
Abstract
Atypical femoral fractures (AFFs) are recently observed as a complication of long-term bone-modifying agent (BMA; bisphosphonate or denosumab) therapy for bone metastases. We describe the cases of two women diagnosed with breast cancer who developed incomplete AFF associated with BMAs prescribed for bone metastases. Radiographs of their femurs revealed thickening of the lateral subtrochanteric cortex, and tomosynthesis revealed a visible fracture line in the thickened cortex. They were initially treated with conservative management; however, the incomplete fracture resulted in a complete fracture. These cases highlight two major implications. First, symptomatic incomplete AFF associated with BMAs prescribed for bone metastases should be treated with surgical prophylaxis, given the fact that fracture healing is expected to require a longer duration and an incomplete fracture might potentially progress to a complete fracture during long-term conservative management. Second, tomosynthesis is useful in identifying radiolucent fracture lines that are reliable predictors of fracture propagation.
Keywords
Introduction
In the past decade, atypical femoral fracture (AFF) has emerged as a potential complication of bisphosphonates (BPs). Denosumab is a fully human monoclonal antibody against receptor activator of nuclear factor-κB ligand (RANKL) and is increasingly considered as an alternative to BPs. Importantly, a few cases of patients treated with denosumab who developed AFFs were recently reported. 1 Bone-modifying agent (BMA; BP or denosumab) has been used not only to treat osteoporosis but also to reduce the frequency and severity of skeletal-related events (SREs) in patients with bone metastases. We herein present two patients who developed AFFs while receiving BMA therapy for bone metastasis due to breast cancer.
Case reports
Patient 1
The study patient is a 52-year-old woman who had undergone lumpectomy at the age of 36 when she was diagnosed with breast cancer. She had no comorbidity. Three years after the lumpectomy, she was found to have systemic bone metastases, and intravenous BP was administered for 11 years until a switch to denosumab was made. BPs included pamidronate at a monthly dose of 45 mg for the first 6 years and 10 months followed by zoledronate at a monthly dose of 4 mg for 4 years and 4 months. Several courses of chemotherapy were administered during BP therapy, specifically goserelin, anastrozole, tamoxifen, letrozole, capecitabine, trastuzumab, fulvestrant, and paclitaxel. However, multiple bone metastases were found to gradually spread to the vertebrae, pelvis, both proximal femoral shafts, and so on. Radiation therapy targeted at the lumbar vertebrae and pelvis was performed. Because metastatic lesions in both femoral shafts were osteosclerotic and painless, radiation therapy was not required for these femoral lesions.
The patient was administered with denosumab injections at a monthly dose of 120 mg for 2 years and 3 months when she presented with mild pain in her right thigh without any trauma. Radiographs of her right femur showed thickening of the lateral subtrochanteric cortex. Tomosynthesis revealed a visible fracture line in the thickened cortex, which was not detected with conventional radiography (Figure 1); therefore, she was diagnosed with incomplete AFF and denosumab was discontinued. The patient was initially managed conservatively for incomplete AFF. However, she fell down from a standing position and was transferred to our hospital 1 month later.
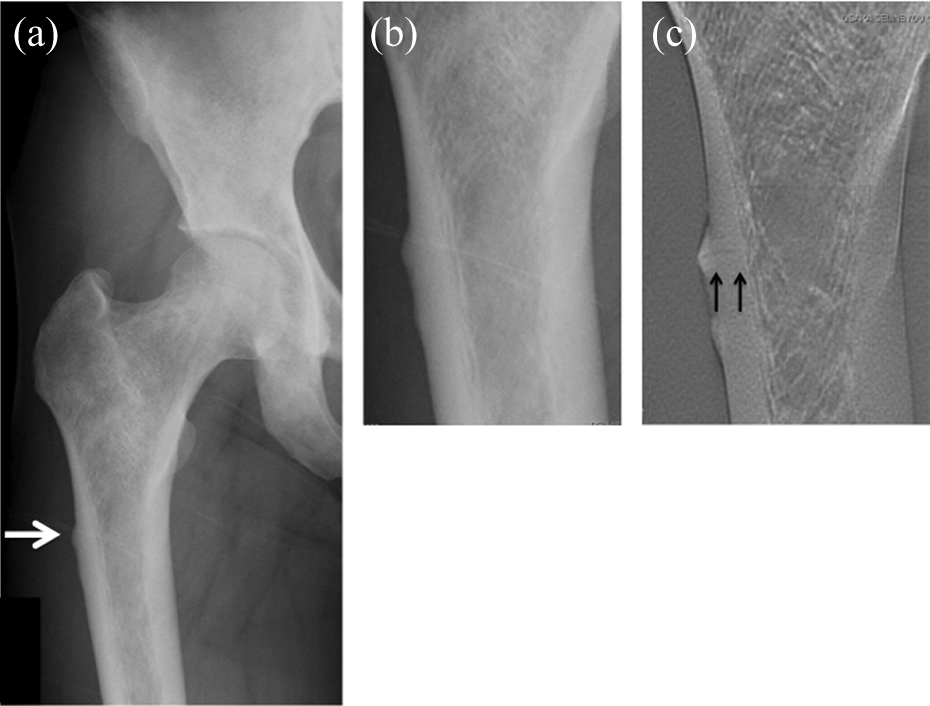
(a) Radiograph showing thickening of the lateral subtrochanteric cortex. (b) A visible fracture line is not observed by radiography. (c) Tomosynthesis showing a visible fracture line at the site of cortical thickening.
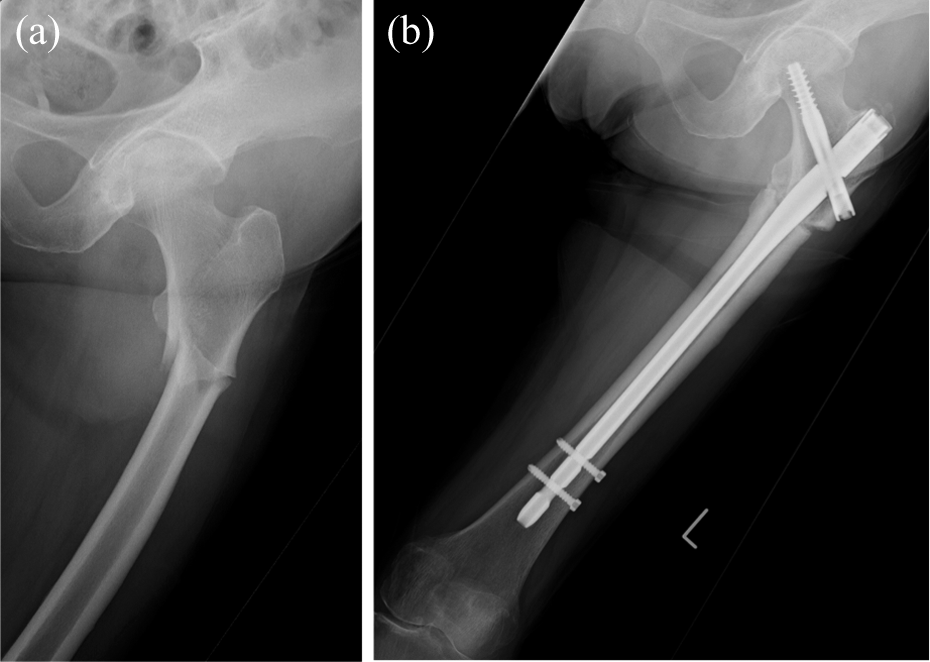
On admission, radiographs showed a complete subtrochanteric transverse fracture in her right femur, which extended through both cortices with a medial spike. She underwent surgery, and an intramedullary nail was placed (Figure 2).

(a) Radiograph showing right femoral subtrochanteric complete fracture. (b) Surgical intervention was achieved with an intramedullary nail.
One month after the surgery, the patient presented with mild pain in her left thigh. Radiographs of the left femur showed slight thickening of the lateral subtrochanteric cortex. Neither radiography nor tomosynthesis showed remarkable fracture lines in the thickened region; however, due to the persistent pain lasting for 1 month, an intramedullary nail was surgically placed to prevent complete fracture that had previously developed on the right side (Figure 3).

(a) Radiograph of the left femur showing slight thickening of the lateral subtrochanteric cortex. (b) A visible fracture line is not observed by tomosynthesis. (c) Surgical prophylaxis was achieved with an intramedullary nail.
Patient 2
The second patient is an 83-year-old woman who had undergone lumpectomy at the age of 71 when she was diagnosed with breast cancer. She had no comorbidity. Three years after the lumpectomy, she was found to have bone metastases on the lumbar vertebrae, and intravenous BP was initiated. Several courses of chemotherapy were administered during BP therapy, specifically tamoxifen, capecitabine, trastuzumab, and fulvestrant. The patient was administered with zoledronate injections at a monthly dose of 4 mg for 9 years when she presented with mild pain in her left thigh without any trauma.
Radiographs of her left femur showed thickening of the lateral subtrochanteric cortex. Tomosynthesis revealed a visible fracture line in the thickened cortex, which was not detected with conventional radiography (Figure 4); therefore, she was diagnosed with incomplete AFF and initially treated with conservative management. Zoledronate was discontinued and low-intensity pulsed ultrasounds were applied. However, she fell down from a standing position and was transferred to our hospital 3 months later.
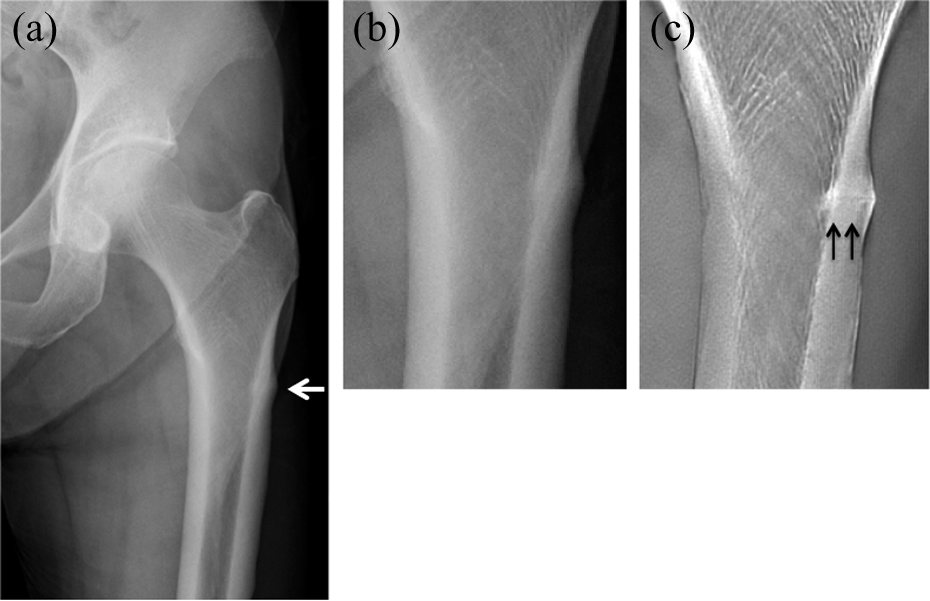
(a) Radiograph showing thickening of the lateral subtrochanteric cortex. (b) A visible fracture line is not observed by radiography. (c) Tomosynthesis showing a visible fracture line at the site of cortical thickening.
On admission, radiographs showed a complete subtrochanteric transverse fracture in her left femur, which extended through both cortices with a medial spike. She underwent surgery, and an intramedullary nail was placed (Figure 5).
(a) Radiograph showing left femoral subtrochanteric complete fracture. (b) Surgical intervention was achieved with an intramedullary nail.
Discussion
Development of effective molecular targeted agents has led to improved overall survival rates in cancer patients. 2 With the consequent increase in incidence rates of bone metastases and associated SREs, the use of BMA is expected to increase in these patients. Thus, in the future, orthopedists should be cognizant of the potential increase in the frequency of AFFs in patients with bone metastases.
Denosumab inhibits the development and activity of osteoclasts and decreases bone resorption by binding to its target, RANKL. 3 Osteoclast numbers were shown to be greatly reduced, with no evidence of ongoing resorption, following the administration of denosumab, which remains in blood for several months after injection. 4 Therefore, because of its molecular mechanisms and pharmacokinetics, denosumab can potentially cause AFFs similar to those observed with most BPs.
The American Society for Bone and Mineral Research (ASBMR) task force described the major and minor defining features of AFF. 5 We did not strictly perform a biopsy only in the bone fracture region, but bone shavings produced while reaming the medullary cavity during the operation were sent for histological examination in both the cases. Cancer cells were found in the specimens of patient 1 and were not found in patient 2. However, when we consider that bone metastases in both femoral shafts were previously detected in patient 1 and we reamed the entire femoral medullary cavity, it is not surprising that cancer cells were found. Based on the clinical history and the presence of all major AFF features, we concluded that the patients presented here were diagnosed not with a pathological fracture but with AFF. These cases were similar to several previous reports of femoral fractures diagnosed as AFFs in patients with bone metastases. 6,7
Several studies demonstrated that AFF might initially appear as a focal or diffuse cortical thickening in the lateral cortex of the subtrochanteric or femoral shaft region. Thereafter, a radiolucent fracture line might appear at the site of cortical thickening, extend medially, and ultimately become a complete fracture. 8,9
Saleh et al. stated that surgical prophylaxis might only be required for incomplete AFFs with radiolucent fracture lines at the sites of cortical thickening in patients with osteoporosis. In that study, nine fractures presented with radiolucent fracture lines, and two patients were successfully managed conservatively, including the human parathyroid hormone teriparatide. Authors also reported that six patients were elected for surgical prophylaxis after 3 months of conservative management, whereas one patient underwent surgical prophylaxis without initial conservative management. 10 In the present cases, the patients initially presented with mild pain in their thighs, and their radiographs showed focal cortical thickening. Tomosynthesis showed a radiolucent fracture line at the site of cortical thickening, which was not observed on radiographs. Therefore, they were initially treated with conservative management; however, the incomplete fracture resulted in a complete fracture following a minor trauma. In the case of patient 1, based on the course of the AFF on the right side, the incomplete fracture that later developed on the left side was treated with surgical prophylaxis.
The clinical courses of the patients presented here implicate two major clinical considerations. First, symptomatic incomplete AFF associated with BMAs prescribed for bone metastases should be treated with surgical prophylaxis due to delayed fracture healing, which is a minor feature of AFF defined by the ASBMR task force. 5 For several reasons, healing of AFF associated with BMAs against bone metastases likely requires an even longer duration than AFF due to osteoporosis. First, teriparatide, which was shown by several studies to advance healing AFF in patients with osteoporosis, is contraindicated in patients with bone metastases. 10,11 Teriparatide was reported to increase the incidence of bone neoplasms, such as osteosarcoma, following long-term administration in rats. 12 Second, BMAs are used in higher doses and more frequently for the prevention of SREs in patients with bone metastases than in patients with osteoporosis. Therefore, potential long-term lasting effects of BMAs after treatment cessation might delay fracture healing. Finally, in certain cases, there are limited alternatives to BMA therapy, especially in patients with high-risk SREs, such as pathological fractures, bone surgery, radiation therapy, and spinal cord compression. In such cases, consensus has not been reached on BMA therapy cessation.
The second clinical implication of this report is the utility of tomosynthesis in the identification of the radiolucent fracture lines at the sites of cortical thickening in AFF associated with BMA therapy for bone metastases. Koh et al. observed that a radiolucent fracture line was a reliable predictor of fracture propagation. 13 Therefore, the presence of a fracture line is an important factor for treatment determination. In the present cases, tomosynthesis showed a fracture line that could not be observed on radiographs, which demonstrated that tomosynthesis might be useful in the diagnosis of AFF associated with BMA therapy for bone metastases.
Conclusion
Surgical prophylaxis should be considered for symptomatic incomplete AFFs associated with BMA therapy for bone metastases, given that fracture healing is expected to require an even longer duration and that an incomplete fracture might potentially progress to a complete fracture during long-term conservative management. Additionally, tomosynthesis is a useful modality to identify radiolucent fracture lines that are reliable predictors of fracture propagation. The number of similar cases is expected to increase with increased use of BMA. Therefore, future studies should investigate whether surgical prophylaxis is beneficial in this patient population and whether routine tomosynthesis might be useful in the identification of the telltale radiolucent fracture line of AFF.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.