
Abstract
Purpose:
Metacarpal bone fractures constitute 10% of all fractures. Unstable metacarpal fractures require surgical intervention, which poses danger to flexor tendon either due to bicortical drilling or construct of the implant. Unicortical locking plate fixation may be the solution to preventing flexor tendon injury. Studies have compared locking and compression plates. However, in these studies, the biomechanical properties were tested using the static loading method. This study looks into cyclical loading that is more representative of in vivo conditions, particularly for early rehabilitation. We compared the biomechanical strength of the unicortical locking plate and bicortical compression plate system in a transverse metacarpal fracture, tested with cyclical loading and torsion.
Method:
Twenty pieces of fourth-generation, biomechanical testing grade, left third metacarpal composite bones were used. Resin was used to create the holding block at both ends of the bone. An oscillating saw with 0.8 mm thick saw blade was used to osteotomize the metacarpal sawbones to create a midshaft transverse metacarpal fracture model. Ten pieces were fixed with a 2.0 mm titanium locking plate via unicortical screw purchase and 10 were fixed with a 2.0 mm, four holes, titanium dynamic compression plate, bicortical purchase of screws. They were subjected to cyclic load to failure testing three-point bending and torsion.
Results:
There were no significant difference in stiffness and cyclic three-point bending to failure between the unicortical locking plate group and the bicortical compression plate group. The bicortical compression plate group is stiffer and has a higher cyclic bending load to failure as compared to the unicortical locking plate group.
Conclusion:
Unicortical locking plate fixation of metacarpal fracture can be reliably applied clinically to produce a strong and stable construct that allows early mobilization of the joints. This will not only reduce the complication rate of metacarpal plating, but also improve the functional outcome of the hand.
Introduction
Metacarpal bone fractures are the commonest fractures involving the upper extremity. 1 The pattern of incidence of metacarpal fractures demonstrates that it does not only cause disability and affect the quality of life of the injured, but also have a negative impact on the socioeconomic aspect as metacarpal fractures most commonly occur in the working age group.
In the treatment of unstable metacarpal fracture, internal fixation is required to maintain the reduction. Plating of the metacarpal fractures is indicated for segmental defects with substance loss, fractures with extreme comminution, and unstable short oblique or transverse diaphyseal fracture. It renders a rigid osteosynthesis while inflicting little to no interference on the surrounding soft tissues when appropriately applied. 2
Hand fractures are as important as other long bone fractures. The final outcome of hand fractures depends on the appropriateness and time of intervention followed by proper rehabilitation. Therefore, the application of the principle of biological, rigid fixation that allows early mobilization is important for a good functional outcome. 3 One of the preferred methods of unstable metacarpal fracture fixation is plating. 4 The capacity of rigid fixation to effect immediate skeletal stability and facilitate early digital motion can considerably enhance recovery. 5
However ideal, it does not come without complications. A retrospective study by Fusetti et al. showed that the common complications of open reduction and plating of extra-articular metacarpal fracture consists of difficulty in fracture healing, stiffness, plate loosening or breakage, and complex regional pain syndrome. 6 Another study demonstrated that 16 of 38 proximal phalangeal and metacarpal fractures treated with plate fixation developed complications of stiffness, malunion, nonunion, and tendon rupture. 7 Page and Stern retrospectively reviewed 82 patients with 105 metacarpal and/or phalangeal fractures stabilized with plates. Major complications were encountered in 36% of fractures, which included stiffness, nonunion, plate prominence, infection, and tendon rupture. 8
Plate prominence, implant failure, infection, tendon adhesion or rupture, joint stiffness, delayed union, malunion, and nonunion remain the main complications post metacarpal and phalangeal plating. Tendon adhesion is a major problem after plating of small bone fractures of the hand. 9 In order to reduce the friction on the extensor tendon, lower profile plates were used and it was demonstrated that such plates are sufficient enough for metacarpal fixation as compared to conventional plates. 10 Other than complication to the extensor tendon, plating of metacarpal can also cause injury to the flexor tendon. This is attributed to the damage caused during bicortical drilling and also friction of the flexor tendon by the prominent screw tip. A case of flexor tendon rupture post plating of the proximal phalanx of the right index finger was reported on the 18th postoperative day, in which range of motion exercises were begun on the second postoperative day. 11
One of the solutions to prevent injury to flexor tendon is by plating the metacarpal with unicortical screw fixation. Many studies have been carried out to compare the biomechanical strength between unicortical and bicortical conventional plating of metacarpal bone fracture. Dona et al. performed a study to compare the biomechanical properties of unicortical and bicortical conventional plating of a midshaft transverse fracture of cadaveric metacarpals using a static load to failure, four-point bending protocol and it was demonstrated that there was no significant difference between both groups. 12 As opposed to the above result, Ochman et al., using a static loading protocol, demonstrated that there was a significant difference between bicortical and unicortical non-locking plate fixation of the metacarpal fracture, in which the bicortical group had higher load to failure. 13 A study by Afshar et al. also showed that there was a significant difference between the groups where the bicortical group demonstrated higher mean load to failure. 14 The latter study used a cyclic loading protocol, which is more representative of the biological conditions of humans, particularly in the clinical aspect of encouraging early joint motion during rehabilitation post fixation of hand fracture. Both studies showed that plating of the metacarpal fracture using a conventional plate in a unicortical pattern does not produce a strong and stable fixation as compared to a bicortical pattern to allow early range of motion.
Fracture fixation is evolving to the usage of locking plates. Due to the locking mechanism of the screwhead to the plate holes, it provides a more mechanically stable and rigid construct. Therefore, unicortical locking plate can be a better solution in producing a stronger and stable fixation, which allows early joint motion, in addition to reducing the complications of flexor tendon injury. In order to prove its stability, studies were carried out to compare its biomechanical strength to bicortical fixation of non-locking plates. Gajendran et al. demonstrated that there was no significant difference between unicortical locking and bicortical non-locking fixation of a double-row 3-dimensional plate, with an equivalent load to failure value. 15 A study by Mudrick et al. showed that there was no significant difference between unicortical locking plate and bicortical non-locking plate in a midshaft fracture of porcine metacarpal, with the unicortical locking plate group demonstrating higher load to failure. 16 Similar results were also demonstrated by Ochman et al., in which the unicortical locking plate fixation and bicortical non-locking plate fixation of a midshaft metacarpal fracture model showed no significant difference, with the unicortical locking plate group demonstrating higher load to failure. 13 However, the above studies were done using the static loading protocol. As previously mentioned, the cyclic loading protocol is more representative biologically in relation to the forces acting on the fixation construct during early range of motion exercise. Therefore, a biomechanical study comparing unicortical locking plate fixation and bicortical non-locking compression plate fixation was carried out on transverse midshaft metacarpal fracture model using a cyclic loading regime to have a more clinically relevant result.
Materials and methods
In this study, 20 pieces of fourth-generation, biomechanical testing grade, left third metacarpal composite bones (sawbones; Pacific Research Laboratories, Vashon, Washington, USA) were used. Fourth-generation composite bones have mechanical behavior that falls within the range for cadaveric specimens and simulate the physical behavior of human bones. Composite bones are more reliable in mechanical testing as they have lower variability in testing as compared to cadaveric specimens. Several studies have used composite bones to test the biomechanical properties of metacarpal fracture fixation. 15,17,18 Figure 1 shows a sample of the fourth-generation, left third metacarpal composite sawbones and Table 1 shows the dimensions. Ten pieces of each respective plate were used, as shown in Figure 2(a) and (b).

(a) to (c) Side, dorsal, and oblique view of the fourth-generation, left third metacarpal composite sawbones.
Dimension of the fourth-generation, left third metacarpal composite sawbones.


(a) Synthes 2.0 mm, four holes, titanium LCP and 2.0 × 8.0 mm self-tapping titanium locking screw. (b) Synthes 2.0 mm, four holes, titanium DCP and 2.0 × 14.0 mm self-tapping titanium cortical screw. LCP: locking compression plate; DCP: dynamic compression plate.
Resin and its hardener were used to create the holding block at both ends of the metacarpal composite sawbones. Two cube-shaped metal jigs were used as the molding block for the resin (Figure 3(a) to (c)). One 10 cc syringe was used to withdraw the appropriate amount of resin needed and one 1 cc syringe was used to withdraw the appropriate amount of hardener needed to mix into the resin. A plastic container and a wooden spatula were used to mix the resin and its hardener before pouring it into the molding jig. Grease spray was used to apply grease over the inner aspect of the cube-shaped metal jig for easy removal of the hardened resin around both ends of the metacarpal sawbones. Final product is shown in Figure 3(d) and (e).
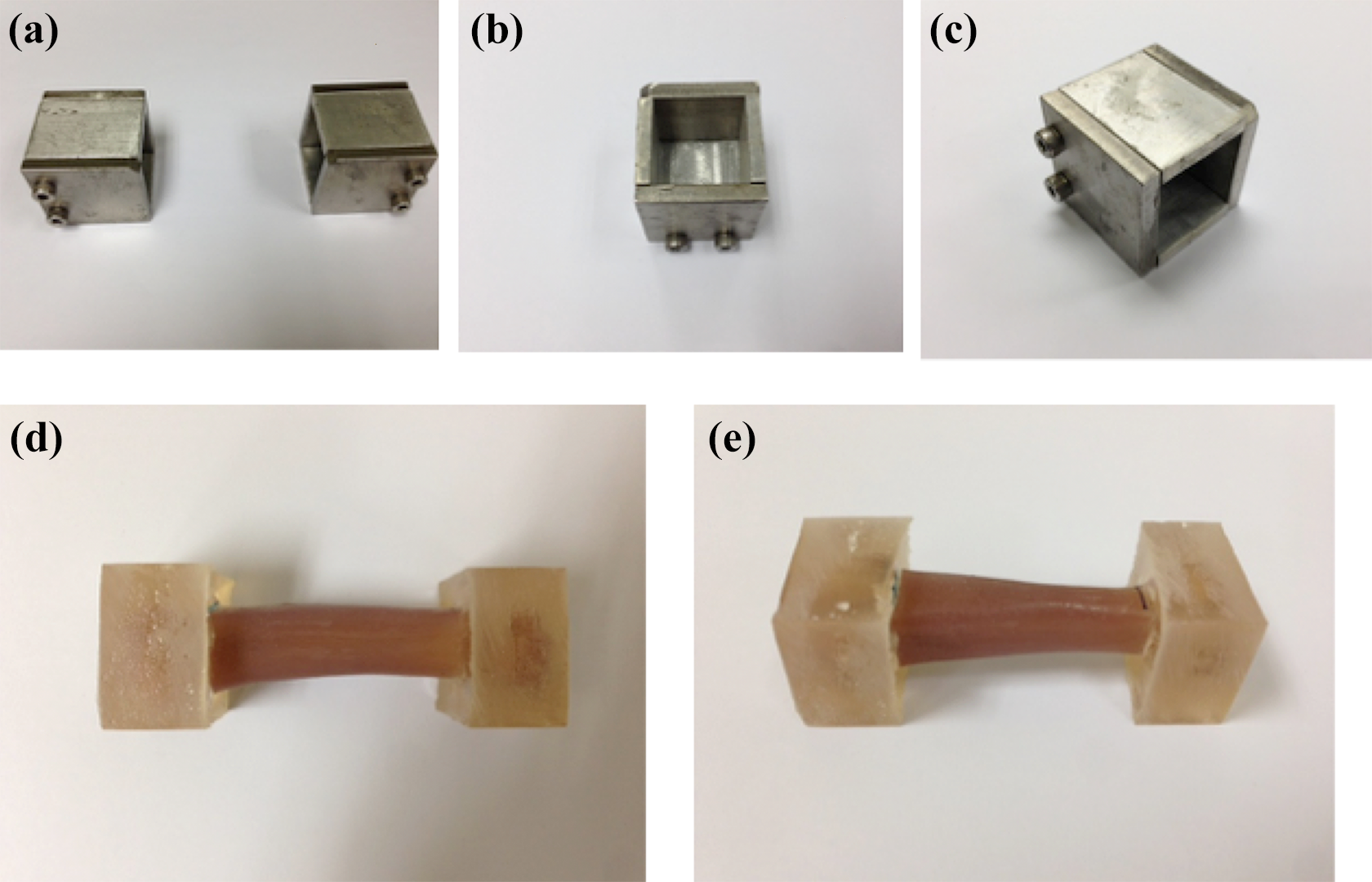
(a) to (c) Different views of the cube-shaped metal jigs that were used as the molding block for the resin and also acting as the holding jig for cyclic torsion test. (d) and (e) Third metacarpal composite sawbones fixed with resin at both ends with a load span of 40 mm.
An oscillating saw with 0.8 mm thick saw blade was used to osteotomize the metacarpal sawbones to create a midshaft transverse metacarpal fracture model (Figure 4(a)). A 1.5 mm drill bit fixed to a handheld, cordless drill was used to create screw holes. A threaded drill guide was used while drilling the screw holes for the locking screws and a universal 1.5 mm drill sleeve was used while drilling the screw holes for the cortical screws. A star-drive screwdriver was used to insert the screws into the screw holes, with an additional torque-limiting device used for the insertion of locking screws (Figure 4(b)). A Synthes 2.0 mm, four holes, titanium locking compression plate was used. The other group of metacarpals was reduced and fixed with a Synthes 2.0 mm, four holes, titanium dynamic compression plate. The plate was pre-bent to ensure the far cortex of the metacarpal was compressed. Screw holes were drilled bicortically using a 1.5 mm drill bit together with a universal drill sleeve for all four holes. Self-tapping cortical screws of 2.0 mm, measuring 14 mm in length were inserted bicortically into all four holes (Figure 4(c) and (d)).
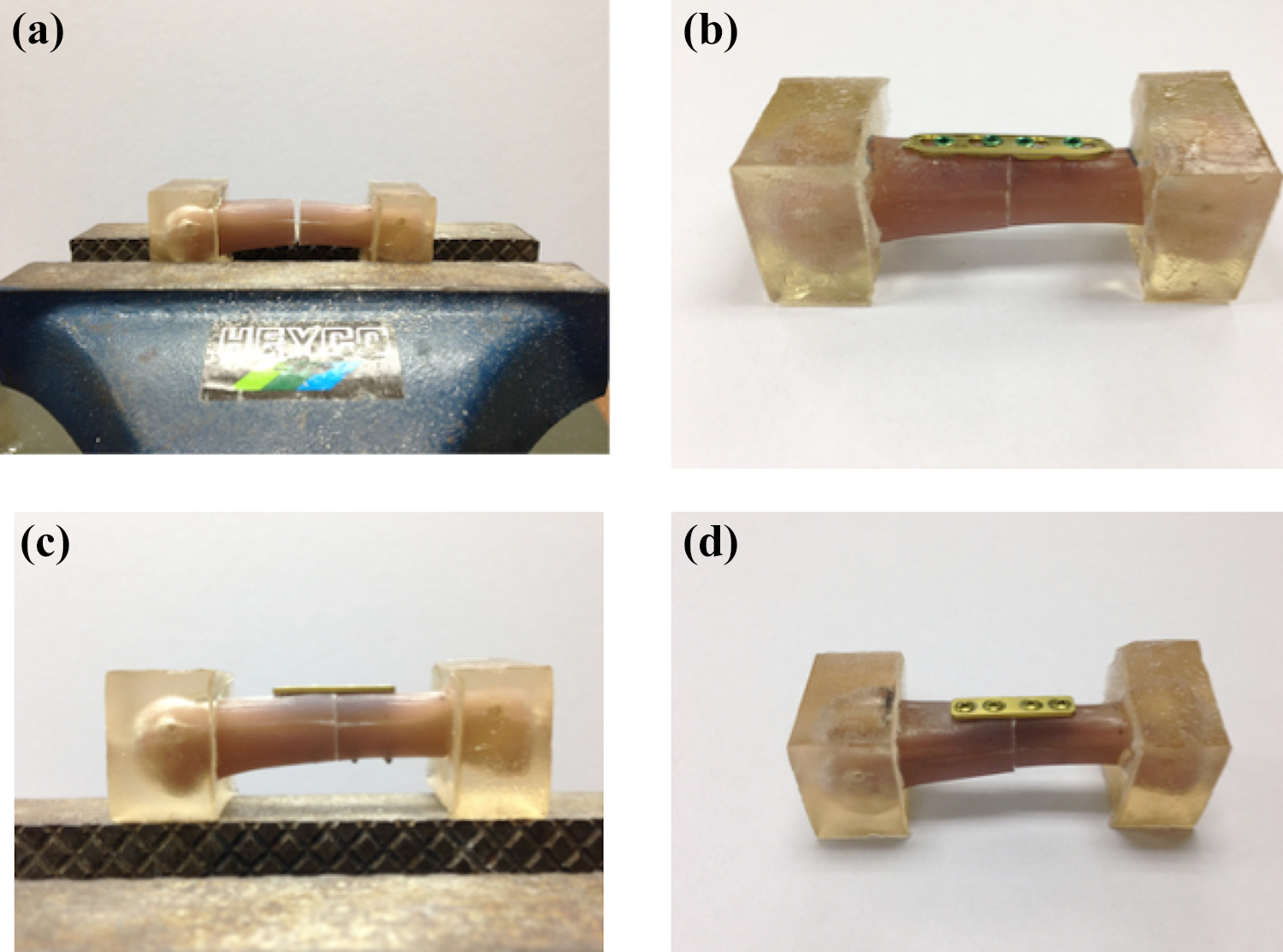
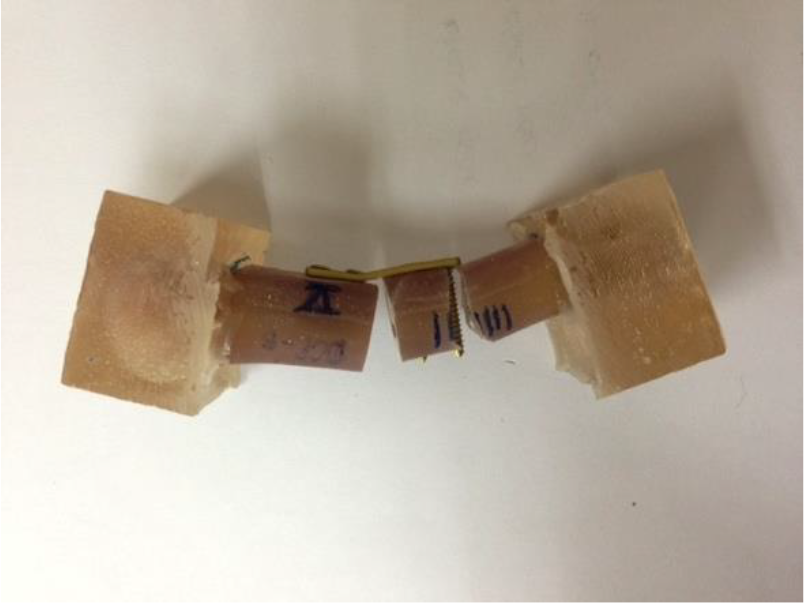
(a) Transverse fracture. (b) Transverse midshaft metacarpal fracture model plated with Synthes 2.0 mm, four holes LCP with the locking screws inserted unicortically. (c) and (d) Transverse midshaft metacarpal fracture model plated with Synthes 2.0 mm, four holes DCP with the cortical screws inserted bicortically. LCP: locking compression plate; DCP: dynamic compression plate.
The cyclic load to failure test was done using Instron Microtester 5848 (Instron, Norwood, Massachusetts, USA) machine.
Cyclic three-point bending protocol
Cyclic three-point bending, a holding jig that is compatible with the size and shape of the resin block was used to hold the specimen and a metal indenter was used to create the bending force over the volar aspect of the plated, fractured metacarpal model (Figure 5(a)). A preload of 1 N was applied at the beginning of each cycle to ensure that the metacarpals remained in place throughout the test. A sine wave–shaped load was applied and the test was done under load control using a 2 kN load cell. At the beginning of the cyclic loading protocol, a trapezoidal load of 50 N was created to assess the stiffness of the construct. The cyclic loading was then started with a load of 100 N for the first block followed by an increment of 100 N for each block of cycles, with each block consisting of 20 cycles. A 10-s rest was applied after each cyclic block. The test was conducted at a rate of 0.5 Hz and was performed until the fixation failed with a sudden drop in the resisted load. Modes of failure were based on three main observations: cortical fracture at the shaft (mode I), screw cutout from the shaft and implant loosening (mode II), and plate bending (mode III).
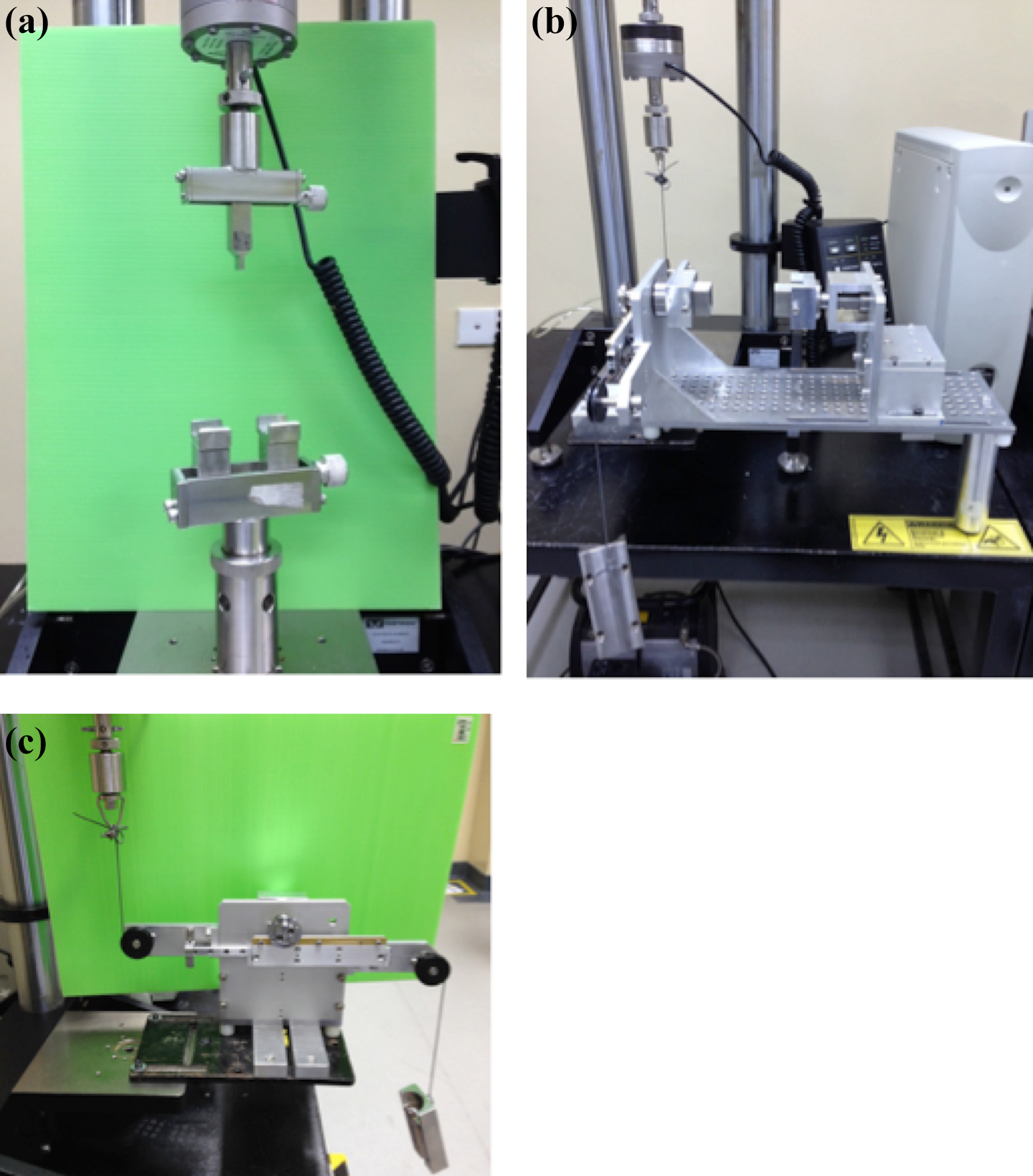
(a) Metal indenter and holding jig for the specimens used in cyclic three-point bending test. (b) Torsion jig with the cogwheel system on the left side and the fixed end on the right side. (c) The cogwheel system of the torsion jig; on the left side it was connected to the Instron Microtester 5848, while on the right side it was connected to a balancing load hanging freely. This is to ensure the system returns to normal position during cyclic torsional loading.
The transverse bending load was applied using an indenter at the fracture site over the volar aspect of the metacarpals, which simulated the compression forces over the volar aspect and tensile forces over the dorsal aspect of the metacarpals during flexion of the fingers. The test for each specimen was recorded down using a video recorder and reviewed back to ensure that no errors occurred. The measured value was rounded to the nearest 0.01 N/mm for stiffness and 0.01 N for cyclic load to failure and load for plastic deformation.
Cyclic torsional loading protocol
For the torsion test, a modified jig using a cogwheel system was used, with one end connected to the Instron machine and the other end connected to a balancing load to ensure the whole system returns to its normal position during cyclic torsional loading, particularly when the bone–plate construct is still within the elastic zone biomechanically (Figure 5(b) and (c)). A sine wave–shaped load was applied and it was done under load control using a 1 kN load cell. At the beginning of the cyclic loading protocol, a trapezoidal load was created to assess the torsional stiffness of the construct. The cyclic torsional loading was then started with a load of 10 N for the first block followed by an increment of 10 N for each block of cycles, with each block consisting of 20 cycles. A 10-s rest was applied after each cyclic block. The test was conducted at a rate of 0.25 Hz and was performed until the fixation failed. Failure was defined as rotational deformity of 5 degrees or more, in which the extension was at 1.08 mm or more. The torsional stiffness value was rounded up to the nearest 0.01 N/mm, while the cyclic torsional load to failure was rounded up to 0.01 N.
Results
Bending stiffness
The unicortical locking plate group had a mean bending stiffness (Figure 6) value of 257.37 N/mm (standard deviation (SD) 81.12), with the highest value of 364.85 N/mm and the lowest value of 166.32 N/mm. The bicortical compression plate group had a mean bending stiffness of 326.06 N/mm (SD 55.71), with the highest value of 382.37 N/mm and the lowest value of 252.30 N/mm. The bending stiffness between the unicortical locking plate group and the bicortical compression plate group was not significantly different (p = 0.21, using paired t test).

Bending stiffness of the unicortical locking plate group and the bicortical compression plate group. LCP: locking compression plate; DCP: dynamic compression plate.
Cyclic loading to failure: Three-point bending
The highest load to failure achieved during cyclic loading (Table 2) of the unicortical locking plate construct was 1000 N, with a mean value of 940 N (SD 54.77). The highest cyclic load to failure in the bicortical compression plate construct was 1300 N with a mean value of 1100 N (SD 158.11). Both groups had the same lowest load to failure, which was 900 N. There was no significant difference between both groups (p = 0.06, using paired t test).
Cyclic three-point bending to failure of unicortical LCP versus bicortical DCP.

LCP: locking compression plate; DCP: dynamic compression plate; SD: standard deviation.
The highest number of cycles to failure (Table 3) in the unicortical locking plate system was 186 cycles, while the bicortical compression plate system was 250 cycles. The mean value of cycles to failure in the unicortical locking plate group and the bicortical compression plate group was 174.20 cycles (SD 9.73) and 203.40 cycles (SD 34.41), respectively, and both were not significantly different (p = 0.10).
Number of cycles to failure in cyclic three-point bending protocol of unicortical LCP versus bicortical DCP.

LCP: locking compression plate; DCP: dynamic compression plate; SD: standard deviation.
Plastic deformation
The highest load of plastic deformation (Figure 7) in the unicortical locking plate group was 600 N, whereas the lowest was 400 N. The unicortical locking plate group had a mean value of 520 N (SD 83.67). In the bicortical compression plate group, the highest plastic deformation load was 900 N and the lowest was 400 N, with a mean value of 600 N (SD 212.13). There was no significant difference between both groups (p = 0.54, using paired t test).

Plastic deformation of unicortical LCP versus bicortical DCP. LCP: locking compression plate; DCP: dynamic compression plate.
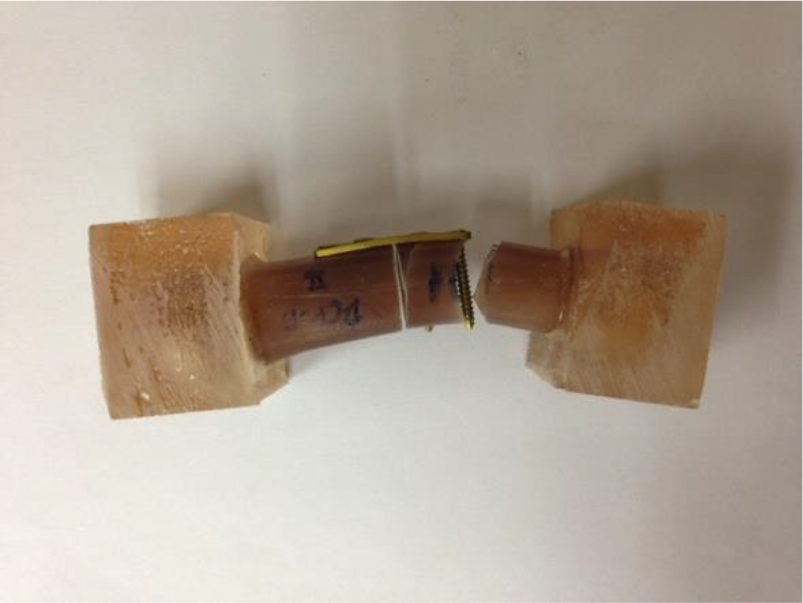
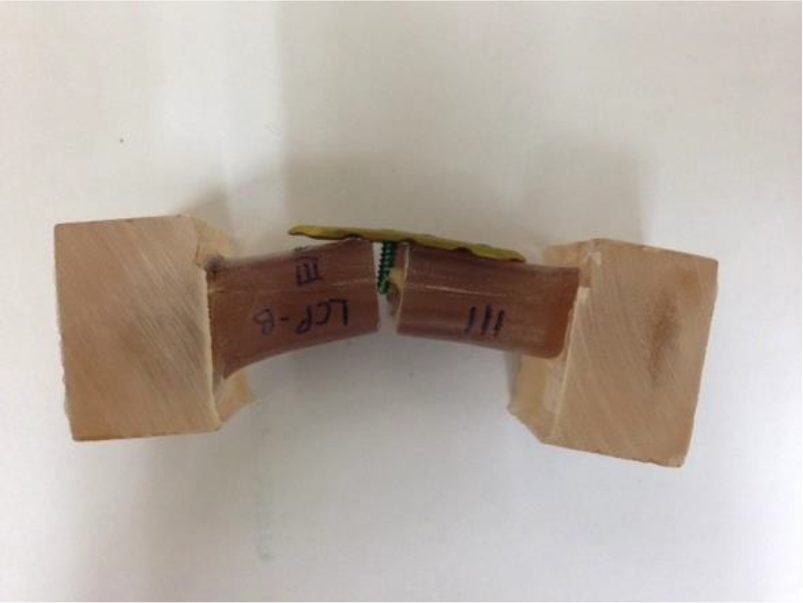
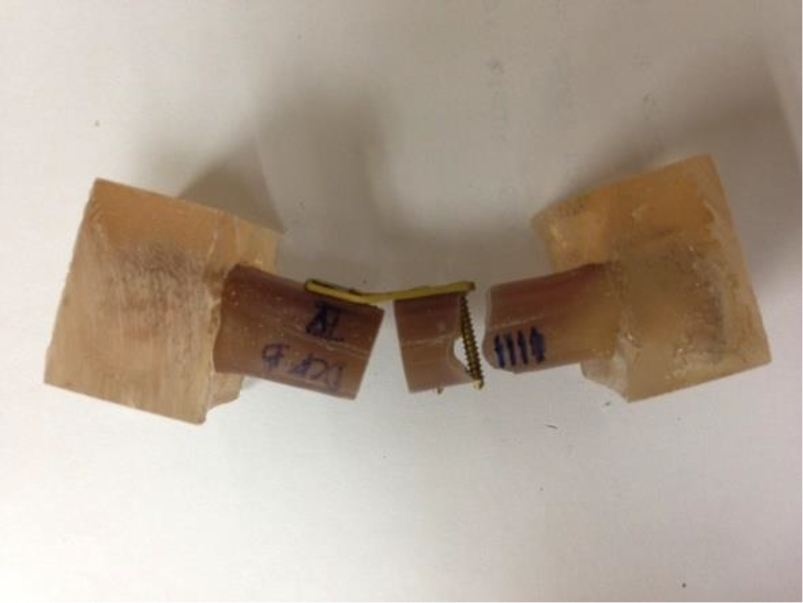
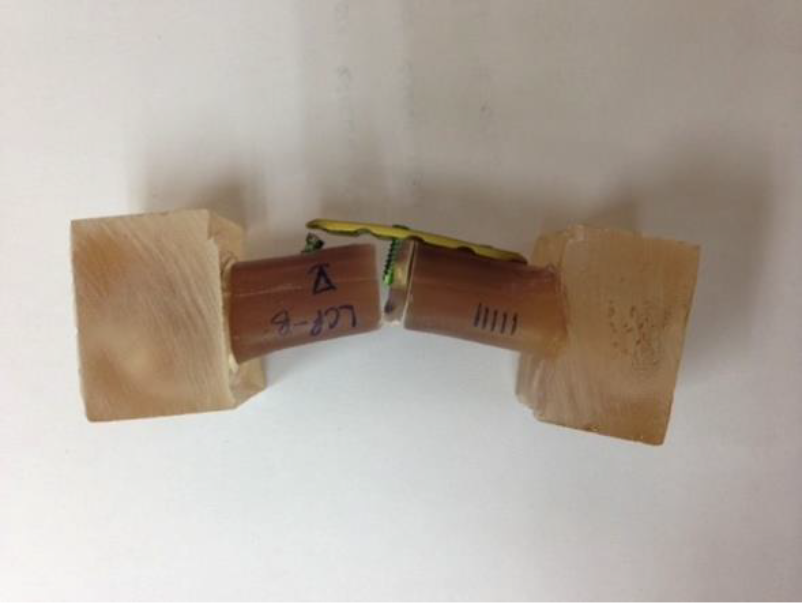
Mode to failure
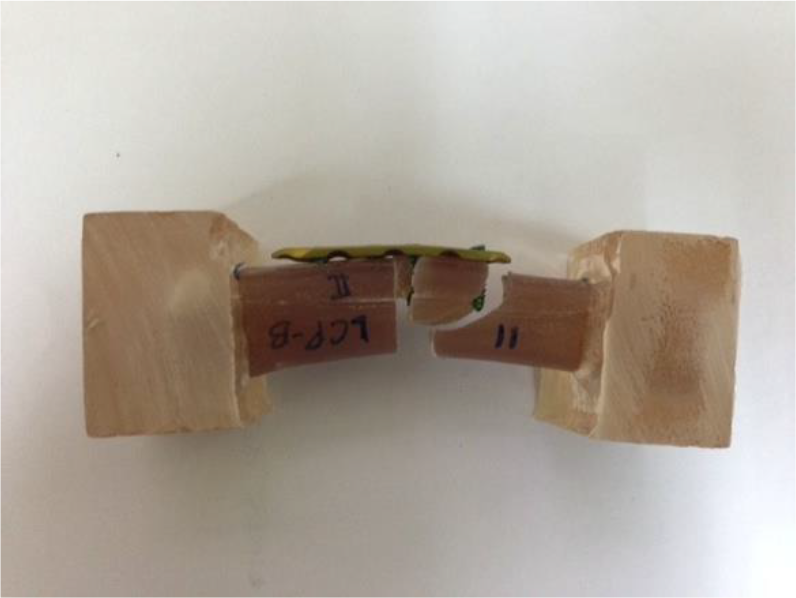
Only one mode of failure was identified in both groups of constructs. In the unicortical locking plate group, all five samples failed by a cortical shaft fracture at the screw–bone interface (mode I). Three of the five samples fractured at the screw–bone interface at the proximal end of the construct, which is the stress riser site. An interesting finding was noted in the other two samples, in which the construct failed by fracture at the inner screw of the distal segment. At the same time, the outer screw at the distal segment had breakage and bending at the head–shaft junction. In addition, both of the screwheads were noted to be disengaged from the threaded hole of the locking plate. All five samples in the bicortical compression plate group failed by the cortical shaft fracture at the screw–bone interface (mode I) at proximal end of construct. Both groups of constructs were not associated with any screw cutout or plate bending (Table 4).
Mode of failure between the unicortical locking plate group and the bicortical compression plate group for all five samples submitted to cyclic three-point bending protocol.





Torsional stiffness
In the unicortical locking plate group, the mean torsional stiffness was 37.77 N/mm (SD 6.14), with the highest value of 42.56 N/mm and the lowest value of 27.23 N/mm. In the bicortical compression plate group, the mean torsional stiffness was 26.44 N/mm (SD 6.78), with the highest value of 35.79 N/mm and the lowest value of 20.29 N/mm. Both groups demonstrated a significant difference with a p value of 0.037 (p < 0.05, using paired t test; Table 5).
Torsional stiffness of unicortical LCP versus bicortical DCP.

LCP: locking compression plate; DCP: dynamic compression plate; SD: standard deviation.
Cyclic torsional load to failure
In the unicortical locking plate group, the mean cyclic torsional load to failure was 174 N (SD 18.17). In the bicortical compression plate group, the mean cyclic torsional load to failure was 116 N (SD 8.94). The highest cyclic torsional load to failure achieved in the unicortical locking plate group and the bicortical compression plate group was 200 N and 130 N, respectively. Both groups demonstrated a significant difference statistically, with a p value of 0.002 (p < 0.05, using paired t test; Table 6).
Cyclic torsional load to failure of unicortical LCP versus bicortical DCP.

LCP: locking compression plate; DCP: dynamic compression plate; SD: standard deviation.
Discussion
There are various methods that are applicable in the fixation of metacarpal bone fractures, which includes K-wiring, tension band wiring, lag screw, and plating. In order to achieve a stable and strong fixation that prevents malalignment and allows early mobilization, plating is fixation of choice in providing a stable fixation as compared to other methods. 19 Xu and Zhang demonstrated that mini-plate is superior to K-wire in the fixation of the metacarpal fracture. 20
Doht et al. conducted a biomechanical test comparing non-locking and locking plates in mono- or bicortical screw fixation of the metacarpal fracture model by cyclic loading for 1000 cycles using only 20% of the maximum load of the original bone, with a value ranging from 101 to 119 N, followed by observation of differential displacement of the construct. 21 There was no significant difference between the monocortical screw fixation of the locking plate and bicortical screw fixation of the non-locking plate. It was demonstrated that both have similar displacement, maximum load to failure, and stiffness. However, in our study, a different cyclic loading regime was utilized. The test subjects were loaded initially with 100 N for 10 cycles followed by an increment of 100 N for each subsequent cycle with 10-s rests in between, until the construct failed. In our opinion, this regime closely simulates the variable forces that act on the human hand bone during rehabilitation such as range of motion and gripping exercises. A study by An et al. demonstrated that the bending moment at the midshaft of the index finger metacarpal during grasp ranges from approximately 5.6 to 20.9 Nm. 22 This will amount to about 174–652 N of force acting on the distal end of the metacarpal from the midpoint. An assessment on the strength of grip by Swanson et al. showed that the male group has grip strength ranging from 30.4 to 70.4 kg (approximately 298–690 N) and the female group has grip strength ranging from 14.0 to 38.6 kg (approximately 137–379 N). 23
The results of our study demonstrated that there were no significant differences in stiffness and cyclic three-point bending to failure between the unicortical locking plate group and the bicortical compression plate group. The bicortical compression plate group is stiffer and has a higher cyclic bending load to failure as compared to the unicortical locking plate group. The relative thicker palmar cortex of the metacarpal bone as compared to the dorsal cortex 24 may explain the more superior pullout strength of the bicortical compression plate group, contributed by the engagement of the screw into the far, palmar cortex.
In the unicortical locking plate group, three of the specimens failed by the cortical shaft fracture at the proximal end stress riser site at the screw–bone interface, which is similar to the bicortical compression plate group. This suggests that both groups of constructs produce similar strength and stability. The other two specimens of the unicortical locking plate group fractured at the screw–bone interface at the inner screw of the distal segment with associated failure of the outer screw at the neck–shaft junction, which is the weakest point of the screw. No screw cutout or plate bending was noted. This shows that the locking screw demonstrates good pullout strength and thus is able to produce a relatively strong and stable fixation, even though the locking screws were inserted unicortically, as compared to the bicortical compression plate group.
Conclusion
Unicortical locking plate fixation for the metacarpal fracture provides a stable fixation, which is comparable to conventional compression plate but it does not imply that the principle of compression be replaced. In cases where you may not be able to achieve interfragmentary compression, a unicortical locking plate construct would offer comparable fixation strength to a standard compression plate construct and protect the volar structures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.