of these joints are necessary for functional shoulder and upper limb movement. However, due to the complex structure of the shoulder, stability and mobility can be impaired at multiple levels, including bones, joints, ligaments, and muscles, as well as the central and peripheral nervous systems that control the movement of the shoulder. Rehabilitation aims to recover shoulder movement and arm function, and the use of robots has been advocated for the rehabilitation of shoulder movement among stroke survivors. 1 –4 However, as shoulder motion is complex, current robots are limited to providing passive range of motion (ROM) at the shoulder. Therefore, there is a demand for compact devices that would support active movement of the shoulder.
The Hybrid Assistive Limb® robot (HAL) was designed to assist active movement through real-time monitoring of bioelectric signals of the superficial muscles around a joint. The HAL has been effectively used to assist walking in patients with lower limb impairments due to spinal cord or cerebrovascular injury. 5 –11 In addition to assisting with movement, the interactive feedback between the bioelectrical signals, which reflect a patient’s intention to move, and the resultant sensory feedback from movement can improve the functioning of the central and peripheral neural systems for movement.
A single-joint HAL has been constructed to support uniaxial movement at a single joint, such as flexion-extension at the knee or elbow joint. The HAL is very compact and has been successfully used for active ROM support after knee joint replacement surgery. 12 Based on this evidence, the single-joint HAL could facilitate shoulder movement. However, to assist with shoulder flexion-extension, the proximal arm of the robot would need to be affixed to the trunk, which is difficult to achieve reliably. An alternative technique would be to fix the proximal arm of the robot to a platform, with the distal arm of the robot affixed to the upper arm. Therefore, our aim in this study was to evaluate the safety of this novel attachment system for the single-joint HAL at the shoulder in healthy adults. Our second aim was to evaluate the capacity of the single-joint HAL to reliably analyze the complex bioelectrical signals of the muscles of the shoulder that assist with arm elevation. This would establish the validity of using the single-joint HAL for active motion support of shoulder flexion-extension.
Materials and methods
Six healthy adult men, 33.7 ± 1.0-years old, participated in our study. None of our participants was receiving active treatment of a circulatory or respiratory condition at the time of testing. Additionally, none of our participants had a previous history of spinal cord injury, musculoskeletal disorders, or injury/surgery of the shoulder. For analysis, three left shoulders and three right shoulders were randomly evaluated among the six participants. The study was approved by an ethics committee, and all participants provided informed consent.
Setup of the single-joint HAL
Attachments appropriate for the single-joint HAL and platform used were custom designed, with the requirement that all attachments provide firm fixation (Figure 1(a)). To attach the distal portion of the HAL to the upper arm, we used a belt that is currently available with the robot for elbow joint movement (Figure 1(b)). To align the robot at the shoulder, participants were seated on an adjustable chair, with the height and position of the robot adjusted such that the center of rotation of the single-joint HAL was located 3 cm below the acromion, and the longitudinal axis of the HAL was aligned with the center of the shoulder joint. As the HAL will be used in practice with patients with upper limb paralysis, we used a splint to maintain the elbow at a position of 0° of extension for all participants.

Single-joint HAL fixed to a platform. (a) Uniaxial movement, with the center of rotation located at the white circular component. (b) Frontal view, showing the HAL affixed to the upper arm. HAL: Hybrid Assistive Limb® robot.
Shoulder flexion-extension movement through activation of the shoulder muscles
Sensors were positioned on the surface of the anterior fibers of the deltoid to provide the electrical output for shoulder flexion (arm raising), and on the surface of the posterior fibers of the deltoid muscle to provide the electrical output for shoulder extension (arm lowering). Participants were asked to perform a cycle of shoulder flexion and extension through an arc of 120° at a speed of 45 cycles per minute; the timing was ensured by the use of a metronome. By changing the orientation of the trunk relative to the HAL platform, flexion-extension could be performed either in the anatomical or scapular plane of the shoulder (Figure 2(a) to (d)).

Arm raising by 120° in the anatomical and scapular planes. (a) Frontal views of arm raising in the anatomical and (b) scapular planes are shown. (c) Schematic diagram of forward flexion of the shoulder. (d) Schematic diagram of shoulder flexion in the scapular plane.
Anatomical and scapular plane: The anatomical plane of shoulder movement is the sagittal plane, wherein the arm passes through the body front to back. The scapular plane is parallel to the scapular body, which is normally 30° to 45° forward from the frontal plane.
For analysis, participants completed 5 sets of 20 flexion-extension cycles, with a 1-min rest between sets.
Evaluation of safety
Vital signs (blood pressure, heart rate, and blood oxygen saturation) were measured immediately before and after the five sets. Shoulder fatigue and pain were evaluated, before and after the five sets, using a visual analog scale (VAS). Participants were questioned regarding pain, fatigue, and any other adverse symptoms.
Evaluation of validity
To obtain baseline measures of muscle activity and shoulder ROM before the testing session, participants completed 10 cycles of shoulder flexion-extension in the scapular plane through an arc of 0° to 120°, in time with a metronome, and without the HAL. Participants subsequently completed another 10 cycles with the HAL, and muscle activity and shoulder motion were recorded for comparison.
Muscle activity
Muscle activity was recorded from the upper fibers of the trapezius, deltoid muscle, and infraspinatus muscle using a wireless superficial electromyography (EMG) device (Trigno Lab, Delsys, Inc., Natick, Massachusetts, USA). Muscle activity patterns recorded with and without the HAL were compared. EMG data of each muscle of each participant obtained by the device were filtered by a band-pass filter of 40–400 Hz bandwidths and rectified, and an envelope trajectory was computed by a moving-average smoothing filter of a 100-ms window width and then normalized to 0–100%, according to the maximum activation during the shoulder flexion-extension trials without the HAL, using scripts that run on MATLAB 8.2 (MathWorks, Inc., Natick, Massachusetts, USA).
Motion analysis
The scapulohumeral rhythm was recorded using an optical three-dimensional motion analysis device (MX System, Vicon Motion Systems Ltd., Oxford, UK), according to the methods of Yano et al. 13 Surface markers were positioned on the spinous process of C7 and T10, medial margin of the scapular spine, posterolateral margin of the acromion, coracoid process, anterolateral margin of the acromion, and medial and lateral epicondyles of the humerus. Reference axes for the measurement of movement angles were defined as follows: trunk axis, defined by a line from C7 to T10; upper arm axis, defined by a line from the central point between the coracoid process and anterolateral margin of the acromion to the center between the medial and lateral epicondyles of the humerus; and scapular axis, defined by a line from the medial margin of the scapular spine to the posterolateral margin of the acromion. The angles between these axes were calculated (Figure 3). Muscle activity measured by the wireless surface EMG was recorded in synchronization with the motion capture for analysis of muscle activation in accordance with shoulder motion. Among the 10 cycles of shoulder flexion-extension, 8 cycles, excluding the first and last cycles, were detected according to the lower peaks of the upper arm elevation angle. The cycle duration was normalized to 0–100% for each cycle, and the shoulder angles and activation of each muscle were averaged among the cycles.
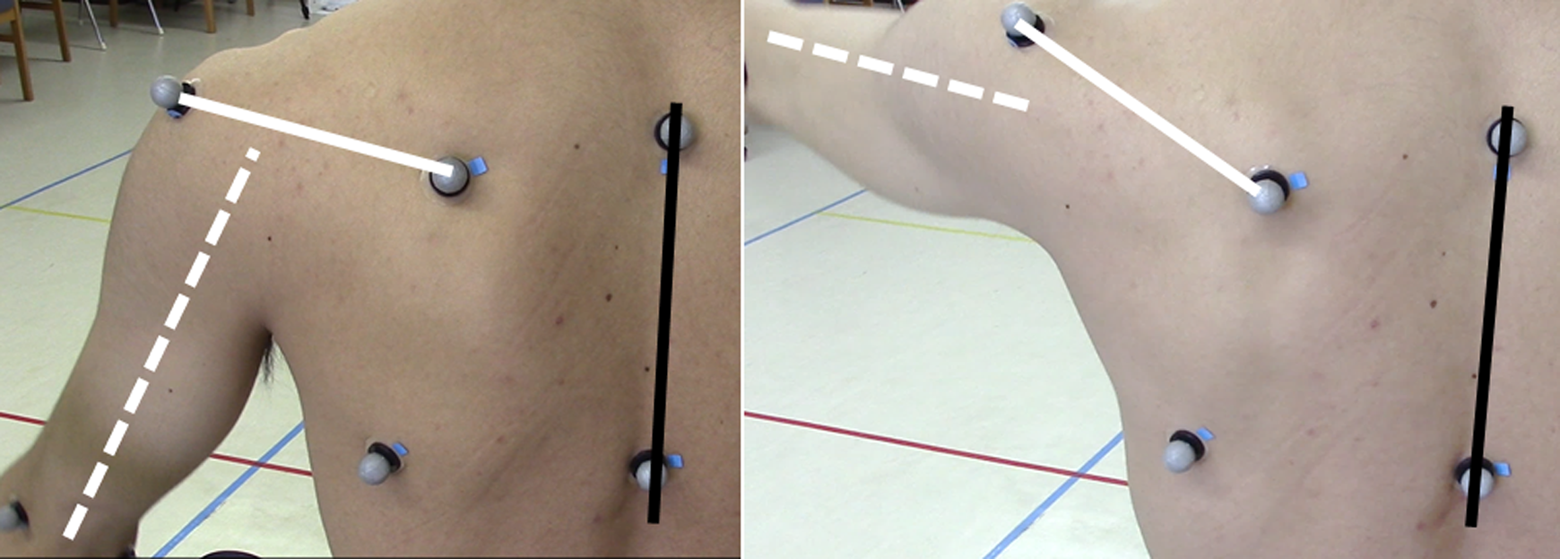
Definitions of axes used for motion analysis. Black line: trunk axis; white broken line: upper arm axis; white solid line: scapular plane axis.
Statistical analysis
Paired t-tests were used to evaluate the difference in joint angle and muscle activity patterns for flexion-extension cycles performed with and without the HAL. Differences with p values <0.05 were considered statistically significant.
Results
Visual inspection of the recorded shoulder movements in the anatomical and scapular planes confirmed that smooth, continuous arm flexion-extension movements could feasibly be achieved with the HAL (video: Online Supplementary).
Safety
Vital signs and VAS scores for pain and fatigue before and after the exercise are reported in Table 1. All measures pretesting and posttesting were comparable. Some participants did report mild fatigue with the use of the HAL, but with no significant difference in VAS scores. One patient developed redness under the electrical output sensor of the HAL with no associated pain or itching. The redness disappeared by the following day.
Mean vital signs and mean VAS pain and fatigue values measured before and after testing.

VAS: visual analog scale; SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate; SpO2: oxygen saturation of peripheral artery; N.s.: not significant.
Validity
Muscle activity profiles of the deltoid, trapezius, and infraspinatus muscles during a single cycle of flexion-extension are shown in Figure 4. The normalized time of the flexion-extension cycle is shown along the x-axis, with the integrated value of muscle activity normalized to a maximum voluntary contraction reported along the y-axis. All muscle activity values were lower for movements performed with than without the HAL (p < 0.05), as follows: a 41% decrease for the anterior fibers of the deltoid, a 55% decrease for the trapezius muscle, and a 32% decrease for the infraspinatus muscle.

Mean muscular activities. The standardized time for a single cycle is shown along the x-axis, and muscle activity levels normalized to a maximum contraction are reported along the y-axis. Solid lines, movement performed with the HAL; broken lines, movement performed without the HAL; blue lines, activity of the deltoid (delt) muscle; green lines, activity of the trapezius (trap) muscle; red lines, activity of the ISP muscle. HAL: Hybrid Assistive Limb® robot; ISP: infraspinatus.
Scapulohumeral rhythm
The upward rotation angle of the scapula for a single cycle for flexion-extension performed with and without the HAL is shown in Figure 5. At the maximum shoulder flexion position of 120°, the upward rotation angle of the scapula was 17.3° for movement assisted by the HAL compared to 24.7° when performed without the HAL (p < 0.05).

Angles of upper arm raising and scapular rotation. The standardized time for a single cycle is shown along the x-axis and the angle of scapular rotation is reported along the y-axis. Solid lines, movement performed with the HAL; broken lines, movement performed without the HAL; blue lines, angle of shoulder flexion; green lines, angle of scapular rotation. HAL: Hybrid Assistive Limb® robot.
Discussion
The single-joint HAL was developed to support movement of the knee and elbow joints. In the present study, we extended the use of the HAL to support flexion-extension movement of the shoulder, including the design of a unique platform to attach the proximal arm of the HAL. In our healthy participants, the use of the HAL did not affect the vital signs, and there was no report of adverse events. Therefore, the HAL was safe and effective to support shoulder flexion-extension. Compared to robots that have previously been used for shoulder rehabilitation, 1 –4 the HAL is compact and simple to use. Moreover, compared to these devices, the HAL was designed to be versatile, providing support for knee and elbow joint movement. Since the HAL uses myoelectric inputs, the assistance it provides reflects a patient’s movement intention. In clinical practice, the effectiveness of a device used in physiotherapy will be markedly impacted by the presence or absence of proprioception. 4 The HAL is distinctive in this aspect, providing meaningful sensory feedback information of movement, which is not available with passive movement.
The significant decrease in activity levels of the muscles of the shoulder is indicative of the support provided by the HAL. Therefore, the HAL would be useful to assist shoulder flexion-extension movement in patients with decreased muscle strength, and it could be effective in reducing reliance on compensatory movements, such as shoulder shrugging during abduction performed in the presence of shoulder abductor weakness. In fact, during assisted flexion-extension movement, the largest decrease in the level of muscle activity (55%) was for the upper fibers of the trapezius, indicating that a compensatory shoulder shrugging is not induced by the use of the HAL.
During shoulder flexion-extension movements, the glenohumeral and scapulothoracic joints move simultaneously, with the coordinated rotational motion of the scapula producing a shift at the center of rotation of the shoulder. Therefore, shoulder flexion-extension is not truly a uniaxial movement. 14 When we fix the single-joint HAL to a platform for shoulder flexion-extension, the resultant movement is uniaxial, with the center of rotation of the robot remaining at a fixed position throughout the movement. Therefore, the flexion-extension movement supported by the HAL is different from the physiological movement, which is reflected in differences in the rotational position of the scapula at the end point of shoulder flexion with and without the HAL. Despite these differences in the location of the center of rotation of the shoulder during flexion-extension, the movement supported by the HAL remained smooth, with no pain reported by participants. Although the HAL does not mimic the physiological motion of the shoulder, it does prevent compensatory motions. In this way, the HAL can prevent pain during movements of shoulder flexion-extension in the same way that passive shoulder movement does not cause pain even though the physiological motion of the shoulder is not reproduced. The association between an altered scapulohumeral rhythm and the occurrence of pain remains to be fully clarified. 15
The use of the HAL to support the shoulder flexion-extension motion in clinical populations remains to be investigated. We recognize that the HAL has the potential to cause pain in patients in whom restriction in shoulder movement is associated with contractures or mechanical pain. Likewise, the patients who have an incision or scar at the proximal humerus from undergoing shoulder surgery can feel pain due to practical contraction of damaged muscles. In these patients, the HAL may not be suitable for shoulder motion assistance. Moreover, future research is needed to evaluate the effects of shoulder muscle weakness and injury to the shoulder on the support provided by the HAL. Similarly, the potential application of the HAL to support movement will need to be evaluated in patients with chronic, large rotator cuff tears who feel less pain but have severe disability of shoulder elevation. Additionally, the patients with altered myoelectric signals of weak muscles due to spinal cord and/or brain injury have an indication for the present motion assistance.
Conclusion
The use of the single-joint HAL fixed to a platform provided safe and effective assistance to shoulder flexion-extension in the scapular plane among healthy adults.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material for this article is available online.