
Abstract
Objectives:
To analyze the clinical efficacy and cement leakage rate of percutaneous kyphoplasty (PKP) for the treatment of metastatic vertebral lesions between the two groups using different cement infusion techniques.
Methods:
One hundred twenty-nine patients (160 metastatic vertebral fractures) who chose “the incremental temperature cement delivery technique” (ITCDT group) and 105 patients (128 metastatic vertebral fractures) who chose “traditional infusion technique” (TI group) were finally enrolled (nine patients were lost to the follow-up). The visual analog scale (VAS), Oswestry Disability Index (ODI), the local Cobb’s angle, the relative height of the vertebral anterior border, and cement leakage were analyzed to evaluate the clinical efficacy of the two cement infusion techniques within postoperative 12 months.
Results:
There was no significant difference in the VAS scores, ODI scores, the relative height of the vertebral anterior border, and local Cobb’s angle between the ITCDT group and TI group preoperatively and postoperatively (p > 0.05). The cement leakage occurred in three patients of ITCDT group (2.3%), which was significantly less than TI group (12 patients, 11.4%; p < 0.05).
Conclusions:
The ITCDT and TI technique in kyphoplasty are effective at relieving pain and improving functional disability, vertebral height, and kyphosis angle; However, kyphoplasty using the ITCDT causes less cement leakage significantly.
Introduction
Up to 40% of cancer patients develop spinal metastases depending on primer tumor, including breast (21%), lung (14%), prostate (8%), renal (5%), gastrointestinal (5%), and thyroid (3%) cancers. 1 –3 Spinal metastases of which 70% are located in the thoracic spine, 20% in the lumbar spine, and 10% in the cervical spine. 4,5 After vertebrae were invaded, growth factors that stimulate osteoblastic and osteolytic activities and local cancer cell proliferation can cause symptomatic pain, mechanic instability, neurological dysfunction, sphincter control failure, hypercalcemia, and pathological fractures. 6,7 Percutaneous kyphoplasty (PKP) is reported as an available measure of pain relief for the treatment of painful metastatic vertebral lesions, due to regaining the height of metastatic vertebral body and stability of spinal column, destroying the sensory nerve endings, and killing the tumor cells by chemical and exothermic reaction of the cement. 8,5
Cement leakage is the most common complication in PKP. As is reported, the leakage rate can be 4.8–39%. 9 –13 Approximately 73% of the clinical complications are associated with the leakage. 14,15 To our knowledge, the incidence rate of cement leakage for the treatment of metastatic vertebral lesions using PKP may be higher than for osteoporotic vertebral compressive fracture (OVCF), which may result from more severe fractured vertebrae or irregular worm-eaten intravertebral lesions. 16 –18 Once the cement remote into the spinal canal or vital vessels, severe outcomes will occur, including paralysis, pulmonary embolism, and even death. The cement leakage is related to many factors, such as inappropriate puncture, balloon placement, and cement infusion, of which the safe and effective infusion technique is very important. 15 To decrease the incidence rate of cement leakage, we summarized a new infusion technique called the incremental temperature cement delivery technique (ITCDT). In the study, we aimed to retrospectively analyze the clinical efficacy and cement leakage rate of PKP for the treatment of metastatic vertebral lesions between the two groups (traditional infusion (TI) group and ITCDT group).
Materials and methods
Clinical study design
The study was designed as a single-center retrospective research comparing “ITCDT group” and “TI group.” The protocol was approved by the local ethics committee. Informed consent was obtained from all individual participants included in the study.
Two hundred thirty-four patients who suffered from metastatic vertebral lesions and had accepted PKP surgeries from January 2008 to September 2015 in our hospital were finally enrolled. The 129 patients were treated using ITCDT (including breast cancer (n = 53), lung cancer (n = 49), prostate cancer (n = 8), stomach cancer (n = 6), liver cancer (n = 3), rectal cancer (n = 5), cervical cancer (n = 2), renal cancer (n = 2), and ovarian cancer (n = 1), and two patients (breast cancer and lung cancer) were lost to the follow-up). The 105 patients were performed by “TI technique’ (including breast cancer (n = 44), lung cancer (n = 41), prostate cancer (n = 6), stomach cancer (n = 5), liver cancer (n = 2), rectal cancer (n = 3), renal cancer (n = 3), and ovarian cancer (n = 1), and seven patients (three breast cancer, three lung cancer, and one ovarian cancer) were lost to the follow-up). All patients received preoperative or intra-operative biopsy. The patients must meet all the inclusion criteria to participate in the research: (1) the patients did not improve the pain complaint for at least 3 weeks of chemotherapy, radiotherapy, or conservative treatment; (2) patients suffered from metastatic vertebral fractures; (3) magnetic resonance imaging (MRI) showed hypointensity on T1 sequence, hyper or mixed intensity on T2 sequence, and hyperintensity on short-time inversion recovery sequence. Contrast-enhanced MRI revealed hyperintensity in the metastatic fractured vertebrae. If MRI examination was unavailable, the vertebral bone scan should indicate the high uptake of radionuclide. The exclusion criteria includes the following: (1) the dural sac was obviously compressed or nerve injury due to the retropulsion of vertebral fracture; (2) OVCFs; (3) patients with coagulopathy; and (4) patients had serious medical or psychiatric illness. Patient demographic data are showed in Table 1.
Summary of patient demographics.

Methods
For both two groups, the patients were punctured bilaterally after general anesthesia. After successful puncture, the balloon was placed in the middle 1/2 of the vertebra through the working casing. The polymethylmethacrylate (PMMA) bone cement was injected in the two different ways: The ITCDT group (interval infusion technique): (1) Temperature: the temperature of operating room was set up to 20°C. (2) Infusion time: the cement infusion was started when the cement became doughy and did not stick to the surgeon’s rubber gloves, which meant the cement viscosity was a little high. (3) Interval infusion: The higher the temperature was, the faster the cement solidified. Therefore, the solidification of cement in the vertebral body (37°C) was much faster than that in the operating room (20°C). ITCDT used the temperature gradient characteristic to inject cement into the vertebral body intermittently. Firstly, the cement was injected at the broken border of fractured vertebrae, 1–2 min later, nearly solidified cement formed the artificial vertebral wall to prevent from cement leakage. Then, the remaining cement was injected into the cavity of vertebral body. TI group (single infusion technique): (1) Temperature: the temperature of operating room was set up to 20°C. (2) Infusion time: the cement infusion was started when the cement was mixed, which meant the cement viscosity was low. (3) Single infusion: the cement was slowly injected into cavity of vertebral body at one time.
All procedures were performed under live fluoroscopy. After the infusion, the wound was compressed and sutured for hemostasis. The second day after surgery, the patients were allowed to walk under the protection of the waist.
Outcome measures
At preoperative, postoperative 1 week, and postoperative 1 year, visual analogue scale (VAS) and Oswestry Disability Index (ODI) were used to evaluate patient pain relief and functional improvement status. The local Cobb’s angle and the relative height of the vertebral anterior border (the anterior border height of fractured vertebrae/the average anterior border height of adjacent vertebra) were measured through postoperative X-ray. The cement leakage was judged by postoperative X-ray or computed tomography scans.
Statistical analysis
All the data were presented as x ± s. Independent samples t-test and χ 2 test were conducted in this study. p < 0.05 was considered statistically significant. All statistical analyses were performed with SPSS 13.0 for Windows (SPSS, Chicago, Illinois, USA) and Microsoft Excel 2003 (Microsoft, Seattle, Washington, USA).
Results
Clinical evaluation
The VAS scores and ODI scores were not statistically different in the comparison between two groups among the preoperative and postoperative scores and ones at the last follow-up (p > 0.05; Table 2).
Clinical evaluation.a

aThe last follow-up was 12 months after surgery.
Radiologic evaluation
There was no significant difference in the relative height of the vertebral anterior border and local Cobb’s angle before and after surgery and at final follow-up (p > 0.05; Table 3).
Radiologic evaluation.a

aThe last follow-up was 12 months after surgery.

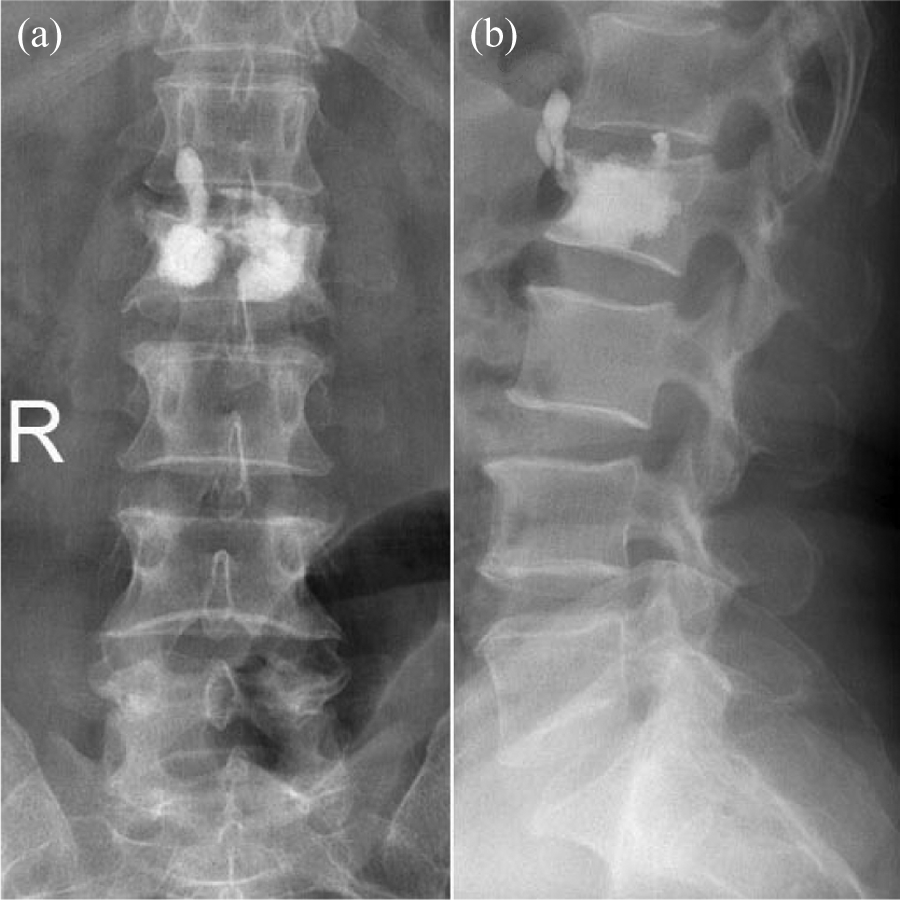
Anteroposterior and lateral X-ray (a and b) after L4 kyphoplasty using the ITCDT. The cement injected to anterior border of vertebral body firstly formed an artificial wall, so that the ITCDT performed interval cement infusion to prevent from cement leakage. ITCDT: incremental temperature cement delivery technique.
Anteroposterior and lateral X-ray (a and b) after L2 kyphoplasty using the TI technique. The low-viscosity cement was injected to the cavity of vertebral body at one time. The single infusion may case cement leakage. TI: traditional injection.
Complication occurrence
The cement leakage rate in ITCDT group was 2.3% (3/129). One case leaked through the lateral side of the vertebrae, and the other two cases leaked into intervertebral disc with no clinical symptoms. The cement leakage rate in TI group was 11.4% (12/105). Six cases leaked into intervertebral disc, eight cases leaked through peripheral vertebral wall, and one case of pulmonary embolism, which showed no obvious clinical symptoms. The leakage rate of the ITCDT was significant lower than that in TI group (χ 2 value = 4.641, p < 0.05).
Discussion
Lieberman published the first follow-up report of PKP. 19 A total of 30 cases of OVCF patients, including 70 fractured vertebrae, were investigated, of which the cement leakage rate was 8.6%. In 2006, a systematic analysis of 69 clinical studies showed the leakage rate of PKP was 9%. 14 In 2008, a meta-analysis of 168 studies 20 indicated that PKP leakage rate was 7.0%. The meta-analysis by Lee et al 15 reported the leakage rate of 14%. However, for metastatic vertebral fractures, the risk of cement leakage may be higher. Puffer et al. reported that the range of cement leakage in PKP for malignant vertebral compressive fractures may be 0–21.8%. 21 Fourney et al. reported a direct comparison on the treatment of timorous lesions with vertebraoplasty and kyphoplasty in 56 patients undergoing 65 vertebroplasties and 32 balloon kyphoplasties. Cement leakage was observed in 9% of vertebraplasties and 0% of balloon kyphoplasties. 22 Pflugmacher et al. reported a 2-year prospective evaluation for PKP in the treatment of metastatic vertebral lesions; the cement leakage rate of which revealed 12%. 16 Generally speaking, the linear and the strip leakage are the main forms of cement leakage. 23 The cement may be leaked through the breakage of cortical vertebrae, the basilar vein, or the intervertebral vein. 24
The vertebral status, the standard position, definition of radiological images, the puncture procedure, and the infusion methods are relevant factors which might cause cement leakage in PKP. We started the researches of PKP for OVCF since October 1999. Nowadays, we find out the infusion technique which may effectively reduce leakage of cement, that is, the ITCDT. The key points are as follows: (1) The best infusion time of cement is the late drawing stage or early slug stage, which could make cement diffuse well instead cause leakage. Clinically, we suggested the infusion time when the cement did not stick to the rubber gloves. (2) The ITCDT (interval infusion technique): The cement solidification rate is closely related to the ambient temperature. The higher the temperature is, the faster the cement solidifies. The temperature of operating room is generally 20°C, while the body temperature is nearly 37°C. In the vertebrae, the solidification of cement is much faster than that in the operating room. We injected the cement at the broken border of fractured vertebrae at first time. After 1–2 min, nearly solidified cement formed the artificial vertebral wall to prevent from cement leakage. After that, we continued to inject the remaining cement in order to finish the vertebral augmentation. (3) If necessary, mix of cement can be separated into several times. Small amount of cement could be mixed first, which was injected into the vertebral body to block the broken peripheral wall of the vertebrae, after the completely solidification, we begin to mix the cement and inject the cement again. In that way, the cement leakage will be significantly reduced.
The results of our study show that there were no significant differences in the VAS scores, ODI scores, the local Cobb’s angle, and the relative height of the vertebral anterior border between the ITCDT and TI group. However, cement leakage rate is only 2.3% in the ITCDT, significantly lower than that of 11.4% in TI group. We believe the new technique is compliance with the characteristics of cement solidification. The research by Wu et al. 25 also showed the staged infusion procedure during percutaneous vertebroplasty (PVP) could reduce the incidence of cement leakage. Since our study is not a randomized controlled study, the strict inclusion and exclusion criteria could reduce the selection bias. 26,27
Conclusion
According to the results, compared with the TI technique, the ITCDT leads to lower incidence of cement leakage while it shows no difference in clinical and radiological evaluation.
Footnotes
Author contribution
The authors Hao Liu and Shenghao Wang contributed equally to this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.