
Abstract
Purpose:
The optimal method for fixation of extra-articular distal humerus factures poses a management dilemma. Although various plate configurations have been proposed, anatomic shaped extra-articular distal humerus locking plates have emerged as a viable solution for these complex injuries. We assessed clinico-radiologic outcome in our retrospective case series of extra-articular distal humerus fractures managed with these plates.
Methods:
Forty-five patients of extra-articular distal humerus fractures, who were operated at our level 1 trauma centre between January, 2012 and December, 2016, were identified. After exclusion, 36 patients were available for the final assessment. All patients were operated with the triceps-reflecting modified posterior approach. Regular clinico-radiologic follow-up was done evaluating elbow functionality, fracture union, secondary displacement, non-union, implant failure and any complications; Mayo Elbow Performance score (MEPS) was used for the final functional assessment.
Results:
Twenty-four (66.7%) male and 12 (33.3%) female patients constituted the study group, who had an average follow-up of 15 months. Preoperatively three patients and post-operatively one patient had radial nerve palsy; all had neurapraxia and recovered completely. Overall, 34 (94.4%) patients were adjudged to have complete radiological union within 3 months; 2 (5.5%) patients developed non-union. Mean flexion achieved was 122.9° ± 23°, and mean extension was −4.03° ± 6.5°; 1 patient with head injury developed flexion deformity of 45°. Average MEPS at the final follow-up was 90.8° ± 9.9°.
Conclusion:
Stable reconstruction and early initiation of physiotherapy are utilitarian to envision optimal outcome; the use of precontoured extra-articular distal humerus locking plates has yielded satisfactory results with minimal complications in our hands.
Introduction
Extra-articular distal humerus fracture accounts for approximately16% of humerus fracture and 3% of all fractures in adults. 1 These fractures are difficult to manage in view of its periarticular location, small size of distal fragment, associated comminution, and moreover, the osteoporotic nature of bone in older individuals. Numerous methods are described for its management, and there are proponents for both conservative and operative intervention. The main goal of treatment is to achieve stable fixation with correct alignment and to allow early range of movement of elbow and shoulder. 2,3 Operative management of these fractures is favoured as it is quite difficult to control and maintain acceptable fracture alignment with the functional brace, and also long duration of immobilization in brace is cumbersome and may lead to elbow stiffness. 4,5
Standard plates available, that is, 4.5 mm dynamic compression plate/locking compression plate (LCP), fail to provide adequate stability in such fracture pattern. 6 –8 Dual plating either in an orthogonal or in a parallel fashion is generally accepted for management of such fracture pattern, as it confers multiple points of fixation into small size distal fragment. This ensures stable fixation, and therefore, allows early range-of-motion (ROM) of the elbow; but its application is fraught with dangers of extensive soft tissue stripping and long operating time, which may risk the development of non-union and infections. 8,9 To minimize the surgical duration and soft tissue devitalization, a single conventional posterolateral distal humerus plate has been proposed for fixation; however, these plates also do not provide adequate stability to allow early range of movement. 5,8,10
The extra-articular distal humerus locking plate (EADHP) is a precontoured, anatomical shaped, angular stable locking plate crafted for extra-articular distal humerus fracture. By even fixing one column of bone, it is purported to provide adequate construct stability, and therefore, can allow early range of movement. We conducted this retrospective study to analyse the functional and radiological outcomes, complication rates and the need of re-operation in the patients with extra-articular distal humerus fracture of distal third of diaphysis and metaphysis managed by EADHP.
Materials and methods
Forty-five patients with extra-articular distal humerus fracture involving distal third of diaphysis and/or metaphysis (AO/OTA type 12A/B/C, and 13A), treated at our level 1 trauma centre between January 2012 and December 2016, were evaluated retrospectively after obtaining ethics clearance. Clinical and radiological data were obtained from hospital charts, patients’ file, office records and hospital’s electronic and radiological database. Exclusion criteria were pathological fractures, associated vascular injury, frank compartment syndrome, age < 15 years and grade II and III open fractures.
Demographics, mechanism of injury, associated injuries, hospitalization details, along with operation description, were collected from the hospital records. Patients with a minimum follow-up of 1 year were called telephonically or by letter for clinical and radiological assessment. Of 45 patients, only 37 patients had met the inclusion criteria, and therefore, included for retrospective evaluation.
All patients with extra-articular distal humerus fracture were evaluated preoperatively for skin condition, associated injuries and neurovascular status. Depending upon the skin condition, U-slab was applied in traction and maintained until operation. All patients were operated in lateral decubitus position under general anaesthesia and/or brachial block; fracture was approached through the midline posterior incision and triceps-reflecting approach. Radial nerve was identified and protected both at lateral intermuscular septum and at spiral groove; status of radial nerve was documented in every case. Triceps was lifted from lateral intermuscular septum and fracture site was exposed. Fracture was reduced under vision and provisionally held with Kirschner’s wire or bone holding clamps; depending upon the fracture configuration, fragments were lagged, whenever appropriate. Appropriate length of plate was chosen and slid under the radial nerve, its proximal end was centred on diaphysis of humerus, and the distal end of the plate was placed over posterolateral aspect of distal humerus just lateral to olecrenon fossa and inferior to it up to the capitellum. Final position was checked under C-arm and fixation done accordingly. Closure was done in layer over romovac drain.
A supervised physiotherapy regime of active assisted and passive exercises was started for all patients from the first post-operative day. All patients were subjected to regular clinical and radiological follow-up in OPD. At the latest follow-up visit, patients were evaluated clinically for ROM, activity level. Radiological assessment was done to look for union of fracture, secondary displacement, non-union, implant failure or any other implant-related complications. Final functional evaluation was done using Mayo Elbow Performance score (MEPS). Range-of-motion of elbow was measured using a goniometer. Union was assessed radiologically; bone was assumed to be united when three cortex unions were seen on orthogonal roentgenograms.
Results
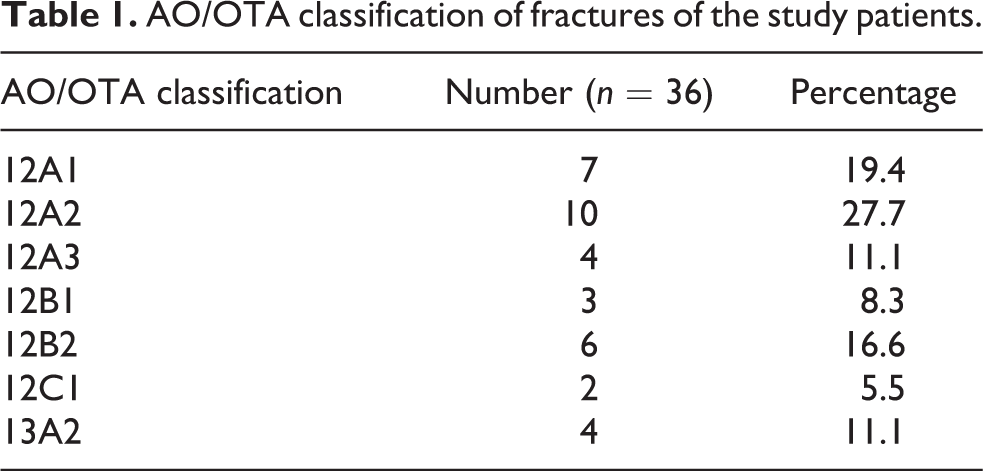
A total of 37 patients were included in the study, of which 1 patient died before fracture union due to medical cause; hence, the final results were calculated for 36 patients. AO/OTA classification of fractures of the study patients is given in Table 1. Average duration of follow-up was 15 months (range 12–36 months). Our study group comprised 24 (66.7%) male and 12 (33.3%) female patients, of which 22 (61.1%) had left limb involvement and 1 patient (2.8%) had bilateral involvement. The average age at the time of surgical procedure was 31.4 (range 16–56) years. Fourteen patients (38.9%) had associated injuries, and two patients had grade 1 open fracture.
AO/OTA classification of fractures of the study patients.
Surgical fixation was performed within a mean delay of 2.3 days from the date of injury utilizing the triceps-reflecting modified posterior approach by EADHP. No intra-operative complications were noted in relation to implant application. Clinical and radiographic data were available for all 36 patients. Three patient (8.3%) had preoperative radial nerve palsy, and post-operatively one patient (2.7%) developed radial nerve palsy; all had neurapraxia and recovered completely within 3 months as evident by nerve conduction tests. Intra-operatively, continuity of radial nerve was found in all patients. Of the 36 patients, 34 patients (94.4%) were adjudged to have complete radiological union within 3 months. Mean flexion achieved was 122.9° ± 23° (range 45–135), and mean extension was −4.03° ± 6.5° (range 0 to −20) (Figure 1). One patient, who developed elbow stiffness and flexion deformity of 45°, had associated head injury. Elbow arthrolysis was performed one and half years after index operation, and final elbow ROM attained was 20–90°. Two patients (5.5%) had non-union; one of them showed breakage of the second proximal locking screw; however, intact plate was providing adequate stability. Even so, they were satisfied with their elbow functionality, resumed their pre-injury occupation with minimal discomfort, and therefore, refused for further operative intervention. Implant prominence over posterolateral aspect of distal humerus was noted in majority of the patients (n = 22), especially in thin built individuals, because of which they complained of pain in that area when their elbow hit some hard object. But only one patient had undergone implant removal so far (Figure 1). Average MEPS at the latest follow-up was 90.8 ± 9.9. No superficial or deep infection was reported. There were no cases of redisplacement of fracture, implant failure or any other implant-related complication in follow-up.
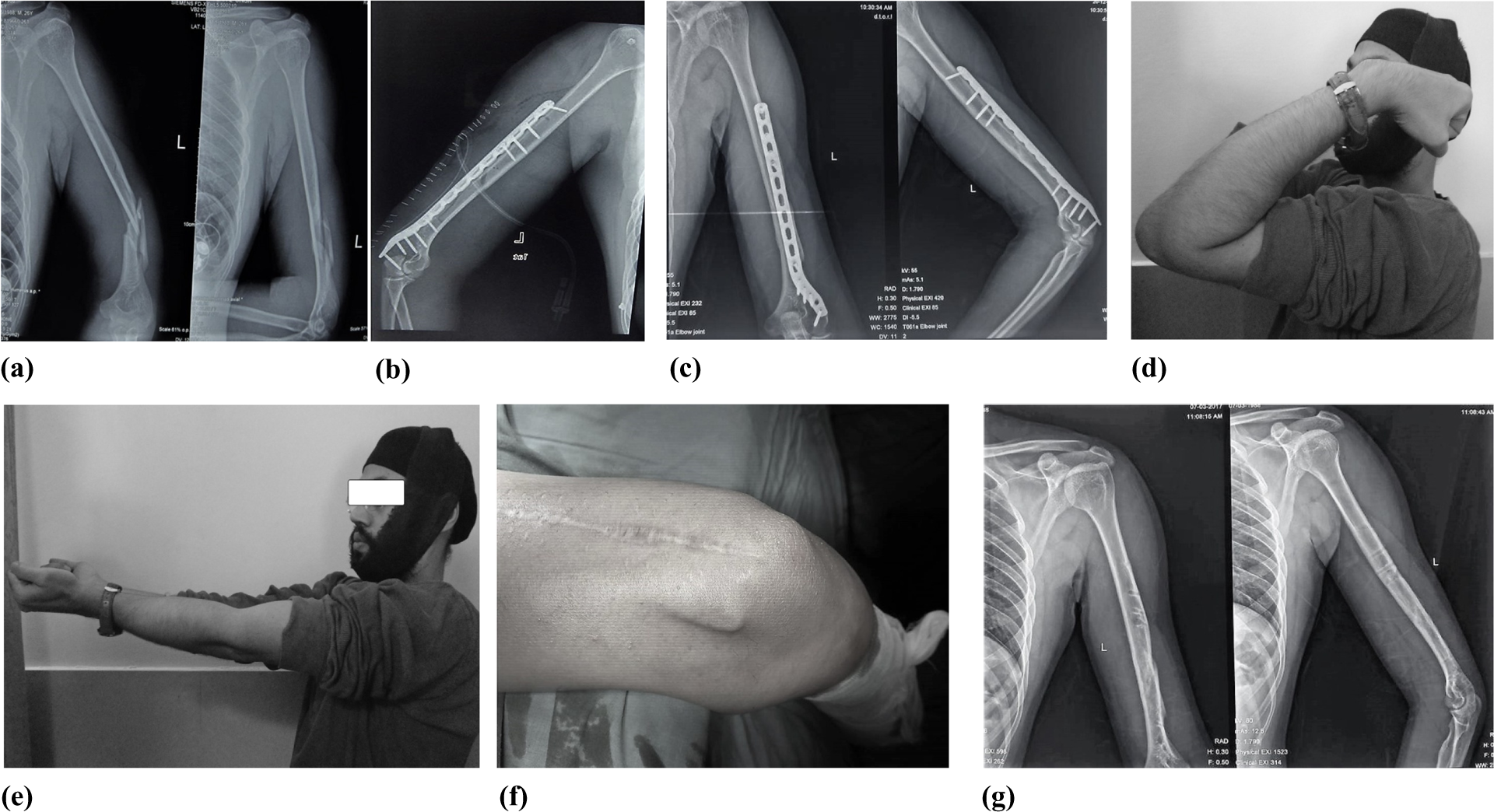
A 26-year-old man sustained extra-articular distal humerus fracture (a) in a road traffic accident. Post-operative radiograph (b) after fixation with EADHP. AP and lateral radiographs (c) 2 years after operation showing complete bony union with satisfactory alignment. Patient had excellent elbow functionality (d and e). This patient requested for implant removal due to untoward prominence of the implant. Clinical photograph showing prominence of implant on posterolateral aspect of distal humerus (f). AP and lateral radiographs (g) after plate removal. EADHP: extra-articular distal humerus locking plate; AP: anteroposterior.
Discussion
Extra-articular distal humerus fractures are difficult injuries and pose management challenge in view of its peri-articular location, associated comminution and small size distal fragment; still there is no definite consensus as to the optimal choice of implant. The goal of treatment is to achieve proper alignment with stable reconstruction so as to commence early elbow ROM. Hence, surgical intervention is favoured over conservative treatment. 8
Small size of distal fragment and strong torsional forces at this junction does not allow optimal stable fixation with the standard plates available. To overcome this difficulty, numbers of modifications in plate designs have been suggested, and some authors have recommended using the plates that are meant for different locations. Levy et al. 11 had used the lateral proximal tibial head buttress locking plate of same side with few modifications to fix these difficult fractures. They reported on 15 patients with good clinico-radiologic outcome without any implant failure, but they argued that this needs elaborate modification in existing designs of plate and in bulk production of the same for general use. Similarly, Spitzer et al. 12 had demonstrated encouraging results with a ‘hybrid’ metaphyseal LCP for proximal or distal metaphyseal humerus fractures and non-unions; it comprised 4.5 mm locking holes at one end and 3.5 mm locking holes at the other end which was postulated to be advantageous to afford increased purchase by virtue of its small calibre screws at short bone fragments. They reported healing of all 21 fractures or non-union at a mean time of 4.5 months without any adverse event of infection or implant failure. Saragaglia et al. 13 developed a ‘Lambda’ plate, which is an inverted Y-shaped plate with a stem and two sectile arms that can be easily remodelled to fit properly according to the type of fracture in distal humerus. However, there is no denying the fact that it is a compression plate without locking holes, which is fraught with risk of inadequate fixation particularly in the presence of comminution and in osteoporotic bone.
We have been using EADHP for treating these difficult fractures since 2012 at our level 1 trauma centre; it is a pre-contoured, anatomical shaped distal humerus metaphyseal plate with lateral curvature to accommodate at least five locking screws in small distal fragment of humerus which ensures rigid fixation in such fracture pattern. Although a dual-plate construct is postulated to confer greater stiffness than single locking plate construct in the presence of severe comminution, 14 a recent in vitro study by Scolaro et al. 15 have concurred favourable biomechanical properties of single precontoured posterolateral extra-articular LCP. This implant was found to have significantly greater bending, torsional and yield strength than standard 3.5 mm LCP for fixation of distal humerus fracture, which was simulated by saw bone osteotomy 80 mm above the trochlea. However, authors were pragmatic in their approach and cautioned that extrapolation of these data to be done carefully, which is because of the fact that this study was done on the saw bone model without taking into account the surrounding soft tissues, which could potentially stabilize or destabilize fracture fragments.
Different approaches have been defined to fix this fracture; the posterior approach being the most common. We have used triceps sparing a modified posterior approach proposed by Gerwin et al. 16 This allows excellent visualization but causes minimum devascularization of bone, spares extensor mechanism to allow early movements, with added advantage of exploration of radial nerve both at lateral intermuscular septum and spiral groove. The main problem with posterior approach, what was observed in our patients was hypertrophic scar, which was not appreciated cosmetically by patients, in 15 (41.6%) of our cases.
Recently, Meloy et al., 17 in a comparative study, contended that single-column plating with precontoured posterolateral locking plate results in comparable union rate and alignment in comparison to dual column plating for extra-articular distal humerus fracture but with significantly fewer complications and better elbow ROM. Favourable results have emanated from our study; union was achieved in 34 patients within 3 months, mean arc of elbow movement was found to be 118.8° ± 24.7°; mean MEPS score was 90.8. Our results fare favourably with other published studies (Table 2). 18 –21 We feel that non-union in our two cases (5.5%) were because of failure to achieve sufficient compression in anterior cortex, which may be partly due to plate configuration. The problem noted during application of plate on flat posterior aspect was offset of plate away from bone in proximal aspect; an attempt to approximate the plate close to the bone with the help of cortical screw leads to anterior opening of fracture site. This phenomenon was particularly noticeable in transverse fracture pattern, which we encountered in our initial two cases that subsequently developed non-union. Zhou et al. 22 in their study showed that mismatch was found between proximal portion of plate to posterior surface of humerus shaft due to the existence of forward flexion angulation of humerus shaft. An attempt to bring the plate close to the bone surface leads to opening of opposite cortex; so pre-bending of plate to approximately 8° between the fourth and fifth dynamic compression portion of combination hole in the distal to proximal direction is recommended, and for an obvious reason, preoperative planning with evaluation of contralateral uninjured humeral anatomy could make it an effective way to combat this potential problem. Learning from our initial experience, we strive to avoid untoward distraction and keep a low threshold for pre-bending the plate whenever deemed necessary.
Brief overview and comparison with other published studies on extra-articular distal humerus fracture fixation.

EADHP: extra-articular distal humerus locking plate; LCP: locking compression plate.
The other problem encountered was the prominence of hardware at lateral aspect of elbow in most of the patients. Thin built patients were more vulnerable, and almost all patients complained of pain on lateral aspect of elbow when they hit by some object. But only one patient asked for removal of implant so far.
We take cognizance of the fact that retrospective nature of the study and lack of control cohort are the potential drawbacks of our study. However, judicious management of extra-articular distal humerus fractures with extra-articular plates has yielded encouraging results in our hands. We reiterate the importance of stable anatomic reconstruction and early initiation of ROM. We suggest to use EADHP in extra-articular distal humerus fracture involving distal third of diaphysis and/or metaphysis. However, surgeons should use a pragmatic approach; judicious preoperative planning is pivotal to choose appropriate implant and thereby optimize the outcome. Patients might need to be counselled about future implant removal due to untoward prominence when using EADHP.
Footnotes
Authors’ note
The content of this article is the original work of the authors. No benefits or funds were received or will be received by any of the authors or their family members in support for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.