
Abstract
Purpose:
The general surgical approach for patellar fractures has a significant weakness, in that the articular facet is invisible because the fixation is performed using radiation amplifiers after exposing the fracture site through vertical or transverse dissection on the anterior patella. We report excellent outcomes in the surgical treatment of patellar fractures, using a medial parapatellar approach.
Methods:
This study evaluated 20 patients who underwent surgery between August 2008 and April 2014 to correct patellar fractures with comminution or with displacement of the articular facet of ≥2 mm and who had ≥1 year of follow-up. Surgery was performed using anatomical reduction with direct exposure of the articular facet of the patella via a medial parapatellar approach. Bone union, severity of displacement, range of motion (ROM) of the patella, and complications were evaluated after surgery, and patellar function was evaluated using the Lysholm knee score.
Results:
Bone union was achieved in all cases, and average displacement of the articular facet decreased from 3.2 mm (range: 1.2–7.3 mm) preoperatively to 0.2 mm (range: 0–0.5 mm) postoperatively. No particular postsurgical complication was observed. All cases had a normal ROM, and the average Lysholm score at final follow-up was 96.2 points.
Conclusion:
Anatomical fixation of the articular facet via a medial parapatellar approach appears to be suitable for patellar fractures, which are intra-articular.
Introduction
A patellar fracture is an intra-articular fracture that may cause traumatic patellofemoral arthritis if the articular facet is not accurately reduced during surgery. It may also result in knee stiffness and reduction of the extensor mechanism in the case of long-term immobilization. 1,2 Although either conservative treatment or partial or total patellectomy was the previously used conventional strategy, the issue of aftereffects and the importance of the patella in the extensor mechanism of the knee joint have since been recognized. 3 Hence, the current trend involves the conservation of as many bone fragments as possible to recover the original length of the patella, even in severe comminuted fractures. Moreover, the performance of open reduction results in a more accurate anatomic reduction of the articular facet, which allows for joint exercises by enabling stable internal fixation, thereby minimizing problematic aftereffects. 4 –6
However, one disadvantage of the general surgical approach for patellar fractures is the lack of visibility of the articular facet when evaluating the reduction. Typically, an image intensifier is used following reduction of the extra-articular portion of the patella using pointed reduction forceps or K-wires, after exposing the site of the patellar fracture via vertical or transverse dissection. 7,8 This method differs from the one that is used for other intra-articular fractures, wherein the reduction state is evaluated by directly observing the articular facet.
Materials and methods
Twenty patients (15 men and 5 women) who underwent surgery for patellar fractures between August 2008 and April 2014 and who had ≥1 year of follow-up were included in this study. This was a retrospective cohort study. The surgical indication for the treatment of a patellar fracture via a medial parapatellar approach was limited to fractures with comminution or with a ≥2 mm displacement of the articular facet. Compression-type fracture was defined as reduction in the thickness of the fracture fragment by more than half of the thickness of the contralateral side on a lateral radiograph. 9 We used a medial parapatellar approach in compression-type cases when the periosteum and retinaculum were relatively intact and the articular portion could not be identified through the fracture site. Patients with other combined fractures were excluded from the study. In cases in which active knee extension was impossible owing to extensor mechanism injuries, only the separation of bone fragments was done, without dislocation of the articular facet. In cases of eminence fracture, which is a type of extra-articular fracture, surgery was performed using established methods involving a vertical incision.
Injuries were caused by traffic accidents involving automobiles or motorcycles in 12 cases, by a fall from a height in 5 cases, and by a fall due to slipping in 3 cases; all cases involved contact trauma that directly injured and damaged the patella. Fracture of the patella was classified as follows, based on the pattern of the fracture and degree of displacement of the articular facet: 12 cases of comminuted fracture, 5 cases of transverse fracture, and 3 cases of longitudinal fracture. Excluding the comminuted cases, the remaining eight were compression fractures. When defining separation, the value was obtained by calculating the average of two distances measured between the two bone fragments (one at the anterior side of one fragment and another at the posterior side of another fragment in the lateral view). Displacement was defined as the anteroposterior distance measured between the articular facets of the two bone fragments. 10 The preoperative lateral radiograph showed an average separation of 4.2 mm (range: 2.0–10.0 mm) and an average displacement of 3.2 mm (range: 1.2–7.3 mm) (Figure 1). 10

Definition of separation and displacement. Separation is defined as “(a + b)/2” and displacement as “c.”
The patients were placed in the supine position under spinal or general anesthesia, while wearing a tourniquet at the proximal femoral region. The skin on the midline of the patella was vertically dissected, followed by vertical dissection from the borderline between the medial one-third and central one-third of the proximal quadriceps femoris muscle, along the direction of the fibers. Following dissection from the midline of the patella to a point 4–5 mm distally, further dissection was continued toward the proximal tibia along the midline. In the case of a severe comminuted fracture of the medial patella or a ruptured patellar tendon, the approach was made through the medial side. The articular facet was then exposed by everting the patella, after which accurate reduction of the articular facet fracture was performed using pointed reduction forceps or K-wires. Fixation was performed using the K-wire (1.5 mm diameter) that was used for reduction by (1) applying tension band wiring for small bone fragments, (2) applying modified tension band wiring with 3.5-mm-thick cannulated screws, using the K-wire as a guide wire for bone fragments with a maximum cross-sectional area of ≥1 cm2, or (3) using either additional K-wires or cannulated screws to fix the comminuted articular facet in the case of severe comminution. The K-wire was used mainly for temporary fixation during surgery, and screws were used in cases where the size of the main fracture fragment was large enough to prevent dislocation of the fragment. At this time, the soft tissue dissection was limited to the extent that the fracture site could be confirmed while preserving the maximum attached soft tissue. Dissection was only performed 2–3 mm distal and proximal to the retinaculum, and the soft tissue adhering to the bone fragment was not damaged.
Straight-leg-raising exercises were allowed from postoperative day 1, and continuous passive motion (CPM) exercises were allowed from postoperative day 2. CPM exercises were performed until the active range of motion (ROM) of the knee joint reached 90°. Postoperative weight bearing was performed as soon as possible with both straight-leg-raising and quadriceps muscle-strengthening exercises. If the patient experienced pain at the time of weight bearing, then a crutch was used for assistance.
Follow-up was performed at 1 month, 3 months, 6 months, and 1 year after surgery. Statistical significance was evaluated (Wilcoxon signed-rank test) by measuring and comparing the pre- and postoperative degrees of articular facet displacement on the lateral radiographic view. Level of statistically significant difference was set at p < 0.05. The degrees of displacement were defined as follows: A smooth articular facet with a displacement of ≤1 mm was considered excellent, a displacement of 1–2 mm was good, a displacement of 2–3 mm was fair, and a displacement of > 3 mm was poor. Bone union relative to initial severity of displacement, ROM of the patella, and complications were radiologically evaluated after surgery, and patellar function was evaluated using the Lysholm knee score.
Results
The average duration of postsurgical follow-up was 18 months (range: 12–32 months). Bone union was achieved in all cases, and the average time required for bone union was 12.7 weeks (range: 10–17 weeks). Maximum knee joint flexion was considered to be 140° and was achieved within 1 week of surgery in all 8 transverse and longitudinal fracture cases, and within an average of 3 weeks (range: 2–4 weeks) after surgery in the 12 comminuted fracture cases. The final follow-up revealed full recovery of maximum flexion of 140°, with a flexion limitation of 0° in all cases. Complications such as avascular necrosis (AVN) of the patella; limitations in the ROM of the knee joint; nonunion; loss of fracture reduction; irritation due to implants, dissociation, and translocation of the implants; and infection were not observed in any cases (Figures 2 to 5). Similarly, postsurgical separation of the articular facet was not found in any cases. The lateral radiographs revealed reduction (p = 0.001, Wilcoxon signed-rank test) in the average displacement from 3.2 mm (preoperative value; range: 1.2–7.3 mm) to 0.2 mm (postoperative value; range: 0–0.5 mm). Therefore, an excellent outcome, including a smooth articular facet with a displacement of ≤1 mm, was achieved in all cases (Figures 2 to 5). At the final follow-up, the average Lysholm knee score was 96.2 points (range: 90–100 points).

A 69-year-old man with displacement of ≥3 mm and intra-articular fracture observed on radiographs and computed tomography at the time of the visit for a pedestrian traffic accident.

(a) Exposure of the fracture site using a medial parapatellar approach and (b) anatomical reduction of the articular facet using pointed reduction forceps.

Postsurgical anteroposterior and lateral radiographs.
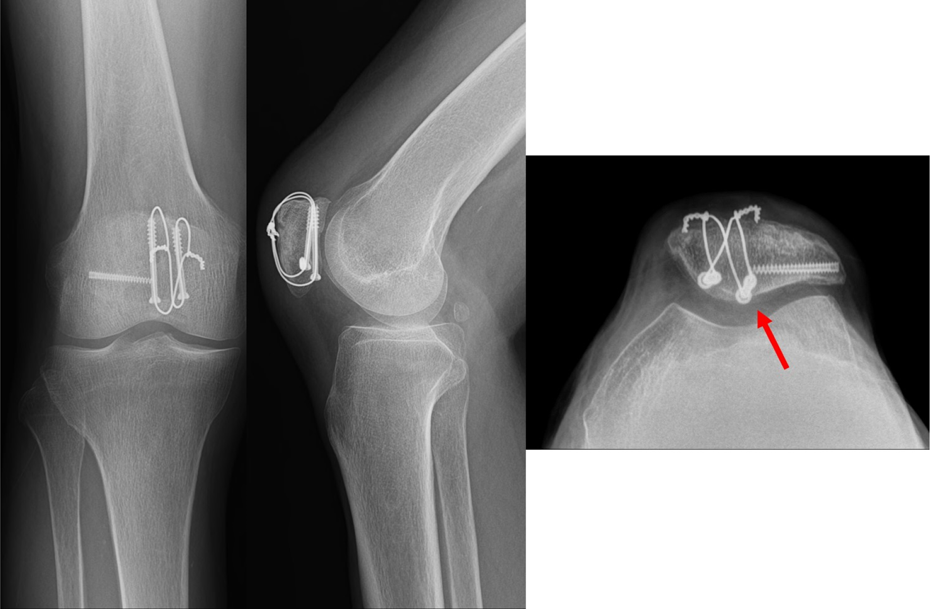
Anteroposterior, lateral, and Merchant view radiographs taken 6 months after surgery show strong subchondral bone fixation of the screws (red arrow).
Discussion
In this study, patellar fractures with intra-articular comminution and displacement showed good clinical and radiological results, using a medial parapatellar surgical approach. This approach is used for total knee replacement. The advantages of this approach include easy eversion of the patella and easy access to the articular facet owing to a wide visual field. 11 –13 Furthermore, instrument implantation into the articular facet can be assessed while inserting the K-wire and cannulated screws, after the articular facet is accurately reduced, direct stable fixation to the subchondral bone can then be achieved.
Moreover, this anterior approach can reduce implant irritation as theorized in many studies. 14 –16 This approach makes it possible to insert the implant deep into the subchondral bone, thereby reducing irritation. Therefore, there was no irritation in any of the 20 cases. Two patients requested implant removal, which was accomplished without difficulty using the same approach.
The extensor mechanism is known to be weakened by injury to the medial superior and descending genicular artery during dissection of the quadriceps femoris muscle and patella and can be considered a disadvantage of the medial parapatellar approach. However, no AVN or weakening of the extensor mechanism due to arterial injury was observed in this study. This may be explained by (a) a careful approach to the ligament region of the quadriceps femoris, (b) relatively intact periosteum and retinaculum using this approach to a compression-type fracture, (c) complete suturing of the ligament of the quadriceps femoris and patella during surgery, and (d) allowing continuous rehabilitation exercise. In addition, we limited surgery for patellar fractures to the stated indications.
One specific technique that can be performed through the wound involves the temporary maintenance of reduction using pointed forceps, after the bone fragments are reduced by touching the articular facet either directly or indirectly; exposure of the articular facet by dissection of the lateral retinaculum has been reported. 17 In addition, the reduction can be evaluated using arthroscopy. 18 However, such a method has limited ability to evaluate the suitability of reduction, since the evaluation is performed indirectly. In comminuted fractures, the accuracy of reduction cannot be determined using an approach through the wound or partial dissection of the retinaculum. In addition, the blood supply to the patella may be a consideration in a lateral parapatellar approach to internal fixation. 19 However, this method involves difficult inversion in the fixation of the patella.
Study limitations include the small number of patients, possibly leading to inaccurate results; furthermore, a control group using other approaches to a patellar fracture could not be prospectively analyzed. In addition, the mean follow-up period was 18 months, which was insufficient to evaluate patellofemoral arthritis after fracture.
Conclusions
In comminuted patellar fractures with displacement of the articular facet and in compression-type patellar fractures, an excellent treatment outcome can be achieved by performing accurate reduction while directly observing the articular facet of the patella via a medial parapatellar approach.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.